A Novel Technique to Overcome Treatment Delay Between Facemask Therapy and Comprehensive Orthodontic Correction
Jalis Fatima1, Subrata Saha2, Subir Sarkar3
1 Post Graduate Student, Pedodontics and Preventive Dentistry, Dr. R. Ahmed Dental College and Hospital, Kolkata, West Bengal, India.
2 Professor, Department of Pedodontics and Preventive Dentistry, Dr. R. Ahmed Dental College and Hospital, Kolkata, West Bengal, India.
3 Professor, Head of Department, Department of Pedodontics and Preventive Dentistry, Dr. R. Ahmed Dental College and Hospital, Kolkata, West Bengal, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Jalis Fatima, House No-9, West Row, Park Circus, Kolkata, West Bengal-700017, India.
E-mail: jlsfatima3@gmail.com
Protruded mandible, Retruded maxilla, Skeletal class III malocclusion
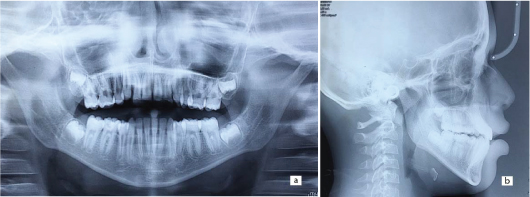
A 11-year-old boy presented to the Department of Pedodontics and Preventive Dentistry with the chief complaint of anterior crossbite. On clinical examination, he was found to have bilateral posterior crossbite and Class III molar relation with anterior crossbite [Table/Fig-1a-c] and small sized 24 which was unrestorable due to extensive caries and class V caries involving 46. On radiographic examination of Orthopantomogram (OPG), 13, 23, 35 and 45 were impacted in their respective quadrants due to arch length deficiency [Table/Fig-2]. Radiographic examination of lateral cephalogram revealed the last phase of growth period of patient by cervical vertebrae maturity indicators and the large Frankfurt Mandibular plane Angle (FMA) of 33° with short maxillary jaw base length [Table/Fig-3].
(a) Preoperative showing anterior crossbite; (b) Preoperative showing right side posterior crossbite; (c) Preoperative showing left side posterior crossbite.

Preoperative OPG showing impacted 13, 23, 35, 45.

Preoperative Lateral cephalogram.

After extraction of the non-restorable 24 and waiting period of three weeks for healing of extraction wound, a rapid maxillary expander of HYRAX (9mm) type was cemented which had hooks and posterior bite plate incorporated in its design to provide attachment for facemask elastics and release the trapped maxilla from mandible [Table/Fig-4]. The patient was instructed to turn the screw twice daily in the explained direction for one month. Following expansion, once the transverse correction was achieved, the same appliance was used to bring about maxillary protraction with facemask using 8 ounce elastic for three weeks and 14 ounce elastic for consecutive 6 months [Table/Fig-5]. After appreciable maxillary protraction by facemask was completed, even at the marginal growth period phase in this case, further consolidation and establishment of correct inter-arch relationship needed the employment of full bracket straight wire mechanics. The facemask therapy too needed sufficient retention period to prevent relapse. To save time of retention period and utilize it in employing straight wire mechanics, a contemporary appliance was customized by incorporating hooks for continued facemask usage as needed for retention and bite plate to separate maxillary and mandibular arch so that their individual dental correction by Mclaughlin Bennette and Trevisi (MBT) brackets could be undertaken. Before cementation of this novel appliance, 14, 34 and 44 were extracted to allow eruption of impacted 13, 35 and 45 in their respective quadrants.
Occlusal view of Bonded rapid maxillary expander.


This appliance was designed by customizing stainless steel bands on 15, 16, 25, 26. The bands on 15 and 16 were soldered with a 19 gauge (1mm) wire both bucally and palatally to add to the stability ratio of the appliance. A trans-palatal arch of two 19 gauge wires soldered together, was also soldered palatally to bands of 15 and 16. The same was done on 25 and 26. The entire setup was embedded in acrylic, again to add to the stability and anchorage of the appliance, for it to act as a whole unit and prevent any dissipation of unlikely forces onto any of the dental component [Table/Fig-6a-c]. After dental alignment of maxillary and mandibular arch, this appliance was removed and two arches were seen to have attained overjet and overbite which further aided in providing retention to the forwardly protracted maxilla.
(a) Intraoral frontal view with novel appliance and MBT brackets; (b) Lateral view with novel appliance; (c) Occlusal view of novel appliance.

The occlusal gap between the maxillary and mandibular posterior segments was allowed to close by passive eruption of the non bonded15, 16, 25, 26 while, segmental straight wire mechanics on 11, 12, 21, 22 and full arch straight wire mechanics (incorporating 35 and 45) was allowed to correct fine dental discrepancies [Table/Fig-7], 13 and 23 were allowed to erupt at their own place through active eruption into the dental arch and the brackets were removed taking all together only 13 months for the case to be completed including the retention phase [Table/Fig-8a-c].
Intraoral frontal view following removal of novel appliance.

(a) Intraoral frontal postoperative; (b) Right lateral postoperative and restored 46. (c) Left lateral postoperative.

Class III malocclusion has always been arduous in terms of understanding its cause, orthodontic treatment and post treatment retention. More so, if the underlying cause of class III malocclusion gathers up to be skeletal in origin, then its treatment and more importantly its retention oodles abundant concern on the clinician. Skeletal class III malocclusion was formerly thought to be due to mandibular prognathism [1]. Lately, maxillary retrusion has been culminated as a notable cause of skeletal class III malocclusion. Whenever, maxilla falls into the offender for skeletal class III malocclusion, it can either be because of retruded sagittal maxillary position and/or short maxillary jaw base length [2]. Sue et al., and Guyer EC et al., reported 62% and 63% of their patients with class III malocclusion having retruded maxilla respectively [3,4]. In case of maxillary retrusion, facemask which is an orthopedic appliance, has evolved to be of sizeable help not just in primary or early mixed dentition, but also in late mixed and early permanent dentition period. The obvious disadvantage of retention by any orthopedic appliance is not ruled out in case of facemask therapy too, but the retention phase of facemask therapy can be used to simultaneously carry out comprehensive orthodontic treatment (if needed) in second phase following facemask to settle the intra arch dental discrepancies.
The large FMA and the early permanent dentition phase in which the patient reported and had to be treated, made it grueling for the clinician to undertake treatment using facemask. Also, the concern regarding increased facial height due to further unstoppable downward and backward growth of mandible as a part of facemask therapy made results all the more unpredictable. The appreciable anterior displacement of maxilla was achieved using facemask therapy. The maxillary occlusal plane rotated clockwise with increased anterior facial height and decreased posterior facial height as a result of concurrent orthopedic and orthodontic correction when compared to their preoperative values [Table/Fig-9a,b]. To limit the vertical facial height during the facemask therapy, the elastics were oriented parallel with the occlusal plane and not 20° to it [5,6]. With the course of treatment, FMA was seen to have shown an increase from 33°-37° only [Table/Fig-10]. The remaining notorious growth of mandible if could catch up in future and be a cause of relapse can not certainly be concluded in this case, as with any other treatment modality.
(a) OPG postoperative; (b) Lateral Cephalogram postoperative.
Pretreatment and post treatment cephalometric readings.
| DCP | LC-DCP | LCP |
|---|
| SNA | 83.5 | 85 |
| SNB | 88 | 84 |
| AFH | 105mm | 107mm |
| PFH | 68mm | 63mm |
| MxBL | 76mm | 79mm |
| MnBL | 113mm | 106mm |
| MOLAR RELATION | CLASS-III | CLASS-I |
A pristine treatment approach used for correction of orthopedic and orthodontic class III mal-relation using a novel appliance resulted in favourable, stable and desired results by cutting down the treatment duration (which includes in it the retention period of facemask) to as low as 13 months.
[1]. Ellis EE 3rd, McNamara JA Jr, Components of adult Class III malocclusionJ Oral Maxillofac Surg 1984 42:295-305. [Google Scholar]
[2]. Scala A, Auconi P, Scazzocchio M, Caldarelli G, McNamara JA, Franchi L, Using networks to understand medical data: The case of class III malocclusionsPLoS One 2012 7:e44521 [Google Scholar]
[3]. Sue G, Chacona SJ, Turley PK, Itoh J, Indicators of skeletal Class III growthJ Dent Res 1987 66:S343 [Google Scholar]
[4]. Guyer EC, Ellis EE, McNamara JA, Behrents RG, Components of Class III malocclusion in juveniles and adolescentsAngle Orthod 1986 56:7-30. [Google Scholar]
[5]. Ciaburro H, Dupont C, Prevost Y, Cloutier G, Forward traction in the correction of retrodisplaced maxillaCan Med Assoc J 1973 108:1511-14. [Google Scholar]
[6]. Kambara T, Dentofacial changes produced by extraoral forward force in the Macaca virusAm J Orthod 1977 71:249-77. [Google Scholar]