Mesenteric Teratoma in Elderly Female: A Rare Case Report
Chandrasekhar Sharanappa Neeralagi1, KR Surag2, Yogesh Kumar3, S Lakkanna4, Preetham Raj5
1 Junior Resident, Department of General Surgery, ESIC Medical College, Bengaluru, Karnataka, India.
2 Junior Resident, Department of General Surgery, ESIC Medical College, Bengaluru, Karnataka, India.
3 Junior Resident, Department of General Surgery, ESIC Medical College, Bengaluru, Karnataka, India.
4 Professor, Department of General Surgery, ESIC Medical College, Bengaluru, Karnataka, India.
5 Assistant Professor, Department of General Surgery, ESIC Medical College, Bengaluru, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Chandrasekhar Sharanappa Neeralagi, # 3, Syndicate Residency, 1st Main, Vidyagiri, Dharwad-580004, Karnataka, India.
E-mail: chandrusn22@gmail.com
Dermoid cysts rarely present as mesenteric cysts. Mesenteric cysts are rare pathologic entities, with a reported incidence of approximately 1 of 27 000 to 1 of 100 000 admissions. Mesenteric cyst was first described by Florentine anatomist Benevieni in 1507, while performing an autopsy on an eight-year-old boy. Most commonly, teratoma occurs in the early age group. Mature mesenteric teratoma in adulthood is extremely rare. Teratoma are germ cell tumours commonly composed of multiple cell types derived from one or more of the 3 germ layers. We present the case of a 69-year-old elderly female who presented with abdomen pain for nine months with right lumbar and right iliac fossa mass. Computed Tomography (CT) abdomen revealed bilocular cystic lesion with possibility of mucinous cystadenoma with no definitive organ of origin. She underwent explorative laparotomy and total excision of the cystic mass. Histopathologic examination confirmed diagnosis of mature cystic teratoma of mesentery. This case report highlights the need to maintain high index of suspicion while evaluating abdominal mass.
Autopsy, Cystic, Dermoid, Germ Cell, Laparotomy
Case Report
A 69-year-old female patient presented with abdomen pain for nine months. She had a history of hysterectomy with bilateral salphingo-opherectomy, 25 years back. Physical examination revealed mass in right iliac fossa extending into right lumbar region measuring 20x18 cm. Swelling was firm in consistency, smooth surface with all borders well defined.
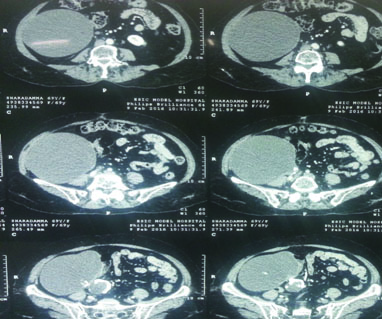
The patient was subjected to ultrasonogram (USG) abdomen which showed 12x13x11 cm thick walled cystic lesion with calcified foci occupying right iliac fossa extending to lumbar region. CT scan of abdomen was suggestive of bilocular cystic lesion with possibility of mucinous cystadenoma with mucocele [Table/Fig-1]. CA-125 ovarian tumour marker level was assayed and found to be within normal limit.
CT scan of abdomen features suggestive of bilocular cystic lesion with possibility of mucinous cystadenoma with mucocele.
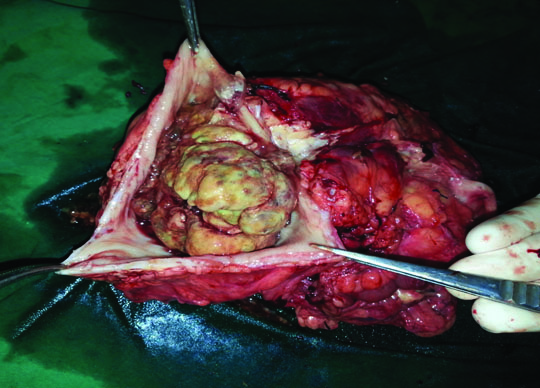
She underwent laparotomy with midline incision. On abdominal cavity exploration a large mass was noted involving right iliac fossa, lumbar and hypochondrium with wrapped up omentum around the mass. Bowel and solid organs liver spleen kidneys were found to be healthy. Uterus and both the ovaries were absent. The cyst was excised in toto, on opening the cyst thick gelatinous mucinous material, unilocular cyst with calcified areas gritty to cut, may be teeth were noted [Table/Fig-2].
Specimen of cyst thick gelatinous mucinous material, unilocular cyst with calcified areas gritty to cut, may be teeth.
The specimen was subjected to histopathological examination and report showed cyst wall lined by flattened cuboidal epithelium, cyst contains derivative of ectoderm lined by squamous epithelium keratin material, mesoderm bone marrow elements fibro fatty tissue, cartilage and endoderm derivative like intestinal glands confirming the diagnosis of mature cystic teratoma arising from mesentery.
Discussion
Mesenteric cysts are rare pathologic entities, with a reported incidence of approximately 1 of 27 000 to 1 of 100 000 admissions. Florentine anatomist Benevieni first described a mesenteric cyst in 1507, while performing an autopsy on an eight-year-old boy [1]. Teratomas are germ cell tumours composed of multiple cell types derived from one or more of the three germ layers. The word teratoma is derived from the Greek teras, meaning monster [2]. Most commonly teratoma occurs in the early age group [3]. Mature mesenteric teratoma in adulthood is extremely rare [4].
Dermoid cysts rarely present as mesenteric cysts. Teratoma can occur anywhere in pathway of ectodermal cell migration, especially in the midline, from the cranium, mediastinum and retroperitoneum to sacrococcygeal regions [5]. The most common location is sacrococcygeal (57%) and in the gonads, more so in ovary. Cystic teratomas occasionally occur in sequ estered midline embryonic cell rests and can be mediastinal (7%), retroperitoneal (4%), cervical (3%), and intracranial (3%) [6].
Differential diagnosis for mesenteric cystic mass include mesenteric or omental cyst, cystic teratoma, cystic spindle cell tumours and cystic mesothelioma. The most common type of mesenteric or omental cyst is lymphangioma [7]. Mesenteric cystic lymphangioma with calcification simulates cystic teratoma radiologically [8].
Malignant forms of mesenteric cysts have been described previously [9] and the incidence of malignancy is reported to be less than 3% [10]. To exclude malignant potential, performing complete surgical excision and a full histological examination of the resected specimen are recommended [9]. Mesenteric cysts can be treated with either laparotomy or laparoscopic surgery. The selection of the surgical approach depends on the size of the cyst, the location within the abdominal cavity, and the skill of the surgeon.
Conclusion
In this article we have described a rare presentation of mesenteric dermoid in right iliac fossa and lumbar region in old age patient with diagnostic challenge and hence it becomes imperative for the practicing physician to consider it as differential diagnosis of any cystic lesion of abdomen, even though imaging might not be contributory.
[1]. Kurtz Robert J, Heimann Tomas M, Robert BA, James H, Mesenteric and retroperitoneal cystsAnn Surg 1986 203:109-12. [Google Scholar]
[2]. Pantoja E, Noy MA, Axtmayer RW, Colon FE, Pelegrina I, Ovarian dermoids and their complications. Comprehensive historical reviewObstet Gynecol Surv 1975 30(1):1-20. [Google Scholar]
[3]. De J, Banerjee M, Biswas PK, Banerjee AK, Karim R, Mature teratoma of the mesenteryJ Indian Med Assoc 2002 100(3):198-99. [Google Scholar]
[4]. Cuevas-Ocampo AK, Tavares-García S, Martínez-Gómez H, Mature mesenteric teratoma in an adult male. A case reportRev Med Inst Mex Seguro Soc 2011 49(2):209-12. [Google Scholar]
[5]. Yu CW, Liu KL, Lin WC, Li YW, Mature cystic teratoma of pancreas in a childPediatric Radiology 2003 33(4):266-68. [Google Scholar]
[6]. Grosfeld JL, Billmire DF, Teratomas in infancy and childhoodCurr Probl Cancer 1985 9(9):1-53. [Google Scholar]
[7]. Grainger RG, Allison DJ, Imaging of mesentery and omentum. In: Ana I. Nicolas, Pablo R. Ros, editorsDiagnostic radiology 1997 LondonChurchill Livingstone:1076-78. [Google Scholar]
[8]. Stoupis C, Ros PR, Abbitt PL, Burton SS, Gauger J, Bubbles in the belly: Imaging of cystic mesenteric or omental massesRadiographics 1994 14(4):729-37. [Google Scholar]
[9]. Bury TF, Pricolo VE, Malignant transformation of benign mesenteric cystAm J Gastroenterol 1994 89(11):2085-87. [Google Scholar]
[10]. Liew SC, Glenn DC, Storey DW, Mesenteric cystAust N Z J Surg 1994 64(11):741-44. [Google Scholar]