Patient with Three Fallopian Tubes at Right Adnexa
Mustafa Gazi Uçar1, Tolgay Tuyan Ilhan2, Ayhan Gül3, Candan Korkutan4, Çetin Çelik5
1 Assistant Professor, Division of Urogynaecology, Department of Obstetrics and Gynaecology, Selçuk University Medicine Faculty, Selçuklu, Konya, Turkey.
2 Assistant Professor, Division of Oncology, Department of Obstetrics and Gynaecology, Selçuk University Medicine Faculty, Selçuklu, Konya, Turkey.
3 Assistant Professor, Division of Oncology, Department of Obstetrics and Gynaecology, Selçuk University Medicine Faculty, Selçuklu, Konya, Turkey.
4 Assistant Doctor, Division of General Gynaecology, Department of Obstetrics and Gynaecology, Selçuk University Medicine Faculty, Selçuklu, Konya, Turkey.
5 Professor, Division of Oncology, Department of Obstetrics and Gynaecology, Selçuk University Medicine Faculty, Selçuklu, Konya, Turkey.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Mustafa Gazi Uçar, Medical Doctor, Assistant Professor, Department of Obstetrics and Gynaecology, Selçuk University Medicine Faculty, Selçuklu, Konya-42075, Turkey.
E-mail: mustafa_gazi_ucar@hotmail.com
Accessory fallopian tube, Malformation, Mullerian anomaly, Urogenital
A 30-year-old woman, gravida 1 para 0, was referred to our high risk perinatology services for further assessment of an adrenal mass at 39 weeks’ gestation. On targeted sonography, an adrenal hemorrhage contained within the capsule of the gland, located superior to the left kidney measuring 12x20 mm was found. Additionally, because of breech presentation and intrauterine growth restriction the patient was scheduled to undergo an elective cesarean section. Her medical history was unremarkable. She had no history of previous surgery. She conceived spontaneously 2 months after her marriage.
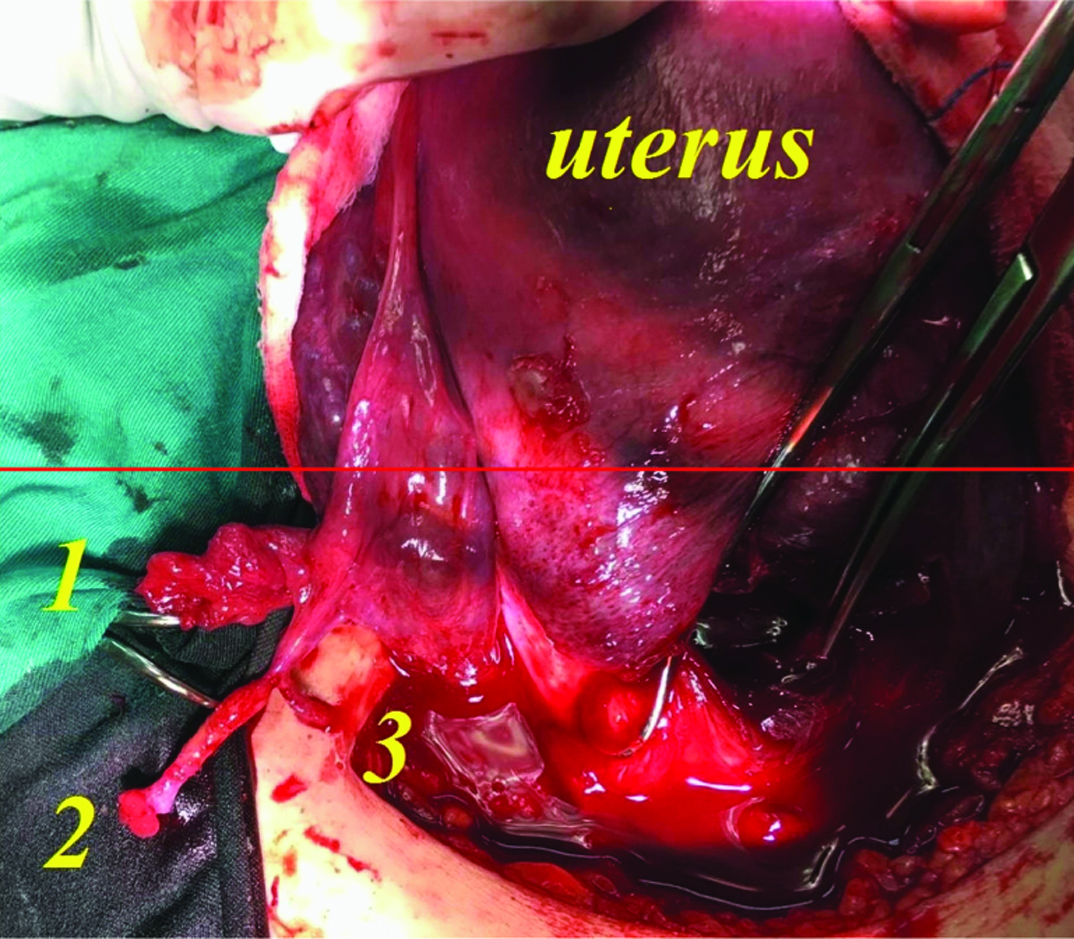
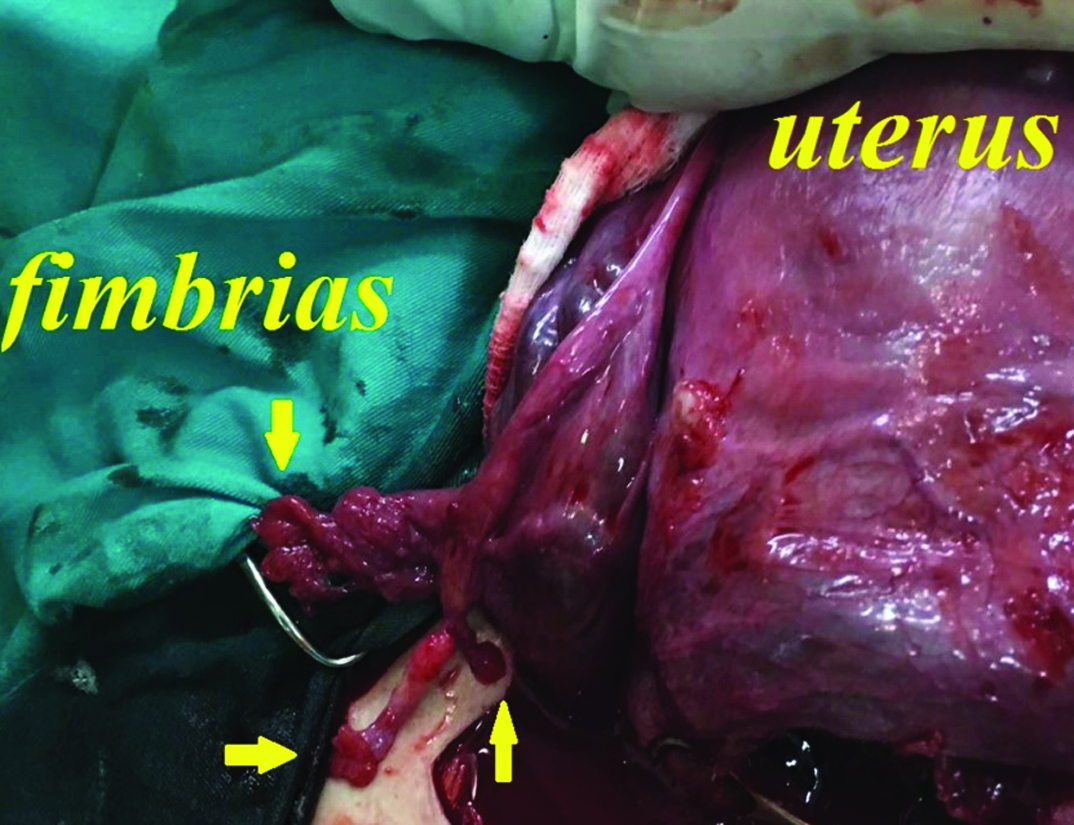
She underwent an uncomplicated caesarean section. However, during routinely checking for operating field, ovaries and fallopian tubes, interestingly there were 3 tubes at right side adnexa [Table Fig-1,2]. One of them was main tube in normal and usual size with normal continuation from the uterine cornua to the fimbrial end. Two thin, hypoplastic accessory tubes arising from the ampullary portion of main fallopian tube with their own fimbrias were noted. The lumen of second accessory tube was obliterated at its junction with the third accessory tube. On the left side, the fallopian tube and ovary were found to be normal.
Main tube (1) and two accessory fallopian tubes (2,3).
Two thin, hypoplastic accessory tubes arising from the ampullary portion of main fallopian tube with their own fimbrias (arrows).
During the embryologic development of the female urogenital system, the paramesonephric (Mullerian ducts) ducts fuse cranially from their caudal tips forming a tube with a single lumen known as the uterovaginal primordium which develops into the upper segment of vagina and the uterus. Many of these malformations are those resulting from varying degrees of failure of fusion of the paramesonephric ducts. Not surprisingly, these anomalies are more frequent in infertile women [1–3]. Although the true prevalence of accessory fallopian tubes in general population is unknown, a recent study found that the prevalence of accessory fallopian tubes was to be high as 1.9% in 1113 patients who underwent diagnostic laparoscopy for infertility work-up [1].
Accessory fallopian tube is a rare anatomical variation, which may rarely cause gynecological complications such as infertility, ectopic pregnancy, cystic swelling, torsion, and pyosalpinx [1]. For the prevention of these complications and to improve fertility outcomes some authors recommended surgical excision when they found incidentally [1,2]. How and why an accessory tube leading to infertility or ectopic pregnancy? It was described by Gandhi KR et al., with this possible mechanism of action in which ovary may also be captured by the fimbria of non-patent accessory tube instead of the main fallopian tubes [2]. Alternatively, the other entry may impair ciliary activity and adversely affect fluid transport mechanism of the oviduct [1].
In this case, both ovaries and uterus were normal and no renal anomalies were found. Similar to our case, Dahan MH et al., concluded that when congenital ampullary atresia occurs without concomitant mullerian anomalies, they would not be expected to be associated with an increase in renal abnormalities [3].
Anomalies of the fallopian tubes are rare and not always prominent. So, it may go unnoticed especially when they are asymptomatic. Systematic examination and appraisal of every oviduct during abdominal surgery may help to the identification and interpretation of such anomalies.
Financial Disclosure
The authors declared that this study has received no financial support.
[1]. Rottenstreich M, Smorgick N, Pansky M, Vaknin Z, Isolated torsion of accessory fallopian tube in a young adolescentJ Pediatr Adolesc Gynecol 2016 29:e57-58. [Google Scholar]
[2]. Gandhi KR, Siddiqui AU, Wabale RN, Daimi SR, The accessory fallopian tube: A rare anomalyJ Hum Reprod Sci 2012 5:293-94. [Google Scholar]
[3]. Dahan MH, Burney R, Lathi R, Congenital interruption of the ampullary portion of the fallopian tubeFertil Steril 2006 85:1820-21. [Google Scholar]