Materials and Methods
Bacterial Isolates and Controls
This prospective study was carried out for a period of six months from February to July 2015 in Department of Clinical Pathology, Haffkine Institute. During this study period, a total of 341 clinical isolates of genera Staphylococcus was collected from Sir Jamshedjee Jeejeebhoy (JJ) Hospital, a tertiary care hospital. The inclusion criteria for collection of the isolates were based on Gram staining results i.e., Gram positive cocci in clusters. All other isolates i.e. Gram negative bacteria and Gram positive cocci in clusters with mixed flora were excluded from the study. The sources of these isolates included pus, urine, blood culture and sterile body fluids. The isolates were identified as Staphylococcus genera by Furazolidone (100 mcg) antibiotic disc wherein, the isolates exhibited zone diameter greater than 15 mm [15]. S. aureus ATCC 25923 and Staphylococcus epidermidis ATCC 12228 were used as positive and negative control respectively.
Identification of S. aureus by Conventional Methods
All the clinical isolates were tested by TCT using RP and HP, MSA and DNase agar media for identification and differentiation of S. aureus from CoNS. The HACCK was also used as a phenotypic test.
TCT
The TCT was performed using commercially available RP (HiMedia Laboratories, Mumbai, India) and 1:10 diluted HP (National Plasma Fractionation Centre, Mumbai, India). Pure colonies from an 18-hour-old culture were inoculated into 0.5 ml of respective plasmas, incubated at 37°C and observed for clot formation for four hours. In case of no clot observed at four hours, the test was continued with an overnight incubation at room temperature. A final observation at 24 hours was noted [16]. Prior to coagulase testing, the plasma was checked for its coagulase activity using ATCC cultures which include S. aureus ATCC 25923, S. aureus ATCC 29213 and S. aureus ATCC 43300 that were coagulase positive and S. epidermidis ATCC 12228, Staphylococcus saprophyticus ATCC 15305 and Staphylococcus haemolyticus ATCC 29970 that were coagulase negative. The plasma was kept in 1.5 ml sterile cryovials and stored at -80°C till further use.
HACCK
HACCK is a coagulase based test for rapid identification of S. aureus and differentiation from CoNS. The kit contents included tubes with dehydrated medium, suspension fluid and a dropper. The test was carried out using manufacturer’s instructions. Briefly, the content of the tube was rehydrated with the sterile suspension fluid. The culture was inoculated in the tube and incubated at 37°C. The tubes were observed for clot formation at regular intervals up to four hours. A positive result was indicated by clot formation. The tube was incubated overnight at room temperature in case of no clot formation until four hours and interpreted as either positive or negative based on clot formation [16,17].
Growth on MSA and DNase Agar Media
The isolates were streaked on MSA media. Growth of yellow colonies on MSA after 24 hours of incubation at 37°C was an indicative of positive result [9]. The DNase test was performed by spotting and incubating the isolates for 24 hours at 37°C on DNase agar with Toluidine blue. Appearance of the pink zone of clearance around the growth of bacteria was an indicative of a positive result [16].
Identification of S. aureus by PCR
The detection of S. aureus by PCR amplification was used as a reference point test. A monoplex PCR targeting the femA gene was carried out for identification of S. aureus using the primers femA-F 5’-CGATCCATATTTACCATATCA-3’ and femA-R 5’- ATCACGCTCTTCGTTTAGTT-3’ [18]. An aliquot of 2 μl of the extracted DNA was used as a template in a 25 μl of PCR mixture containing 1X PCR buffer, 2.5 mM MgCl2 (HiMedia Laboratories, Mumbai, India), 0.2 mM dNTPs mix (HiMedia Laboratories, Mumbai, India), 1U of Taq DNA polymerase enzyme (HiMedia Laboratories, Mumbai, India) with 0.2 μM of each primer. The amplification was performed with the following thermal cycling profile; 1 cycle of initial denaturation at 94°C for 3 min, followed by 30 cycles of amplification (denaturation at 94°C for 30 s, annealing at 56°C for 45 s and extension at 72°C for 30 s) with a final extension at 72°C for 5 min on Prima 96™ PCR machine (HiMedia Laboratories, Mumbai, India). The PCR products were subjected to Agarose Gel Electrophoresis (1.5% Agarose, 1X Tris-Acetate-EDTA) and were resolved along with a 100-bp molecular size ladder. The amplicons were visualized and photographed using a Gel Doc system (Bio-Rad Laboratories, California, USA) [18].
Statistical Analysis
The PCR results were compared to the conventional methods for identification of S. aureus. The data were analysed by a 2×2 contingency table. The sensitivity and specificity were calculated using the diagnostic test evaluation calculator available from MedCalc website [19]. For categorical assessment of the agreement of the conventional tests and coagulase confirmation kit with the PCR assay, Cohen’s kappa coefficient (κ) was calculated using a free tool available from Graph Pad software website [20,21].
Results
Identification of S. aureus using PCR
The identification of S. aureus by targeting the femA gene was used as a reference point test for comparison. Among the 341 staphylococci isolates, 82.40% (n=281) were positive for femA gene while 17.60% (n=60) strains were negative.
Identification of S. aureus by conventional methods
TCT and HACCK
Of the 281 femA positive isolates, 98.58% (n=277) and 95.37% (n=268) exhibited clot formation in the TCT using RP and HP. A 100% (n=281) positivity was observed among femA positive isolates by HACCK. Likewise, the 60 femA negative isolates were negative by the TCT using RP and the HACCK. However, 96.67 (n=58) isolates were negative in TCT using HP as two femA negative isolates showed clot formation.
Growth on MSA and DNase agar media
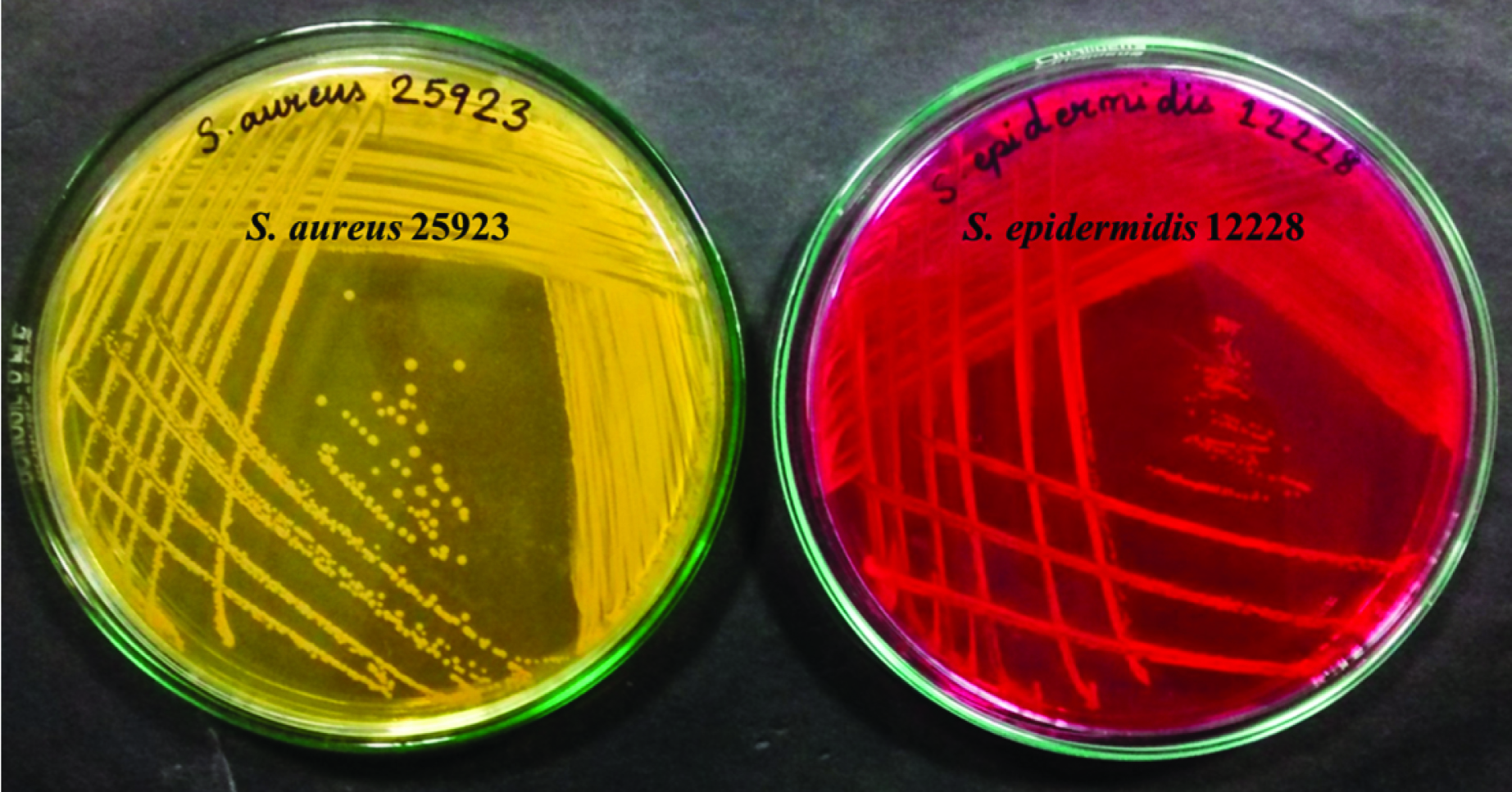
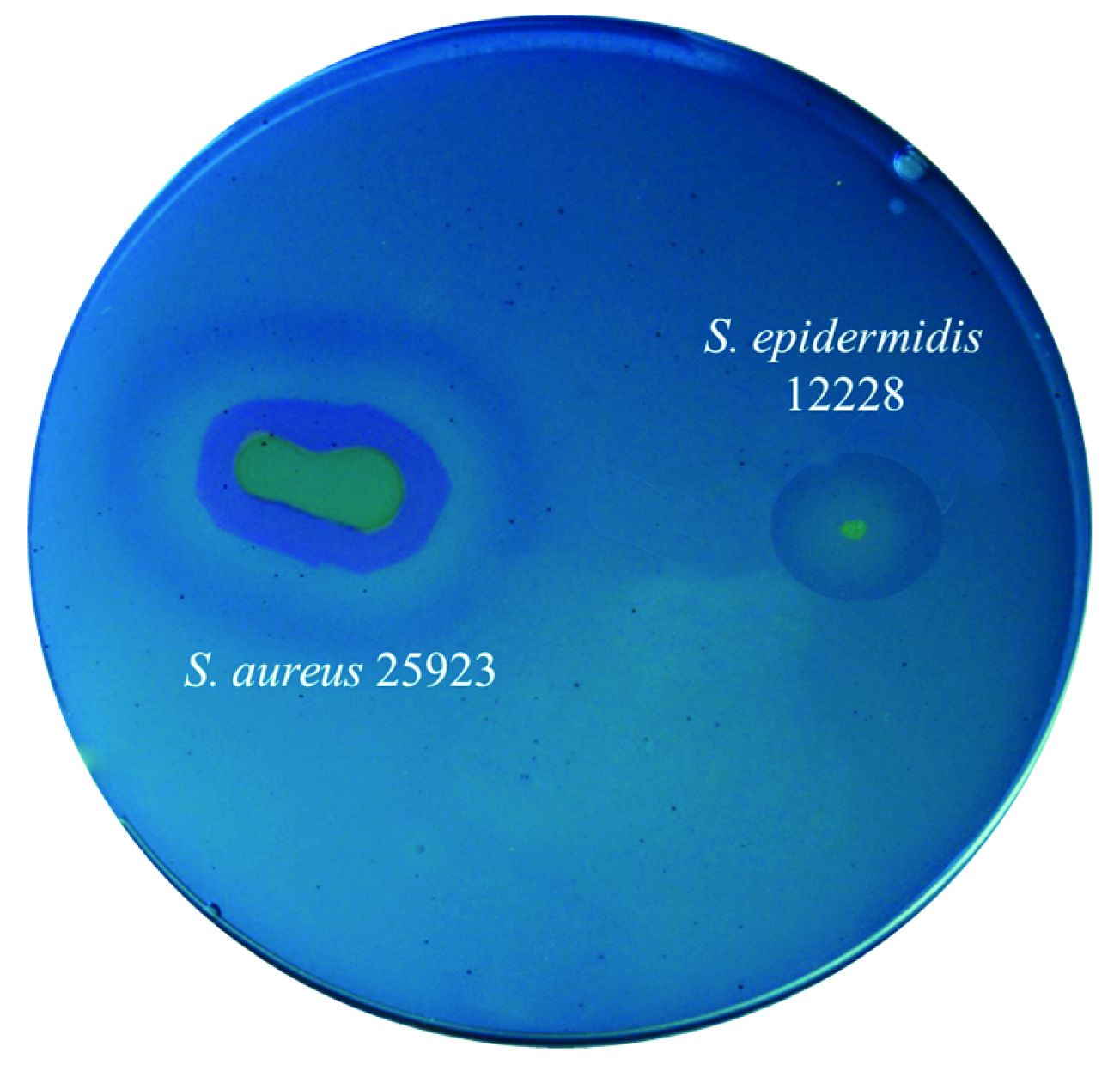
In the mannitol fermentation test using MSA media, 97.86% (n=275) femA positive isolates were positive, while the remaining 2.14% (n=6) femA positive isolates were negative. Of the femA negative isolates, 100% (n=60) of isolates produced pink coloured colonies on MSA and were therefore, marked as CoNS [Table/Fig-1]. In the DNase test, DNase activity was exhibited among 96.44% (n=271) femA positive isolates while 3.56% (n=10) of isolates were negative in this test. Besides, 8.33% (n=5) of femA negative isolates produced pink zones of clearance and the remaining 91.67% (n=55) of femA negative isolates were negative in this test [Table/Fig-2].
Representation of Mannitol Salt Agar (MSA).
Yellow colour colonies – mannitol fermentation positive
Pink colour colonies – mannitol non-fermentation negative
Representation of Deoxyribonuclease (DNase) agar.
Appearance of pink zone of clearance around the growth of bacteria – DNase activity positive
Appearance of no pink zone of clearance around the growth of bacteria – DNase activity negative
Efficiency of Combination of Tests
Among the total 341 isolates, a complete concordance of 90.91% (n=310) was observed amongst the conventional tests and HACCK in comparison to femA PCR assay of which 75.95% (n=259) isolates were identified as S. aureus and 15.54% (n=53) were marked as CoNS by all the tests. Discordant results were observed in 8.54% (n=29) isolates using the tests. Therefore, the combination of tests was evaluated.
RP with MSA and/or DNase media
About 96.80% (n=272), 95.73% (n=269) and 94.66% (n=266) of femA positive isolates were identified as S. aureus by combination tests of RP+MSA, RP+DNase and RP+MSA+DNase combination respectively in comparison to PCR [Table/Fig-3]. Likewise, 100% (n=60), 91.67% (n=55) and 91.67% (n=55) tested negative for S. aureus by either tests of RP+MSA, RP+DNase and RP+MSA+DNase combination respectively in comparison to PCR [Table/Fig-3].
Identification of S. aureus by conventional methods in comparison to femA PCR as reference point test (n=341).
| Phenotypic methods | femA positive isolates (n=281) | femA negative isolates (n=60) |
|---|
| % TP | % FN | % FP | % TN |
|---|
| RP | 98.58 | 1.42 | 0.00 | 100.00 |
| HP | 95.37 | 4.63 | 3.33 | 96.67 |
| HACCK | 100.00 | 0.00 | 0.00 | 100.00 |
| MSA | 97.86 | 2.14 | 0.00 | 100.00 |
| DNase | 96.44 | 3.56 | 8.33 | 91.67 |
| RP+MSA | 96.80 | 3.20 | 0.00 | 100.00 |
| RP+DNase | 95.73 | 4.27 | 8.33 | 91.67 |
| RP+MSA+DNase | 94.66 | 5.34 | 8.33 | 91.67 |
| HP+MSA | 93.95 | 6.05 | 3.33 | 96.67 |
| HP+DNase | 93.95 | 6.05 | 11.67 | 88.33 |
| HP+MSA+DNase | 92.53 | 7.47 | 11.67 | 88.33 |
| HACCK+MSA | 97.86 | 2.14 | 0.00 | 100.00 |
| HACCK+DNase | 96.44 | 3.56 | 8.33 | 91.67 |
| HACCK+MSA+DNase | 95.02 | 4.98 | 8.33 | 91.67 |
| MSA+DNase | 95.02 | 4.98 | 8.33 | 91.67 |
RP – Rabbit Plasma, HP – Human Plasma, HACCK - HiaureusTM Coagulase Confirmation Kit, MSA – Mannitol Salt Agar, DNase – Deoxyribonuclease media, TP – True Positive, FN – False Negative, FP – False Positive, TN – True Negative
HP with MSA and/or DNase media
In conflict to RP, 93.95% (n=264), 93.95% (n=264) and 92.53% (n=260) of isolates were labelled as S. aureus by HP+MSA, HP+DNase and HP+MSA+DNase combination respectively in comparison to PCR [Table/Fig-3]. In the same way, 96.67% (n=58), 88.33% (n=53) and 88.33% (n=53) were identified as CoNS by either tests of HP+MSA, HP+DNase and HP+MSA+DNase combination respectively in comparison to PCR [Table/Fig-3].
HiaureusTM Coagulase Confirmation Kit with MSA and/or DNase media
Of the total 281 femA positive isolates, 97.86% (n=275), 96.44%, (n=271) and 91.67% (n=267) of the isolates were identified as S. aureus using the combination of HACCK+MSA, HACCK+DNase and HACCK+MSA+DNase respectively [Table/Fig-3]. On the other hand, 100% (n=60), 91.67% (n=55) and 91.67% (n=55) of the isolates did not test positive for S. aureus using either tests of HACCK+MSA, HACCK+DNase and HACCK+MSA+DNase combination respectively in comparison to PCR [Table/Fig-3].
MSA and/or DNase Media
The combination of two medias identified 95.02% (n=275) of isolates as S. aureus. Correspondingly, 91.67% (n=55) of isolates were misidentified as S. aureus by MSA+DNase test in comparison to PCR assay [Table/Fig-3].
Assessment of Sensitivity and Specificity
The results were statistically analysed using a 2×2 contingency table to calculate the specificity and sensitivity for evaluation of individual tests and combination of tests for identification of S. aureus in comparison with PCR amplification of femA gene [Table/Fig-4]. Amongst the coagulase based tests, HACCK was 100% sensitive and specific in the detection and differentiation of S. aureus from CoNS. The TCT using RP was 98.58% sensitive while TCT using HP was comparatively less sensitive i.e., 95.37%. Conversely, 100% specificity was observed for TCT using RP while TCT using HP had a specificity rates of 96.67%. The MSA and DNase media had a sensitivity rate of 97.86% and 96.44% and specificity rate of 100% and 91.67% respectively. Among the combination tests, HACCK+MSA showed better sensitivity (97.86%) as compared to RP+MSA (96.80%). The other combination tests had a good sensitivity rate, but low specificity rate with an exception of HP+MSA with low sensitivity and moderate specificity rate (93.95% vs 96.67%).
Calculation of Sensitivity, Specificity, Positive Predictive Value (PPV) and Negative Predictive Value (NPV) of conventional tests in comparison to femA PCR.
| Methods for S. aureus detection | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) |
|---|
| RP | 98.58 | 100.00 | 100.00 | 93.75 |
| HP | 95.37 | 96.67 | 99.26 | 81.69 |
| HACCK | 100.00 | 100.00 | 100.00 | 100.00 |
| MSA | 97.86 | 100.00 | 100.00 | 90.91 |
| DNase | 96.44 | 91.67 | 98.19 | 84.62 |
| RP+MSA | 96.80 | 100.00 | 100.00 | 86.96 |
| RP+DNase | 95.73 | 91.67 | 98.18 | 82.09 |
| RP+MSA+DNase | 94.66 | 91.67 | 98.15 | 78.57 |
| HP+MSA | 93.95 | 96.67 | 99.25 | 77.33 |
| HP+DNase | 93.95 | 88.33 | 97.42 | 75.71 |
| HP+MSA+DNase | 92.53 | 88.33 | 97.38 | 71.62 |
| HACCK+MSA | 97.86 | 100.00 | 100.00 | 90.91 |
| HACCK+DNase | 96.44 | 91.67 | 98.19 | 84.62 |
| HACCK+MSA+DNase | 95.02 | 91.67 | 98.16 | 79.71 |
| MSA+DNase | 95.02 | 91.67 | 98.16 | 79.71 |
RP – Rabbit Plasma, HP – Human Plasma, HACCK - HiaureusTM Coagulase Confirmation Kit, MSA – Mannitol Salt Agar, DNase – Deoxyribonuclease Media, TP – True Positive, FN – False Negative, FP – False Positive, TN – True Negative
Sensitivity = TP/ (TP+FN)*100, Specificity = TN/ (FP+TN)*100, PPV = TP/ (TP+FP)*100, NPV = TN/ (TN+FN)*100
Calculation of Cohen’s kappa coefficient (κ) and concordance rates
The Cohen’s kappa (κ) value and concordance rates were calculated for every test in comparison to femA PCR. Among the tests, HACCK showed 100% concordance with the PCR assay (κ=1) and labelled as a perfect test. Four different tests i.e., RP, MSA, RP+MSA and HACCK+MSA were labelled almost perfect test to have concordance rate nearing 100% with varying κ values. The remaining tests were labelled either strong or moderate tests [Table/Fig-5].
Kappa coefficient test for agreement between two tests.
| Methods for S. aureus detection | κ at 95% CI | Concordance with PCR (%) | Strength of agreement |
|---|
| HACCK | 1 | 100 | Perfect |
| RP | 0.961 | 98.83 | Almost perfect |
| MSA | 0.942 | 98.24 | Almost perfect |
| RP+MSA | 0.914 | 97.36 | Almost perfect |
| HACCK+MSA | 0.942 | 98.24 | Almost perfect |
| HP | 0.859 | 95.6 | Strong |
| DNase | 0.853 | 95.6 | Strong |
| RP+DNase | 0.836 | 95.01 | Strong |
| HP+MSA | 0.825 | 94.43 | Strong |
| HACCK+DNase | 0.853 | 95.6 | Strong |
| MSA+DNase | 0.819 | 94.43 | Strong |
| RP+MSA+DNase | 0.81 | 94.13 | Strong |
| HACCK+MSA+DNase | 0.819 | 94.43 | Strong |
| HP+DNase | 0.63 | 87.81 | Moderate |
| HP+MSA+DNase | 0.741 | 91.79 | Moderate |
RP – Rabbit Plasma, HP – Human Plasma, MSA – Mannitol Salt Agar, DNase – Deoxyribonuclease Media
κ at 95% CI (None: 0.0 – 0.2, Minimal: 0.21 – 0.39, Weak: 0.40 – 0.59, Moderate: 0.60 – 0.79, Strong: 0.80 – 0.89, Almost Perfect: 0.90 – 0.99 and Perfect: 1)
Discussion
Accurate and rapid detection play a vital role in the proper management of infections caused by S. aureus. In the present study, we attempted to evaluate the conventional methods for detecting S. aureus and differentiating from other staphylococci in parallel to a commercially available kit. Of the total 341 isolates, 82.40% of the isolates were identified as S. aureus based on the presence of femA gene, a chromosomally encoded factor, occurring naturally in S. aureus [22]. This gene has been implicated in cell wall metabolism and is present in large amounts in actively growing cultures [18,23].
Coagulase test, the most common conventional test, is either performed as a slide coagulase test or by TCT. The slide coagulase test is based on the characteristic presence of bound coagulase i.e. clumping factor in S. aureus. However, a high rate of false negatives (about 10-15%) has been reported by this test [12,24]. This may be due to masking of the clumping factor by the capsular polysaccharides or due to misidentification of certain clumping factor producing CoNS; thereby, reducing its efficiency, reliability and sensitivity [12,25,26].
The plasma has a component called the Coagulase Reacting Factor (CRF) which binds to the Staphylococcal Coagulase (SC) and forms SC-CRF complex resulting in the conversion of fibrinogen to fibrin clot which forms the basis of coagulase test. RP, pig plasma and HP have been deemed to be the most suitable plasmas for coagulase testing with optimal concentration of CRF, high sensitivity, specificity and low reaction time [27–29]. However, pig plasmas are not widely available and therefore, RP and HP are ideal candidates for testing purposes [30].
In the present study, TCT was performed using RP and HP. The TCT using RP had a sensitivity and specificity rate of 98.58% and 100% respectively which were in agreement with other studies [31,32]. High sensitivity, less reaction time, easy acquisition of rabbits, non-laborious breeding and bleeding makes them as an appealing choice. Nevertheless, the locally available RP may be of poor quality while the commercially available ones are expensive, making it unaffordable [29]. Consequently, HP is used as an alternative in TCT. The HP was 95.37% sensitive and with similar rates from 91% to 95% in comparison to femA PCR [12,29]. However, the use of HP is not perfectly efficacious despite of an overall high sensitivity. HP may contain anti-Staphylococcal agents which may interfere in the identification process and result in false negative outcomes [29]. Also, the lab personnel are at risk of contracting undetected HIV/AIDS, Hepatitis B and C [17,29,33]. Therefore, there is a need for an efficient test that may be helpful to overcome the drawbacks of TCT using RP or HP. This is the first reported study of HACCK to be used for identification of S. aureus. The HACCK exhibited 100% sensitivity, 100% specificity and 100% concordance with femA PCR.
In the present study, 81.23% isolates were mannitol positive while 18.77% were mannitol negative. Theoretically, coagulase positive strains of S. aureus are usually mannitol fermenters. However, 2.14% (n=6) femA positive isolates were mannitol negative. Kateete et al., have reported 6% S. aureus as MSA negative [29]. Shittu et al., have also reported MSA negative Methicillin Resistant S. aureus (MRSA). These false negative results may be due to genetic variation and/or lack of capability of S. aureus to ferment mannitol sugar [34]. Although, false positive results were not observed for MSA test in the present study, there are reports of some CoNS being mannitol fermenters [29,34]. This may be explained by the fact that these isolates can hydrolyse mannitol sugar in the media which forms the basis of identification of S. aureus isolates [35,36]. Therefore, the false negative or positive results can lead to wrong diagnosis or a delay in isolation and subsequent identification of S. aureus [29,34]. Another frequently used test for the detection of S. aureus is the DNase test. In the present study, 10 femA positive isolates were negative for DNase activity while few femA negative isolates were positive for the same. Similar findings have been reported earlier too with no explanation for these findings and thus, requires confirmation using an additional test [29,37–39]. In addition, there may be technical difficulties with regards to interpretation in case of weak positive reactions. Thus, DNase cannot be used as a single test for diagnosis of S. aureus which was evident with low concordance rate with PCR among other individual tests. The evaluation of combination tests revealed that HP with MSA and/or DNase had a low sensitivity similarly reported by Kateete et al., previously [29]. The combination of RP with MSA and/or DNase has not been reported elsewhere. A comparatively higher sensitivity was noted in the present study. Similarly, assessment of the HACCK with MSA and/or DNase is first of its kind and showed highest sensitivity percentage in comparison to RP and HP.
The HACCK test correctly identified all femA positives and femA negatives as S. aureus and CoNS respectively. In view of Cohen Kappa (κ) value, the HACCK was considered as a perfect test for identification of S. aureus. In addition to 100% specificity, sensitivity and concordance rate further advantages were observed. A greater percentage of isolates showed clot formation by the HACCK in less than three hours as against TCT using RP and HP (data not shown). The kit can be stored at room temperature with an extended shelf life, ready to use with minimal preparation time and reduced contamination sources. The number of tubes was reconstituted specifically for the number of samples to be tested which reduced the overall consumption of the kit. The TCT using RP or HP required a time consuming preparation time which included reconstitution of RP, thawing of HP from the frozen state to room temperature and dilution of the same. Also, RP once re-constituted can be stored for a maximum of 14 days at 2-4°C. The calculated cost of HACCK and TCT using RP for a single test was Rs.130-140 and Rs.150-160 respectively. The TCT using HP was cheaper at Rs.60-70 of a single test. The MSA, which had an almost perfect concordance rate of 98.24% with PCR may be used as an alternative test at a cost of 20-30 Rs. for a single test. Thus, MSA could be considered as a second line test for diagnosis of S. aureus and differentiation from CoNS. Also, keeping in mind the cost factor, MSA in combination with TCT using HP could be used as screening tests for diagnosis and confirm discordant results with the highly sensitive HACCK.
Limitation
The observation of clots by coagulase test was not checked between 4-24 hours. It has been reported that, S. aureus strains produce an enzyme called fibrinolysin along with coagulase, which can dissolve the clot formed from 4-24 hours and produce a false negative test when observed after 24 hours.
Conclusion
In view of the sensitivity, specificity and Cohen’s kappa value, the HACCK can be used as an effective tool with high level of confidence to diagnose S. aureus infections, overcome the problems of false positive result of CoNS species and reduce turnaround time for drug susceptibility testing and initiating therapy for the patient.