Giant Antrochoanal Polyp-A Rare Presentation
Swati Kodur1, Shruti Malavalli Siddappa2, Andanooru Mahalingappa Shivakumar3
1 Senior Resident, Department of Ear Nose and Throat, S.S. Institute of Medical Sciences and Research Centre, Davanagere, Karnataka, India.
2 Postgraduate Student, Department of Ear Nose and Throat, S.S. Institute of Medical Sciences and Research Centre, Davanagere, Karnataka, India.
3 Head, Department of Ear Nose and Throat, S.S. Institute of Medical Sciences and Research Centre, Davanagere, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Swati Kodur, No. 3065/2, 8th Main, 4th Cross, MCC B Block, Davanagere-577005, Karnataka, India.
E-mail: drswatikodur@gmail.com
Antrochoanal polyp (ACP), also called as Killian polyp, is an infrequent, benign lesion of maxillary origin in non-atopic patients. The antrochoanal polyp is shaped according to the anatomical constraints of the lateral nasal wall, particularly the middle meatus and antrum, resembling typically a dumbbell. Here presenting a common problem with unusual presentation.
Dysphagia, Giant nasal polyp, Maxillary sinus
Case Report
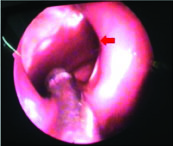
A 36-year-old male presented to the outpatient department with complaint of difficulty in swallowing associated with foreign body sensation in the throat since two months. Patient gave history of difficulty in speech which was also started during the same time period and occasional right sided nasal obstruction, more so during an episode of upper respiratory tract infection. The patient reported, having previously being healthy and had no history of allergy. During examination of the throat we noticed a large, pale, polypoidal mass making appearance from the nasopharynx through the hypopharynx. The mass was noticed to be mobile when moved with a tongue depressor however the lower end of the mass was not clearly made out [Table/Fig-1]. On anterior rhinoscopic examination, patient was noted having a deviation of septum to left with no other positive finding. Examination of ear was normal. Nasal endoscopy revealed that the mass arose from the right middle meatus and extented into the nasopharynx with concha bullosa of right middle turbinate.
Polyp (red arrow) seen projecting from the naspharynx extending down to the hypopharynx.

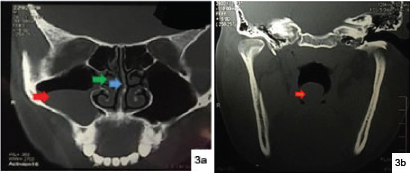
Computed tomography (CT) images demonstrated a pedunculated soft tissue mass seen extending through the maxillary ostium into the nasopharynx and through the hypopharynx, nasal septal deviation to left, concha bullosa of the right middle turbinate. [Table/Fig-2,3a,b]
Axial view of CT PNS -homogenous opacity (red arrow) seen occupying the right maxillary sinus extending the nasopahrynx (green arrow)
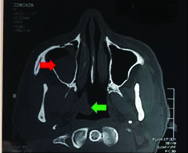
a) Coronal view of CT PNS-homogenous opacity in the right maxillary sinus (red arrow), concha bullosa (green arrow) of the right middle turbinate with deviation of septum to the left (blue arrow); b) Coronal view CT PNS-posterior view of coronal view showing extension of the polyp downwards into to hypopharynx (red arrow).
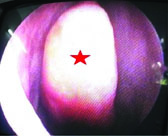
Under general endotracheal anaesthesia, evaluation of the right nasal cavity confirmed that the mass was arising from the right maxillary ostium, extending posteriorly through a stalk to the nasopharynx. Concha bulloplasty [Table/Fig-4,5] was performed to make room for further procedure.
Intraoperative image of right middle turbinate showing concha bullosa (red asterisk).
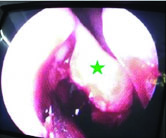
Intraoperative image of right middle turbinate (green asterisk) after concho bulloplasty.
After uncinectomy, stalk of the polyp was identified protruding from the natural maxillary sinus opening [Table/Fig-6], which was then separated from the intra antral part and delivered through intraoral route [Table/Fig-7].
Intraoperative image of stalk of the polyp (blue asterisk) emerging out of the right maxillary sinus opening.

Intraoperative image of polyp (red asterisk) extraction through the inta oral root.green asterisk indicating the soft palate. (Images left to right)

A 8x3 cm polyp was removed. The base of the polyp was then removed from the antrum followed by widening of the natural maxillary ostium [Table/Fig-8,9].
Measurements of the giant antrochoanal polyp after removal.

Postoperative picture of the widened maxillary sinus opening (red arrow).
Hemostasis was maintained throughout the procedure. Patient tolerated the procedure well. Nasal pack was removed after 48 hours Patient has experienced relief from the complaints within one month of postoperative follow up.
Discussion
Antrochoanal polyp was first reported by Palfyn in 1753 [1], although Killian G, was the first to describe this disease in detail in 1906 [2]. In contrast to inflammatory nasal polyposis, which grows from the ethmoid cells [3], an antrochoanal polyp is a benign lesion originating from the oedematous mucosa of the maxillary sinus, growing through the main or accessory ostium which is usually enlarged [4] into the middle meatus and protruding posteriorly to the choana and nasopharynx constituting 4-6% of all nasal polyps [5].
Although unknown, chronic inflammation of sinus, congenital deformities in sinus drainage has been considered in the aetiopathogenesis.
Clinical manifestations usually start with unilateral nasal obstruction, although there are reports of cases starting with epistaxis, purulent rhinorrhea, polyp strangulation, spontaneous amputation, dyspnea and dysphagia, falling into the hypopharynx, occupying the mouth to produce dysphagia and speech disturbances, and obstructive sleep apnea and cachexia [6].
Nasal endoscopy, CT scan and Magnetic Resonance Imaging (MRI) are the core diagnostic techniques used in diagnosis of nasal polyposis. An antrochoanal ployp protruding through the maxillary infundibulum or accessory ostium into the middle meatus and then the posterior choana, with possible extension into the posterior nasopharynx [7] is hypodense on CT, hypointense on T1-weighted and hyperintense on T2-weighted MR images, with peripheral contrast enhancement [8].
Differential diagnosis includes ethmoidochoanal polyp, turbinate hypertrophy, adenoidal hypertrophy, Tornwaldt’s cyst, angiofibroma, inverted papilloma [9], in a rare presentation olfactory neuroblastoma, Wegener’s granulomatosis, rhabdomyosarcoma. Diagnosis of antrochoanal polpy can be made with careful history taking, evaluation with endoscopy and radiographic examinations.
Currently recommended treatment is surgical removal of the polyp through endoscopic sinus surgery. The endoscopic technique consists of an uncinectomy and resection of the polyp and its attachment to the maxillary wall [10]. Endoscopic removal of the antral portion of an antrochoanal polyp by powered instrumentation, an alternative to other methods for removing the antral portion of an antrochoanal polyp, is associated with excellent outcomes and minimal morbidities [4]. Caldwell-luc antrostomy used for many years, have been relegated in favor of endoscopic sinus surgery as it was noticed to cause damage to the growth centers of the maxillary bone and dental germs, cause cheek or tooth inflammation and/or anaesthesia [11].
Conclusion
Antrochoanal polyp though a common lesion can present with unusual symptoms and extension into the hypopharynx.
Surgical management with middle meatal antraostomy proved to be a safe option with less post operative morbidity.
[1]. Palfyn J, Anatomie Chirurgicale 1753 Paris [Google Scholar]
[2]. Killian G, The origin of choanal polypiLancet 1906 2:81-82. [Google Scholar]
[3]. Larsen PL, Tos M, Origin of nasal polyposisLaryngoscope 1991 101:305-12. [Google Scholar]
[4]. Hong SK, Min YG, Kim CN, Byun SW, Endoscopic removal of the antral portion of antrochoanal polyp by powered instrumentationLaryngoscope 2001 111(10):1774-78. [Google Scholar]
[5]. Cetinkaya EA, Giant antrochoanal polyp in an elderly patient: Case reportActa Otorhinolaryngologica Ital 2008 28:147-49. [Google Scholar]
[6]. Maldonado M, Martínez A, Alobid I, Mullol J, The antrochoanal polypRhinology 2004 42:178-82. [Google Scholar]
[7]. Towbin R, Dunbar JS, Bove K, Antrochoanal polypsAJR Am J Roentgenol 1979 132:27-31. [Google Scholar]
[8]. Branstetter BF, Weissman JL, Role of MR and CT in the paranasal sinusesOtolaryngol Clin North Am 2005 38:1279-99. [Google Scholar]
[9]. Lopatin A, Bykova V, Piskunov G, Choanal Polyps: One entity, one surgical approach?Rhinology Jun 1997 35:79-83. [Google Scholar]
[10]. Stammberger H, Hawke M, Essentials of functional endoscopic sinus surgerySt LouisMosby:103-05. [Google Scholar]
[11]. Basak S, Karaman CZ, Akdilli A, Metin KK, Surgical approaches to antrochoanal polyps in childrenInt J Pediatr Otolaryngol 1998 46:197-205. [Google Scholar]