Cytohistological Features of Spindle Cell Lipoma- A Case Report with Differential Diagnosis
Yasmeen Khatib1, Archana L Khade2, Vinaya B Shah3, Manisha S Khare4
1 Associate Professor, Department of Pathology, HBT Medical College and Dr. R. N. Cooper Hospital, Juhu, Mumbai, Maharashtra, India.
2 Assistant Professor, Department of Pathology, HBT Medical College and Dr. R. N. Cooper Hospital, Juhu, Mumbai, Maharashtra, India.
3 Additional Professor, Department of Pathology, HBT Medical College and Dr. R. N. Cooper Hospital, Juhu, Mumbai, Maharashtra, India.
4 Professor, Department of Pathology, HBT Medical College and Dr. R. N. Cooper Hospital, Juhu, Mumbai, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Archana L Khade, Assistant Professor, Department of Pathology, C wing, 1st Floor, Hospital Building, HBT Medical College and Dr. R.N. Cooper Hospital, Juhu-400056, Mumbai, Maharashtra, India.
E-mail: arck115@gmail.com
Spindle Cell Lipoma (SCL) is an uncommon benign tumour of adipose tissue that is usually superficially located in the neck, back and shoulder region. Although it has characteristic histological features it can pose a diagnostic dilemma on cytology. It presents with a mixture of spindle cells, adipocytes, collagen fibres and a myxoid matrix in varying proportions sometimes with mild pleomorphism. Hence, it can be mistaken for other spindle cell, adipose and myxoid tumours which can be benign or malignant. We present a case of SCL of the back in a 47-year-old male, who presented with a slow growing lesion. Fine Needle Aspiration Cytology (FNAC) showed the characteristic cytological features described above and a diagnosis could be given after clinical correlation. We report this case as the cytology of this uncommon tumour has been described in relatively few cases and a correct pre-operative diagnosis will aid in proper management of this tumour.
Benign lipomatous tumour, Cytology, Histology
Case Report
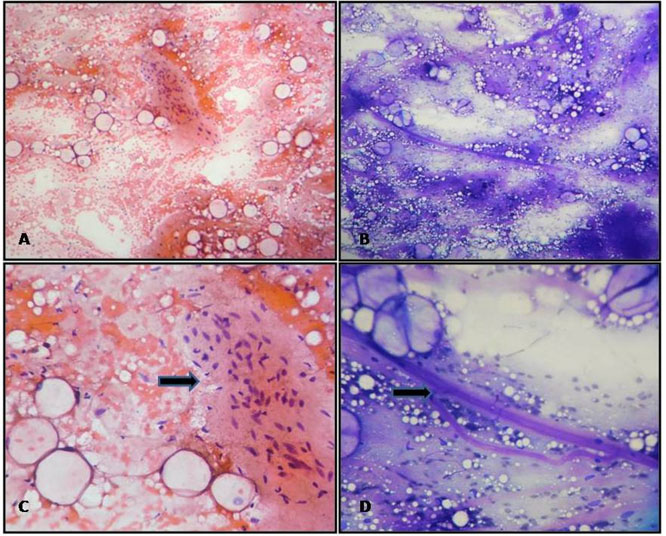
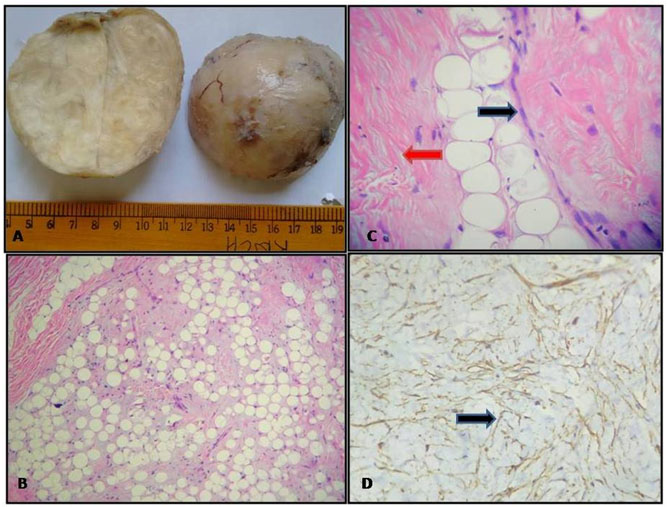
A 47-year-old male, presented to surgical Outpatient Department with the chief complaints of a gradually increasing swelling over the upper back since 15 years. On examination a 10x10cm, single globular swelling was seen over the upper back, just below the nape of neck. The swelling was firm, non-tender and mobile. Ultrasonography showed a heterogeneous, hyperechoeic lesion with few hypoechoeic areas beneath the subcutaneous plane with features suggestive of a benign soft tissue tumour likely to be a lipoma. The FNAC was performed using a 22 gauge needle attached to a 10ml syringe. Both alcohol fixed (95% alcohol) and air dried smears were prepared and stained with Giemsa and Papanicolaou stain respectively. The smears were cellular and showed mature adipocytes with clusters and few scattered spindle cells [Table/Fig-1]. Background showed abundant myxoid material and eosinophilic collagen fibres along with a few thin wall proliferating capillaries [Table/Fig-1]. Lipoblasts and mast cells were not seen. Based on the typical location and cytomorphological features, a diagnosis of SCL was given and excision was advised. Grossly a well circumscribed, capsulated mass was received measuring 8x8cm. On cut surface, it was homogenous, grey white with yellowish fatty and few glistening areas [Table/Fig-2a]. On microscopy, the tumour was composed of mature adipocytes admixed with spindle cells. The spindle cells had moderate eosinophilic cytoplasm with bland vesicular nuclei [Table/Fig-2b,c]. Many collagen bundles were seen along with myxoid matrix in the background [Table/Fig-2b,c]. No lipoblasts, mitosis or necrosis was seen. On Immunohistochemistry (IHC), the spindle cells were positive for CD34 [Table/Fig-2d]. A final diagnosis of SCL was made based on the histomorphological and IHC findings.
FNAC features of spindle cell lipoma: (a) Low power view showing adipocytes along with cohesive fragment of spindle cells. (PAP; 10X); (b) Low power view showing myxoid stroma with collagen fibers. (Giemsa; 10X); (c) High power view showing benign adipocytes with spindle cells having bland spindle and wavy nuclei (Arrow) (PAP; 40X); (d) High power view showing collagen fibers in bundles with adipocytes (Arrow) (Giemsa; 40X).
Histopathological features of spindle cell lipoma: (a) Gross appearance showing homogenous grey white tumour with, yellow areas; (b) Low power view showing many adipocytes, with spindle cells and myxoid background (H&E; 10X); (c) High power view showing bundles of collagen (red arrow) and traversing capillary; (Black arrow) (H&E; 40X) (d) Immunohistochemistry showing CD34 positive spindle cells. (Arrow) (10X)
Discussion
Although lipomatous tumours are the most common soft tissue tumours which undergo FNAC examination, experience in the aspiration of SCL is limited. The differentiation of this tumour from malignant lipomatous tumours and other spindle and myxoid lesions may be difficult both on cytology and histopathology. This may present as a diagnostic challenge especially while reporting FNAC of this lesion.
SCL is a rare type of benign adipose tissue tumour accounting for 1.5% of all lipomatous tumours [1]. It was first reported as a distinct entity in 1975 by Enzinger and Harvey [2]. It usually presents as a solitary, slow growing, and subcutaneous lesion usually arising in men of ages 40-70 years. Clinically it resembles a lipoma, but may be more firm in consistency. The common sites of involvement are the back, neck and shoulder region though other rare sites like tongue, cheek and oral cavity have also been reported [3–6].
Lew et al., have reported a case of SCL in the breast [3]. Agoff et al., have reported a case in the oral cavity [4], while Agarwal et al., and Fasig et al., had difficulty in distinguishing SCL of parotid from lipomatous pleomorphic adenoma [7,8]. Dominaski et al., have described the clinical radiological, cytological and cytogenetic features of this uncommon lesion in a series of 12 cases 8 located in the neck and one each on the tongue and cheek [1]. It was more common in men and they reported cases ranging between 27 years to 75 years. Clinically it presented in the subcutaneous location and measured 1.5cm to 4.5cm in diameter. Radiological features are variable and can show presence of a fatty or non-fatty tumour but give the superficial location. Cytological features described are presence of varying proportions of spindle cells, adipocytes, varying lengths of collagen fibres against a myxoid matrix. The spindle cells had pale poorly defined cytoplasm with ovoid basophilic nuclei showing mild anisonucleosis and absent nucleoli. Mast cells were seen in 50% cases and correlated with the myxoid matrix. All these features were present in the present case. The presence of few capillaries have also been reported in a few proportion of case which were absent in the present case. The spindle cells may show mild atypia in some cases which was absent in the present case.
On histology all three elements of adipocytes, spindle cells and collagen fibres are seen with a myxoid matrix and mast cells. On IHC the spindle cells are positive for CD34 and bcl2 which was seen in the present case. Loss of chromosome 13 and 16 has been found in cases of SCL on cytogenetic studies.
SCL presents with a range of differential diagnosis. FNAC of SCL rich in spindle cells can be mistaken for Neurilemmoma, Nodular fascitis or Dermatofibrosarcoma Proturberance (DFSP). Absence of fat, palisaded buckled nuclei with fibrillar matrix and IHC negative for CD34 but positive for S100 suggests a diagnosis of neural tumour. DFSP also has CD34 positive spindle cells but lacks adipocytes, myxoid matrix and collagen fibres. Nodular fascitis has a short history and shows plump myofibroblasts with active looking nuclei and mitosis. SCL with prominent myxoid matrix can be mistaken for myxoma, myxoid liposarcoma and low grade myxofibrosarcoma (MFS). Myxoma has scant cellularity with few stellate cells. Myxoid liposarcoma is a large deep seated lesion with many capillaries and lipoblasts. MFS can be a close differential but lacks adipocytes and is CD34 negative.
The treatment of SCL is complete surgical excision, together with the surrounding thin fibrous capsule. As SCLs are benign tumours, local recurrence is rare [2]. In our case, the patient been followed for 12 months and disease free without recurrence.
Conclusion
The present case highlights the fact that awareness of the classical cytological findings along with clinical and radiological correlation will help in the correct preoperative diagnosis of SCL leading to optimal management.
[1]. Domanski HA, Carlén B, Jonsson K, Mertens F, Akerman M, Distinct cytologic features of spindle cell lipoma. A cytologic-histologic study with clinical, radiologic, electron microscopic and cytogenetic correlationsCancer 2001 93:381-89. [Google Scholar]
[2]. Enzinger FM, Harvey DA, Spindle cell lipomaCancer 1975 36:1852-59. [Google Scholar]
[3]. Lew WY, Spindle cell lipoma of the breast: A case report and literature reviewDiagn Cytopathol 1993 9:434-37. [Google Scholar]
[4]. Agoff SN, Folpe AL, Grieco VS, Garcia RL, Spindle cell lipoma of the oral cavity. Report of a rare intramuscular case with fine needle aspiration findingsActa Cytol 2001 45:93-98. [Google Scholar]
[5]. Guo Z, Voytovich M, Kurtycz DF, Hoerl HD, Fine-needle aspiration diagnosis of spindle-cell lipoma: A case report and review of the literatureDiagn Cytopathol 2000 23:362-54. [Google Scholar]
[6]. Fletcher CD, Martin-Bates E, Spindle cell lipoma: A clinicopathological study with some original observationsHistopathology 1987 11:803-176. [Google Scholar]
[7]. Agarwal S, Nangia A, Lalita Jyotsna P, Pujani M, Spindle cell lipoma masquerading as lipomatous pleomorphic adenoma: A diagnostic dilemma on fine needle aspiration cytologyJ Cytol 2013 30(1):55-57. [Google Scholar]
[8]. Fasig HJ, Robinson RA, McCulloch TM, Fletcher MS, Miller CK, Spindle cell lipoma of the parotid fine-needle aspiration and histologic findingsArchives of Pathology and Laboratory Fine-Needle Medicine 2001 125:820-21. [Google Scholar]