Biometrics of Pyramidalis Muscle and its Clinical Importance
Sushant Swaroop Das1, Sandeep Saluja2, Neelam Vasudeva3
1 Senior Resident, Department of Anatomy, Maulana Azad Medical College, New Delhi, India.
2 Assistant Professor, Department of Anatomy, G S Medical College and Hospital, Hapur, Uttar Pradesh, India.
3 Director, Professor and Head, Department of Anatomy, Maulana Azad Medical College, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sushant Swaroop Das, Department of Anatomy, MAMC, BSZ Marg, New Delhi-110002, Delhi, India.
E-mail: susvick@gmail.com
Introduction
Pyramidalis is classified as a vestigial muscle which is frequently present. It is muscle of the anterior abdominal wall. It is thought to tense the linea alba. It has been used as a surgical landmark, source of muscle stem cells and in various surgical procedures.
Aim
The aim of this study was to describe the morphometry and morphology of pyramidalis muscle in an adult Indian population and its correlation with the clinical significance.
Materials and Methods
A cadaveric study on 25 formalin fixed cadavers (males-17, females-8) was conducted in context with prevalence, morphology and morphometry of pyramidalis muscle. Statistical analysis was done using the Chi-Square test and student’s t-test using SPSS version 23.
Results
The pyramidalis muscle was present in 92% cases, usually bilaterally (72%) than unilaterally (20%) and more frequently in males (94.11%) than in females (87.5%). This study was conducted in Department of Anatomy, Maulana Azad Medical College, New Delhi, India from August 2014 to August 2016. Bilateral asymmetry was reported. The mean length of the muscle in males and females was 52.21±14.32 and 50.13±13.62mm on the right and 53.97±15.11 and 51.22±13.78mm on the left side. No significant gender predominance existed on the right and left-sided pyramidalis lengths. The mean width of the right-sided pyramidalis in males and females was 18.35±5.15 and 17.05±4.99mm and the left-sided was 17.8±4.80 and 16.21±4.23mm without gender dimorphism. The mean thickness of the right-sided pyramidalis in males and females was 4.91±1.33 and 4.53±1.29mm and the left-sided 4.33±1.28 and 4.38±1.27mm without gender differences. The mean pyramidalis-puboumbilical index was 35.15±4.38%, 36.01±4.97% in males and females respectively. No anatomical variations with regard to origin and insertion were seen.
Conclusion
This study provides valuable information on pyramidalis muscle which may help in appropriate understanding of anatomy, functions and clinical significance of the muscle.
Linea alba, Morphometry, Rectus sheath
Introduction
Pyramidalis is a small triangular muscle located anterior to the lower part of rectus abdominis muscle within the rectus sheath. It is attached by tendinous fibres to anterosuperior margin of pubis and by the ligamentous fibres in front of the pubic symphysis. The muscle decreases in size as it runs upwards and ends as a pointed apex that is attached to the linea alba midway between umbilicus and pubis but can extend to a higher level. It is innervated by a small branch of the subcostal nerve. Pyramidalis is supplied by branches of the inferior epigastric artery [1,2].
The defined function of pyramidalis muscle is vague, but it is thought to tense the linea alba [1,2]. Many authors have related the pyramidalis muscle with erection of the penis or assumption of upright posture in humans [3]. In making longitudinal incision for a classical caesarean section, the pyramidalis muscle is used to determine the midline and location of the linea alba [4]. Furthermore, after long-term cryopreservation, pyramidalis muscle specimens have been used as a source of striated muscle stem cells for the treatment of post-prostatectomy stress urinary incontinence [5]. Thus, its presence and the knowledge are of vital anatomical and clinical significance.
It varies considerably in size and may be larger on one side than on the other, sometimes absent on one or both sides, or occasionally doubled [1]. The incidence of this muscle also varies greatly with sex and race. So, the present study was undertaken to explore the morphological and morphometric diversity of the pyramidalis muscle.
Materials and Methods
The present study was conducted on 25 (17 males and 8 females) embalmed cadavers in the age group 35-60 years in the Department of Anatomy, Maulana Azad Medical College, New Delhi, India from August 2014 to August 2016. The cadavers with injury scars or surgery marks on abdominal wall were excluded from the study. During dissection of anterior abdominal wall, anterior wall of rectus sheath was reflected laterally to expose the pyramidalis muscle on the lower part of rectus abdominis muscle. Following variables were studied: Presence of pyramidalis muscle; total muscle length; width and thickness of the muscle; presence of any morphological variation of the origin and insertion of the muscle. The width and thickness was measured at the mid-point of the muscle. Measuring tape and digital vernier caliper were used for measurements. Pyramidalis- puboumbilical index which is the percentage of distance between pubic symphysis and umbilicus into which the pyramidalis extends (length along the medial border) was also determined.
Statistical Analysis
Statistical analysis was performed using the Chi-Square test for nominal categorical data and Student’s t-test for normally distributed continuous variables in SPSS version 23 to assess the relationship between the examined variables. A level of significance of p < 0.05 was used. All the observations and results were tabulated and compared with previous studies.
Results
The results of various biometric data of pyramidalis muscle is summarised in [Table/Fig-1,2,3 and 4]. Pyramidalis muscle was present in 23 (92%) cases. Out of which in 18 cases (72%) (13 males (76.47%), 5 females (62.5%)) it was bilaterally present, in 2 cases (8%) {1 male (5.88%), 1 female (12.5%)} it was bilaterally absent, in 3 cases (12%) {2 males (11.76%), 1 female (12.5%)} it was unilaterally present on right side and in 2 cases (8%) {1 male (5.88%), 1 female (12.5%)} it was unilaterally present on left side [Table/Fig-1,5]. No anatomical variations related to origin or insertion of muscle was seen. The average value of total muscle length, width and thickness of muscle are depicted in [Table/Fig-2,3 and 4] respectively. The mean pyramidalis-puboumbilical index was 35.15±4.38%, 36.01±4.97% in males and females respectively [Table/Fig-2]. No anatomical variations with regard to origin and insertion were seen.
Prevalence of pyramidalis muscle.
| Total | Male (n=17) | Female (n=8) | p-value |
|---|
| Bilaterally present | 18 (72%) | 13 (76.47%) | 5 (62.5%) | 0.47 |
| Bilaterally absent | 2 (8%) | 1 (5.88%) | 1 (12.5%) | 0.57 |
| Unilaterally present on right side | 3 (12%) | 2 (11.76%) | 1 (12.5%) | 0.96 |
| Unilaterally present on left side | 2 (8%) | 1 (5.88%) | 1 (12.5%) | 0.57 |
Measurement of length of pyramidalis muscle.
| Side | Male | Female | p-value between male and female of same sides |
|---|
| Range (mm) | Mean±Standard deviation (mm) | Range (mm) | Mean±Standard deviation (mm) |
|---|
| Right | 29.52 - 78.31 | 52.21±14.32 | 32.93 - 69.62 | 50.13±13. 62 | 0.89 |
| Left | 28.61 - 78.99 | 53.97±15.11 | 33.75- 70.83 | 51.22±13.78 | 0.92 |
| p-value between right and left side | 0.98 | 0.95 |
| Pyramidalis- Puboumbilical Index | 30.12% – 42.03% | 35.15±4.38% | 31.09%– 43.68% | 36.01±4.97% |
Measurement of width of Pyramidalis muscle.
| Side | Male | Female | p-value between male and female |
|---|
| Range (mm) | Mean±Standard deviation (mm) | Range (mm) | Mean±Standard deviation (mm) |
|---|
| Right | 12.38-25.91 | 18.35±5.15 | 10.56-24.77 | 17.05±4.99 | 0.81 |
| Left | 10.33-24.34 | 17.8±4.80 | 9.51 – 23.93 | 16.21±4.23 | 0.88 |
| p-value between right and left side | 0.78 | 0.56 |
Measurement of thickness of Pyramidalis muscle.
| Side | Male | Female | p-value between male and female |
|---|
| Range (mm) | Mean (mm) | Range (mm) | Mean (mm) |
|---|
| Right | 3.37-6.76 | 4.91±1.33 | 3.49-5.99 | 4.53±1.29 | 0.54 |
| Left | 3.52-6.82 | 4.33±1.28 | 3.31- 5.86 | 4.38±1.27 | 0.77 |
| p-value between right and left side | 0.47 | 0.59 |
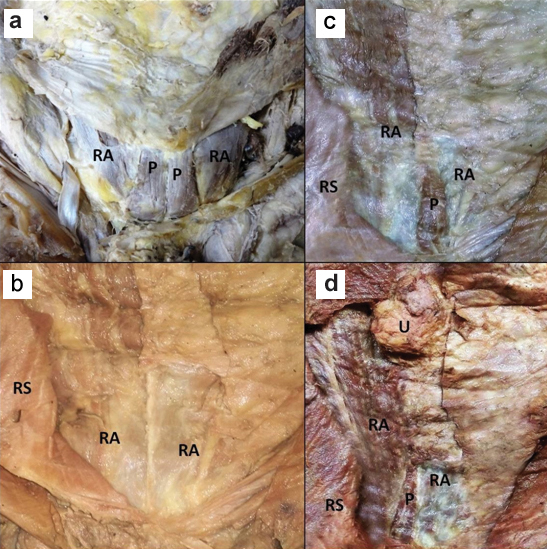
Lower part of anterior abdominal wall showing- A) Bilateral presence of pyramidalis muscle, B) Bilateral absence of pyramidalis muscle, C) Unilateral left side pyramidalis muscle, D) Unilateral right side pyramidalis muscle. P- pyramidalis muscle, RA – rectus abdominis muscle, RS- rectus sheath, U- umbilicus.
Discussion
Vestigial muscles in human beings are those muscles which are tendinous in larger part or reduced in size compared to the homologous muscles in other species or is frequently absent within or between populations. Pyramidalis muscle is also such muscle which is known to exhibit variations.
Phylogenetically, pyramidalis is linked to the pouch inside monotremes such as hedgehog and the platypus and marsupials such as the koala or kangaroo. In humans, standard anatomical textbooks describe the incidence of the pyramidalis muscle to be 83–90% [1]. Different authors around the globe had reported an incidence of pyramidalis in the range 82- 100% in various ethnic groups [Table/Fig-6] [3,6–9]. In our study in Indian population, an incidence of 92% (males-94.11%, females-87.5%) was reported. In Japanese [6] population, the incidence of pyramidalis was greater (94.5%) as compared to our study population. Incidence in the present study was greater than that reported in American blacks (82%) [3]. Kaur et al., and Jit et al., reported incidence of 87% and 100% in north Indian population [3,7]. Present study incidence fall between these data as our population included various subjects of different regions of India. The frequency of pyramidalis muscle in humans is probably influenced by racial and ethnic characteristics. Highest incidence of unilateral pyramidalis was reported in both the genders (male-17.64%, females-25%) of our study population as compared to the rest of populations of the world. Bilateral presence of pyramidalis muscle (72%) was the most common variety. Males showed a greater incidence of bilaterality (76.47%) than females (62.5%). Unilateral pyramidalis on right side (12%) was more common than unilateral left side (8%). Unilateral left pyramidalis was more common in females (12.5%) than males (5.88%). These differences were not statistically significant.
Comparison of morphometric data of pyramidalis muscle with other studies [3,6–9].
| S. No. | Authors | Year | Population | Total incidence (%) | Presence (%) | Bilateral absent (%) | Length (mm) | Width (mm) | Thickness (mm) |
|---|
| Unilateral | Bilateral | R | L | R | L | R | L |
|---|
| 1 | Mori [6] | 1964 | Japanese | 94.5 | - | - | - | - | - | - | - | - | - |
| 2 | Jit et al., [7] | 1986 | North Indian | 87 | Male- 6.45Female –7.31 | Male- 83.06Female–73.17 | Male- 10.48Female–19.51 | - | - | - | - | - | - |
| 3 | Didia et al., [9] | 2009 | Nigerian | 91.67 | - | - | - | 80.9 | 79.4 | 15.5 | 16 | - | - |
| 4 | Natsis et al., [8] | 2015 | Greek | 93.8 | 14.6 | 79.2 | 6.2 | Male | 83.7 | 75 | 16.1 | 15.6 | - | - |
| Female | 61.8 | 65.6 | 15 | 15.5 | - | - |
| 5 | Kaur et al., [3] | 2016 | NorthIndian | 100 | 6.67 | 93.33 | - | Male | 49.78 | 49.78 | 17.5 | 17.2 | - | - |
| Female | 48.73 | 47.84 | 12.5 | 14.57 | - | - |
| 6 | Present study | 2017 | Indian | 92 | Male- 17.64Female –25Total- 20 | Male- 76.47Female–62.5Total- 72 | Male- 5.88Female–12.5Total- 8 | Male | 52.21 | 53.97 | 18.35 | 17.05 | 4.91 | 4.33 |
| Female | 50.13 | 51.22 | 17.8 | 16.21 | 4.53 | 4.38 |
The morphometry of pyramidalis also varies with its frequency. Side asymmetry in length, width and thickness was noticed which was statistically insignificant [Table/Fig-3,4,5]. The biometric parameters of right side pyramidalis muscle were greater than the left side except the muscle length which was greater on left. The average muscle lengths in both the genders were lesser than the corresponding Greek ethnicity [8] and almost equal to the north Indian population [3,7]. The difference may be due to racial variations i.e., difference of stature in different populations. In contrast the average muscle width was greater than the Greek population [8] and roughly equal to the north Indians [3,7]. No statistically significant gender dimorphism was found on the basis of muscle length, width and thickness [Table/Fig-2,3 and 4]. No anatomical variations related to origin or insertion of muscle was seen.
Since, pyramidalis muscle serves as a landmark for surgeon for making a midline infraumbilical incision [10], pyramidalis- puboumbilical index [3] was calculated which could be clinically significant. The average pyramidalis- puboumbilical index was 35.15±4.38% in males and 36.01±4.97% in females [Table/Fig-2]. These values may be useful for surgeons as pyramidalis muscle covers the lower 35-36% of distance between umbilicus and pubic symphysis.
Though literature on the functions of pyramidalis has been vague yet it is unquestionably said to tense the linea alba. Some authors consider it to be immaterial and vestigial, but it is frequently encountered by gynaecologists during caesarean sections [11]. Lovering and Anderson studied the architecture and the fibre type of pyramidalis muscle and predicted that, this muscle generates less than 1% of the anticipated force generated by the rectus abdominis in normal sized adult [12]. This led them to the conclusion that the importance of this less amount of force on linea alba is not understandable. But, yet on a different note, it is frequently harvested to conduct electrophysiological experiments on muscles [13]. Apart from this, clinically the pyramidalis muscle has been used as a source of skeletal muscle stem cells for the treatment of post-prostatectomy stress urinary incontinence [5] and also been used for microsurgical transfer to treat small recalcitrant wounds in the foot/ankle region because of reduced donor site morbidity as compared to traditional free flaps [14]. Therefore, the biometric measurements of pyramidalis could help surgeons in proper sizing of pyramidalis muscle flaps. Pyramidalis muscle has been used successfully to treat severe dysuria due to insufficiency of the perineal floor muscles caused by upper and lower motor neuron lesions, by fixing the prostate with the pyramidalis muscle, associated with a bladder-pexy [15]. Considering the above facts, the role of the pyramidalis muscle cannot be overlooked.
Limitation
The limitation of current study was that the sample size was less (25 cadavers). Also fetal specimens were not included in this study, which could have given appropriate idea about the development of this muscle.
Conclusion
This cadaveric study shows that, the pyramidalis muscle is nearly a constant feature in Indian population. The morphometry of pyramidalis also varies along with its incidence. The muscle morphometric unevenness and its proven applications will help surgeons during lower abdominal wall surgeries.
[1]. Borley RN, Abdomen and PelvisIn: Standring S. Gray’s Anatomy: The anatomical basis of clinical practice 2008 40th edChurchhill Livingstone Elsevier publishers:1063 [Google Scholar]
[2]. Moore KL, Dalley AF, Clinically oriented Anatomy 2004 5th editionBaltimoreLippincott William and Wilkins:204 [Google Scholar]
[3]. Kaur H, Singla RK, Brar RS, Singla M, Study of the morphometry of the pyramidalis muscle and its incidence in the Indian populationInt J Anat Res 2016 4(2):2207-11. [Google Scholar]
[4]. Skandalakis JE, Skandalakin PN, Skandalakis JL, Surgical anatomy and techniqueA pocket manual 1995 New YorkSpringer-Verlag:930-38. [Google Scholar]
[5]. Sumino Y, Hirata Y, Hanada M, Akita Y, Sato F, Mimata H, Long term cryopreservation of pyramidalis muscle specimens as a source of striated muscle stem cells for treatment of post-prostatectomy stress urinary incontinenceProstate 2011 71(11):1225-30. [Google Scholar]
[6]. Mori M, Statistics on the musculature of the JapaneseOkajimas’ Fol Anat Jap 1964 40:195-300. [Google Scholar]
[7]. Jit I, Banga N, Incidence of pyramidalis muscle in north indian subjectsJournal of the Anatomical Society of India 1986 35(1):21-27. [Google Scholar]
[8]. Natsis K, Piagkou M, Repousi E, Apostolidis S, Kotsiomitis E, Apostolou K, Morphometric variability of pyramidalis muscle and its clinical significanceSurg Radiol Anat 2016 38(3):285-92. [Google Scholar]
[9]. Didia B, Loveday O, Christian I, Variations and incidence of agenesis of the pyramidalis muscle in Nigerian malesJ Exp and Clin Anat 2009 :8 [Google Scholar]
[10]. Skandalakis L, Skandalakis J, Surgical Anatomy and Technique: A Pocket Manual 2014 4th edNew YorkSpringer-Verlag:113 [Google Scholar]
[11]. Dickson MJ, The pyramidalis muscleJ Obstet Gynaecol 1999 19:300 [Google Scholar]
[12]. Lovering RM, Anderson LD, Architecture and fibre type of the pyramidalis muscleAnat Sci Int 2008 83(4):294-97. [Google Scholar]
[13]. Coffield JA, Bakry N, Zhang RD, Carlson J, Gomella LG, Simpson LL, In vitro characterization of botulinum toxin types A, C and D action on human tissues: Combined electrophysiologic, pharmacologic and molecular biologic approachesJ Pharmacol Exp Ther 1997 280:1489-98. [Google Scholar]
[14]. Landuyt KV, Hamdi M, Blondeel Ph, The pyramidalis muscle free flapBr J of Plast Surg 2003 56(6):582-92. [Google Scholar]
[15]. Gool V, Jong D, Urinary continence and erectile function after bladder neck sling suspension in male patients with spinal dysraphismBJU international 1999 83(9):971-75. [Google Scholar]