ED is defined as inability to achieve and/or maintain an erection for satisfactory sexual intercourse [1]. Its prevalence increases with age and can affect up to 52 percent men between age group of 40-69 years [2]. Erectile dysfunction is broadly classified into two categories; psychologic and organic. The most common cause of organic impotence is vasculogenic impotence and it may be a marker for occult cardiovascular disease [3]. Vasculogenic erectile dysfunction does not rule out the presence of contributing psychological factors, but merely means that vascular factors are the predominant cause. Two different mechanisms result in vascular erectile dysfunction; obstruction in penile inflow tract and the inability to trap the incoming blood in the cavernosa, both respectively termed as arterial and veno-occlusive erectile dysfunction.
The sonographic evaluation of erectile dysfunction was pioneered by Lue et al., [4]. They postulated that 75% increase in the diameter of cavernosal artery following intracavernosal injection of vasodilating agents is a good indication of normal arterial flow. This minimally invasive technique detects abnormalities in cavernous bodies such as fibrosis and calcifications (Peyronie’s disease), measures cavernous arterial diameter and flow, and also evaluates venous outflow.
PPDU can be performed by oral or intracavernosal vasoactive agents. Various intracavernosal vasoactive agents used for PPDU are papaverine alone or combination of papaverine, phentolamine and prostaglandin PGE1 (Trimix) [1]. Papaverine, when injected in penile tissue causes direct smooth muscle relaxation and consequent filling of the corpus cavernosum with blood resulting in erection. It may lead to persistent painful erection (priapism) in some patients. In comparison, Prostaglandin PGE1 has better erection rate and less incidence of priapism [5].
Oral Sildenafil citrate (Viagra) has been studied for non invasive evaluation of erectile dysfunction as an alternative to intracavernosal injection of vasoactive drugs. Unlike intracavernosal agents, Sildenafil alone cannot achieve satisfactory erection and it must be supplemented with audiovisual sexual stimulation and the results are inconsistent. The quality of erection and the PSV achieved with Sildenafil is lower than the same parameters achieved after intracavernosal injection [6].
To define the role of intracavernosal injection of Papaverine in the evaluation of vasculogenic causes of erectile dysfunction that includes arterial insufficiency and veno-occlusive nature.
Materials and Methods
A prospective longitudinal study was conducted in a tertiary care hospital in Department of Radiology, Hyderabad, India over a period of three years from 16 August 2013 to 15 August 2016 in a selected population of 73 patients.
Inclusion criteria: The study population included male patients of all ages who were being evaluated for erectile dysfunction and were referred from Department of Urology.
Exclusion criteria: Patients who were known cases of trauma, Peyronie’s disease or post operative status for some other penile pathologies, were excluded from this study.
Technique: The individual information, clinical history and findings of every patient were recorded in a prescribed format. A patient population of all ages was selected. Informed consent was taken from all patients. All procedures done were in accordance with the standards of the Institutional Ethics Committee.
The examination was conducted in an atmosphere of privacy. All cases were done using a linear broadband phased array transducer (7–12 MHz) on an E-Saote MyLab 60 ultrasound colour Doppler system.
First gray scale imaging of flaccid penile shaft in transverse and sagittal planes was done to measure the diameter of cavernosal artery and to rule out fibrosis or calcifications. Later Pharmaco penile duplex ultrasonography was done following intracavernosal injection of 60 mg of Papaverine using 30 G needle in either of the corpora cavernosa. The erectile response is graded visually from E0 to E5 as suggested by Broderick et al., [7]. Post Papaverine injection spectral wave forms were recorded once in 5 minutes upto 30 minutes. CAD, PSV, EDV, AT, RI and dorsal vein changes were recorded in all patients. The average time spent by study group in the Ultrasonography room was 40-45 min.
Statistical Analysis
The results were presented in number for the data in tables. All the data was analysed using SPSS software version 22.0 (SPSS Inc., Armonk, NY, USA). Statistical significance was accepted when p<0.05.
Results
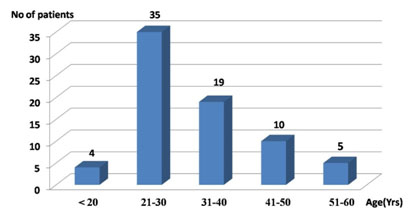
In this study, we selected 73 patients between the age group of 18-60 years with mean age of 32.5 years. Patients between age group of 21-30 years constitute the dominant group (48%) [Table/Fig-1].
Age wise distribution of number of patients.
Diabetes mellitus was present in fourteen patients, hypertension in eight patients, coronary artery disease in two patients and peripheral vascular disease in three patients.
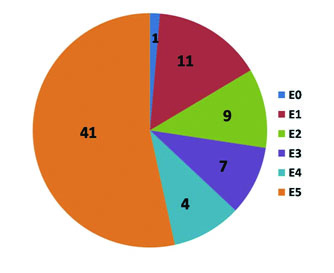
Visual grading for erectile response was E0 in 1 patient, E1 in 11 patients, E2 in 9 patients, E3 in 7 patients, E4 in 4 patients and E5 in 41 patients [Table/Fig-2].
Number of patients with different visual grading scores for erectile response.
In our study, cavernosal artery diameter in pre injection status was 0.3-1.2 mm with mean of 0.5 mm and post injection, it varied from 0.7-3 mm with mean of 1.5 mm.
All patients with visual grading response for erection E5 showed PSV ranging from 31.7-77.1 cm/sec with mean of 53.29 cm/sec.
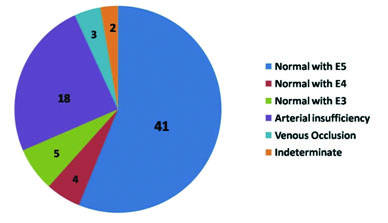
A total of 45 (61.6%) patients with grading score for erection E4 & E5 showed no evidence of arterial or venous insufficiency. A total of 18 (24.65%) patients showed evidence of arterial insufficiency, three (4.1%) patients showed evidence of venous insufficiency and two (2.7%) patients showed indeterminate results. However, small group of patients (5 in number) showed grading score for erection E3 without obvious evidence of arterial or venous insufficiency [Table/Fig-3].
Final PPDU impression with number of patients in each category. (Images left to right)
Discussion
Erectile mechanism is a complex, multiphasic event and erectile dysfunction occurs as a result of psychogenic, vascular, neurologic, endocrinologic or pharmacologic problems [8].
The penis contains three longitudinal erectile bodies, single corpora spongiosum seen on ventral aspect and two corpora cavernosa seen on dorsal aspect and the urethra is seen within the corpora spongiosum. The main arterial supply comes from internal pudendal artery and its branches. The cavernosal artery extends throughout the length of corpus cavernosum and plays an important role in the blood flow of erectile tissue. Numerous side branches arise from cavernosal artery called helicine arteries supply the cavernosal spaces. Venous drainage is mainly through emissary veins which drains the corpus cavernosum and empties into the deep dorsal venous system of the penis [8].
Initial scan in transverse plane before injection during the flaccid state shows diameter of cavernosal artery which ranges from 0.2-1 mm [1]. The arterial flow is difficult to demonstrate in flaccid state, but sometimes can show damped and monophasic systolic wave form with minimal diastolic component.
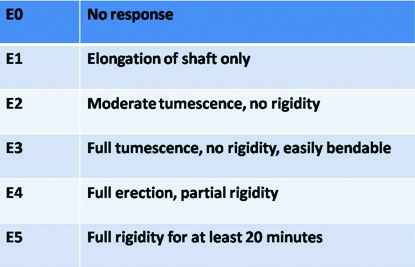
Post intracavernosal injection, both erectile response and vascular flow are analysed. The erectile response is graded visually from E0 to E5 as suggested by Broderick et al., [Table/Fig-4] [7].
Brderick et al.,’ visual grading score for penile erection during PPDU.
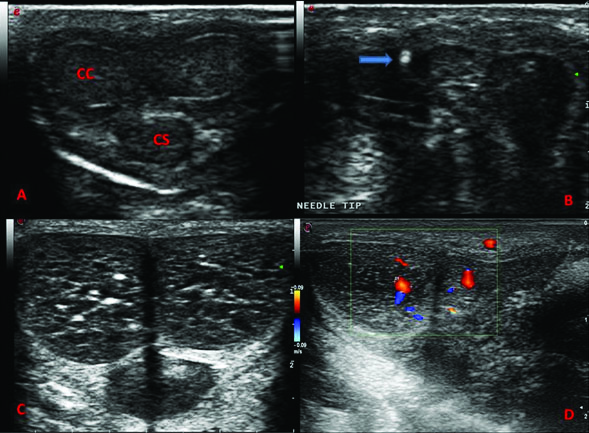
After evaluating the erectile response, scanning is done from the base at the penoscrotal junction to distal part both in transverse and sagittal planes to assess increase in cavernosal artery diameter [Table/Fig-5].
a) normal penile anatomy in transverse plane; b) needle tip in situ; c) post injection, enlarged cavernosal spaces; d) increased cavernosal diameter. (CC-Corpora cavernosum & CS-Corpora spongiosum)
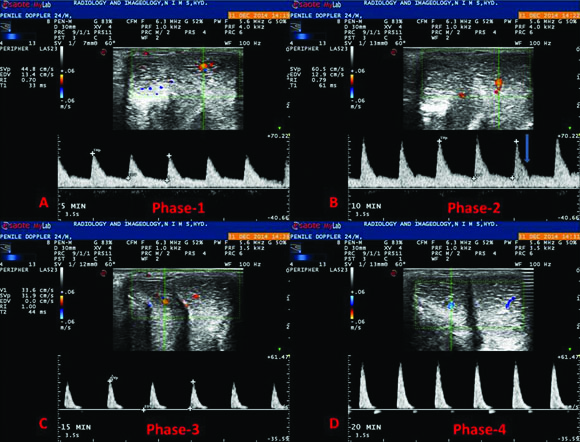
A 75% or more increase in vessel diameter is good indication of normal arterial flow into the cavernosal artery. Post papaverine injection, normal spectral waveform has been described to have five phases [9]. Phase 1 shows increase in both systolic and diastolic velocities. In phase 2, there is progressive decrease in end diastolic velocity and appearance of a dicrotic notch. In phase 3, diastolic flow approximates zero and it is reversed in phase 4. Phase 5 shows eventual loss of both systolic and diastolic signals [Table/Fig-6].
Normal spectral waveform pattern following intracavernosal papaverine injection. (Images left to right)
Normal flowmetry reference values during PPDU are: PSV-25 cm/sec or more, EDV-5 cm/sec or less, AT-0.11 sec or less and RI-0.85 or more [1]. Less than 75% increase in baseline cavernosal artery diameter, abnormal PSV (less than 25 cm/ sec) and AT (more than 0.11 sec) are suggestive of arterial disease. Veno occlusive disease is suggested by abnormal EDV (more than 5 cm/ sec) and RI (less than 0.85) [10].
In this study, whenever PSV was low, age was significantly high and t-test was statistically significant (t=4.279).
All patients with E0, E1 & four patients with E2 showed less than 75% increase in cavernosal artery diameter in post injection scans. In rest of patients, more than 75% increase in cavernosal artery diameter was noted. A study by Acharya and Vasu showed the post injection, mean diameter was 1.0 mm, where as in our study, it was 1.5 mm [11].
If PSV was < 25cm/sec (Arterial insufficiency), visual grading score for erection was E0 in 5.6% patients, E1 in 61.1% patients and E2 in 33.3% patients. If PSV was > 25cm/sec, visual grading score for erection was E3 in 10% patients, E4 in 8% patients and E5 in 82% patients. Pearson Chi-Square was 41.542 and p-value was < 0.001 that means this finding was statistically highly significant in distribution of patients based on erection score between PSV <25 cm/sec & PSV > 25 cm/sec. Similarly, erection score E2 was seen in 100% patients with EDV > 5 cm/sec (Veno occlusive disease) as compared to 8.5% in patients with EDV<5 cm/sec. Pearson Chi-Square was 16.708 and p-value was < 0.001 that means this finding was statistically highly significant.
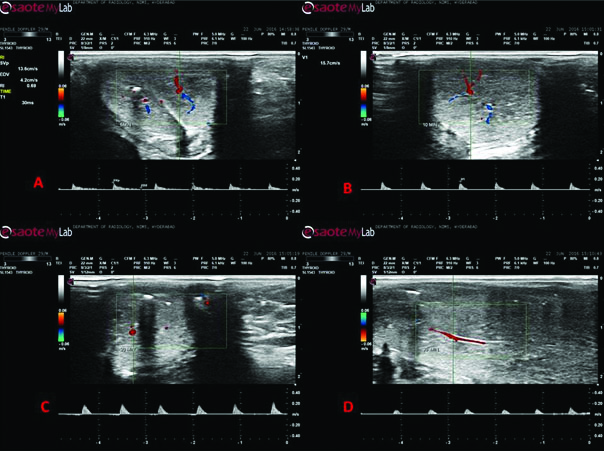
Eighteen patients did not achieve PSV of atleast 25 cm/sec upto 30 min and were diagnosed as having arterial insufficiency [Table/Fig-7]. If PSV during the procedure was > 25 cm/sec, 77.3% of cases were presented as normal. If PSV was < 25 cm/sec, 100% of cases were presented as arterial insufficiency. Pearson Chi-Square was 22.005 and p-value was < 0.001 that means this finding was statistically highly significant.
Arterial insufficiency-PSV is less than 25 cm/sec upto 30 min.
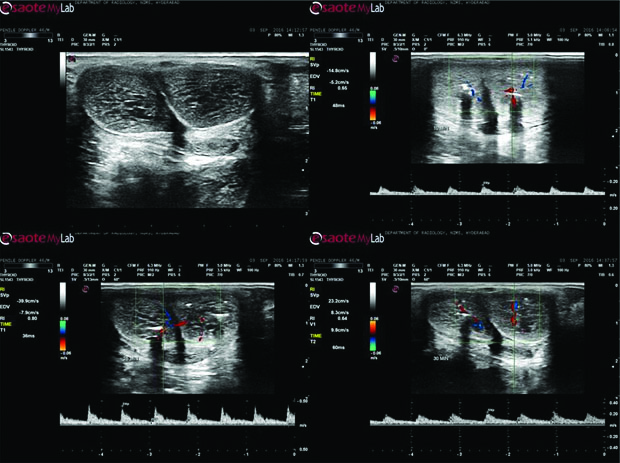
Three patients showed persistence of EDV of > 5 cm/sec or RI of < 0.85 suggestive of veno occlusive disease [Table/Fig-8]. It was observed that if EDV is > 5cm/sec, 100% patients showed veno-occlusive disease. Pearson Chi-Square was 47.981 and p-value was < 0.001 that means this finding was statistically highly significant. In Veno occlusive patients with RI <0.85, higher number of patients had associated risk factors like diabetes and hypertension. p-value was 0.027, that means statistically significant correlation between risk factors and venous insufficiency.
Veno occlusive disease –EDV is more than 5cm/sec upto 30 min.
Normal deep dorsal vein velocity is less than 3 cm/sec. Moderately increased is 10-20 cm/sec and markedly increased when higher than 20 cm/sec and is a sign of veno occlusive disease [12]. Increase in dorsal vein velocity (13 cm/sec) was found in one case of venous insufficiency.
Two patients showed mixed arterial and venous insufficiency or indeterminate result. However, the diagnosis of mixed arterial and venous ED cannot be made using duplex Doppler sonography because venous competence cannot be assessed in a patient with arterial insufficiency [10].
In our study, two patients had developed priapism, which were of low flow in nature and treated by emergency decompression by urologist. These findings are similar to a study by Kilic et al., [13].
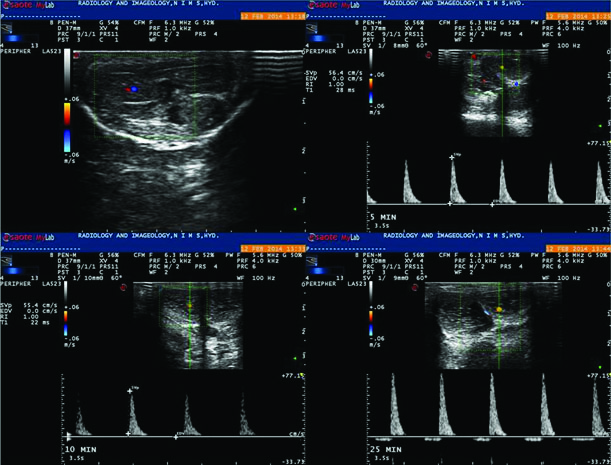
Two patients immediately after intracavernosal injection showed spectral waveform of phase 3 nature without evidence of phase-1 & 2 type waveforms [Table/Fig-9]. Even after thorough research, we could not find any explanation in literature, which needs further workup.
Immediately after injection, the spectral waveform entered Phase 3 pattern without evidence of phase 1 & 2 patterns. (Images left to right)
In our study, PPDU had significantly contributed in the evaluation of vasculogenic causes of erectile dysfunction. This technique has the advantages of being fast, easily available, cost effective and the results are highly accurate [8]. The disadvantages are post procedural pain, chances of haematoma and rarely priapism [10].
Limitation
The limitation in our study is lack of comparison with other intracavernosal and oral drugs.
Conclusion
Vasculogenic pathologies dominate the organic causes of erectile dysfunction. This finding supports increased utilization of penile Doppler for vascular evaluation. Even though arteriography is considered as the gold standard for assessing arteries of the penis, minimally invasive PPDU has emerged as the primary investigation of choice in differentiating psychogenic and vasculogenic causes of erectile dysfunction and aids in assessing erectile dysfunction due to arterial insufficiency and veno occlusive disease accurately.
Conflict of interest: None identified.