Unusual Presentation of Prostate Carcinoma: A Case Report
Rohit Bhattar1, Anuradha Maheshwari2, Sher Singh Yadav3, Vinay Tomar4
1 Resident, Department of Urology, SMS Medical College, Jaipur, Rajasthan, India.
2 Clinical Associate, Department of Anaesthesia, EHCC, Jaipur, Rajasthan, India.
3 Professor and Head, Department of Urology, SMS Medical College, Jaipur, Rajasthan, India.
4 Professor, Department of Urology, SMS Medical College, Jaipur, Rajasthan, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rohit Bhattar, RD Hostel Room No F 61, SMS Medical College, Jaipur-302004, Rajasthan, India.
E-mail: bhattarrohit@gmail.com
Prostate cancer is a common cancer in elderly men and it frequently metastasizes to regional lymph nodes and sometimes to bone. Very rarely in some of the cases it also shows involvement of non-regional lymph nodes like supra-diaphragmatic lymph nodes. In our report, we present a 60-year-old male, initially misdiagnosed as Chronic Obstructive Pulmonary Disease (COPD) with cervical lymph node involvement may be due to infective region or inflammatory pathology, which was later found to have prostatic adenocarcinoma metastatic to supraclavicular lymph nodes. Very less case reports are present which have shown similar presentations. So we would like to highlight that prostatic carcinoma can be present in an atypical form also.
Atypical form, Lymphnode, Supraclavicular
Case Report
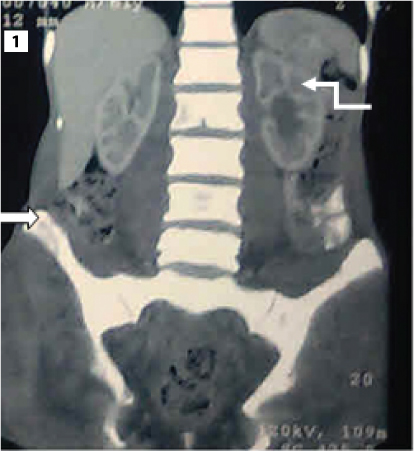
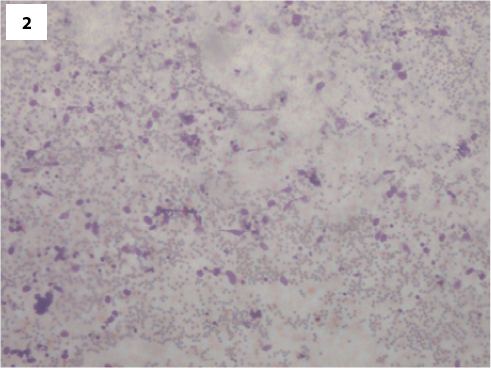
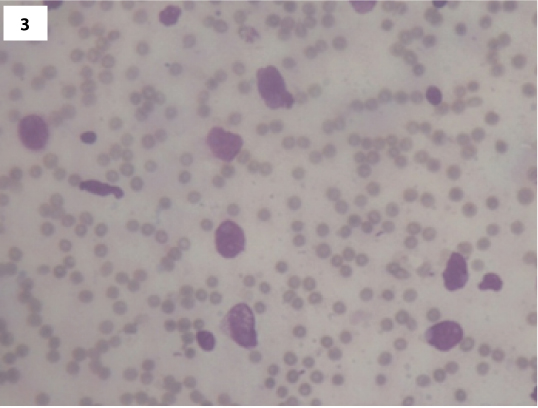
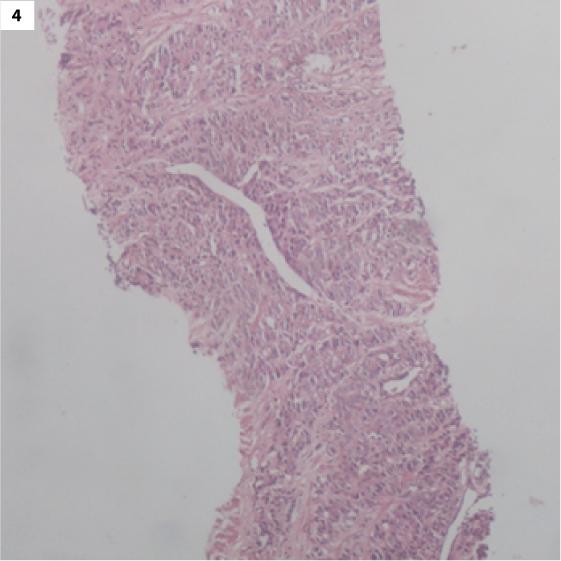
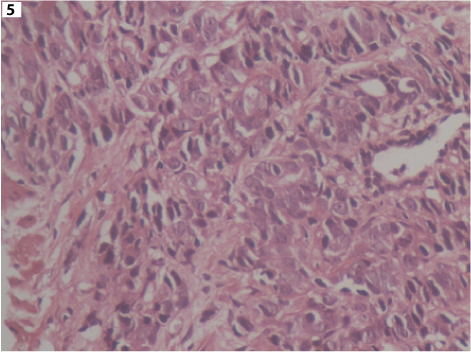
A 60-year-old male was referred to medicine department, initially for difficulty in breathing with palpable painless left cervical mass, a chest X-ray was done, which showed COPD changes. He also complained of eight kg weight loss, anorexia and weakness for approximately four months. He denied any other subjective complaints including difficulty in swallowing, bone pain or urinary symptoms. Physical examination was unremarkable except for an approximately 2 cm nontender, firm mass in left cervical region, fixed to underlying structures. Patient’s past history was unremarkable for any other surgical history or malignancy. His family history was non contributory. During initial evaluation Digital Rectal Examination (DRE) and serum Prostate Specific Antigen (PSA) was not done. Subsequently HRCT thorax and CECT whole abdomen was done which showed possibility of skeletal metastasis and left hydroureteronephrosis [Table/Fig-1]. USG guided FNAC of left supraclavicular node was done which showed possibility of adenocarcinoma [Table/Fig-2,3] which was immunohistochemically positive for PSA staining. Subsequently patient was referred to our department of urology and DRE and PSA was done. DRE showed bilateral hard, fixed and enlarged lobes of prostate. Serum PSA was >100 ng/ml. Biopsy of prostate was done which revealed moderately differentiated carcinoma of prostate with Gleason grade 4+3=7 [Table/Fig-4,5].
Coronal CT scan showing left hydronephrosis and vertebral lesion (curved arrow showing hydronephrosis and straight arrow showing vertebral lesion);
FNAC specimen of neck mass (lymph node) under low magnification (10 x) showing malignant appearing cells.
FNAC specimen of neck mass (lymph node) under high magnification (40 x) showing malignant appearing cells.
Histopathological specimen showing moderately well differentiated adenocarcinoma of prostate (10 x).
Histopathological specimen showing moderately well differentiated adenocarcinoma of prostate (40 x).
Detailed discussion with the patient was done and he declined any further investigations (bone scan) and opted for surgical treatment (bilateral orchidectomy). In addition to this, patient was also treated with tab bicalutamide 50 mg once daily. Patient was followed up at regular intervals. His symptoms subsided and PSA decreased to <1 ng/ml. At 12 months follow up he remains asymptomatic on androgen blockade.
Discussion
Prostate cancer is the second most frequently diagnosed cancer of men after lung cancer and the fifth most common cancer worldwide [1]. The axial skeleton, the nodes of the pelvis and the retroperitoneum are the most frequent sites of metastasis [2]. Cervical lymph node involvement can be due to various reasons like inflammation, lymphoma or metastasis. Prostatic carcinoma generally metastasizes to regional lymph nodes and bone however in some cases it can present in many forms and one of the aspect is presentation in the form of neck mass as shown in this report. Cervical lymphadenopathy can be the initial presentation of prostatic carcinoma in very rare cases. The aim of our case report was to share our experience and focus on an unusual presentation of prostate cancer.
Many theories suggest the mechanism of metastasis to the supradiaphragmatic lymph nodes from genito-urinary malignancy. It has been suggested that cancer cells can lodge in the nodes, near to entry of thoracic duct into left subclavian vein by retrograde spread and this mechanism may be responsible for supra-diaphragmatic spread of prostatic cancer [3]. Haematogenous spread via the vertebral venous plexus fails to explain the predilection of this carcinoma to metastasize to the left cervical region, whilst right side involvement is extremely uncommon [4]. Prostate carcinoma can also present in various atypical forms like huge abdominal lump, osteolytic bone metastasis, peritoneal metastasis, malignant ascites [4–7]. Rarely, it can also manifest its initial presentation in the form of pneumothorax or anejaculation [8,9]. However, asymptomatic neck mass is more common atypical presentation and some of the case reports had presented these kind of manifestation [3,4,10–12].
In the present report, patient had left supraclavicular lymphadenopathy with bone metasatsis without having any other lymph node involvement. Unilateral involvement of cervical lymphnode is more favorable of lymphatic spread in contrast to hematogenous spread in which bilateral involvement is more common. It was suggested that prognosis of such kind of cases is generally poor but Wang et al., followed such cases for 16 months and in their series none of the cases showed progression [3]. Similarly, we also did follow up for 12 month and in this period our patient was clinical and biochemically quiescent. However, this can be one of the limitations because carcinoma prostate is slow growing disease and if patient is followed for a long duration then results can change. Serum PSA and DRE are the two most important methods for diagnosis of prostatic carcinoma and in our report PSA and DRE was done after the FNAC of neck mass, not at the initial stage. So our case report again highlights the fact that Serum PSA and DRE should be considered in patients that present with such manifestations.
Conclusion
Prostate carcinoma is considered to be a disease of old age and can surprise clinicians by its various manifestations. So any patient (specially elderly) presenting with a asymptomatic neck mass with an unknown primary even in the absence of urinary symptoms should be considered as a potential candidate for DRE and PSA estimation. Despite the rare presentation of prostatic carcinoma in such forms, clinicians should have high index of suspicion coupled with having low threshold for investigations for early and proper diagnosis of this disease and timely management.
Informed Consent: Written informed consent was obtained from patient for presentation of this case.
[1]. Ferlay AJ, Shin HR, Bray F, Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008J Int Cancer 2010 127(12):2893-917. [Google Scholar]
[2]. Carleton J, Vander Riet P, Dahm P, Metastatic prostate cancer presenting as an asymptomatic neck massProstate Cancer Prostatic Dis 2005 8(3):293-95. [Google Scholar]
[3]. Wang HJ, Chiang PH, Peng JP, Yu TJ, Presentation of prostate carcinoma with cervical lymphadenopathy: report of three casesChang Gung Med J 2004 27:840-44. [Google Scholar]
[4]. Singh I, Advanced metastatic prostate cancer presenting as a huge abdominal lumpIndian J Surg 2003 65:279-80. [Google Scholar]
[5]. Sepúlveda L, Gorgal T, Pires V, Rodrigues F, Prostate cancer metastatic to the cervical lymph nodesCase Reports in Urology 2015 2015:263978 [Google Scholar]
[6]. Segamwenge IL, Mgori NK, Abdallah Yussuf S, Mukulu CN, Nakangombe P, Ngalyuka PK, Cancer of the prostate presenting with diffuse osteolytic metastatic bone lesions: a case reportJournal of Medical Case Reports 2012 6:425 [Google Scholar]
[7]. Petrakis D, Pentheroudakis G, Kamina S, Pappa L, Papadiotis E, Malamou-Mitsi V, An unusual presentation of a patient with advanced prostate cancer, massive ascites and peritoneal metastasis: Case report and literature reviewJournal of Advance Research 2015 6(3):517-21. [Google Scholar]
[8]. Chianga KH, Hung SH, Chang ST, Pneumothorax as a presenting clinical manifestation of metastatic prostate cancerWorld J Oncol 2013 4(2):118-21. [Google Scholar]
[9]. Mufti U, Ghani KR, Samman R, Virdi J, Potluri B, An ejaculation as an atypical presentation of prostate cancer: a case reportCases J 2008 1:81 [Google Scholar]
[10]. Vaughn C, Jaqua K, Meacham R, Vieira F, The presenting symptom of metastatic prostate carcinoma: case of a large supraclavicular mass and review of literatureInternational Journal of Otolaryngology and Head & Neck Surgery 2013 2(5):207-10. [Google Scholar]
[11]. Dubhashi SP, Kumar H, Nath SR, Prostate cancer presenting as cervical lymphadenopathyAm J Case Rep 2012 13:206-08. [Google Scholar]
[12]. Elabbady A, Kotb AF, Unusual presentations of prostate cancer: A review and case reportsArab Journal of Urology 2013 11(1):48-53. [Google Scholar]