Application of CAD-CAM for Fabrication of Metal-Free Band and Loop Space Maintainer
Harleen Kaur Soni1
1 Senior Lecturer, Pedodontics and Preventive Dentistry, Manubhai Patel Dental College, Vadodara, Gujarat, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Harleen Kaur Soni, B-401, Radhey Residency, Manjalpur, Vadodara-390005, Gujarat, India.
E-mail: drharleensoni@gmail.com
An ideal occlusion with proper tooth alignment and fully functional teeth is the ultimate goal of all dental treatments. Premature extraction of deciduous teeth is a common sequeale of untreated dental caries in teeth in which the damage is far beyond repair. Premature extraction might lead to loss of space for the successor tooth, drifting of teeth and loss of arch integrity leading to malocclusion in the permanent teeth. To prevent the space loss, space maintainers are designed and delivered at the time of extraction to allow for development of proper functional occlusion in children till the eruption of the succedaneous permanent tooth. A six-year-old female patient with chronic intra-radicular abscess in upper right first primary molar was treated with extraction followed by the placement of BruxZir zirconia space maintainer. Clinical and radiographic examinations were performed at one and six months. At the end of six months, the patient was completely asymptomatic and there were no visible signs of gingival inflammation and tissue irritation at the site of the space maintainer.
BruxZir, Extraction, Pulp necrosis, Space maintainer
Case Report
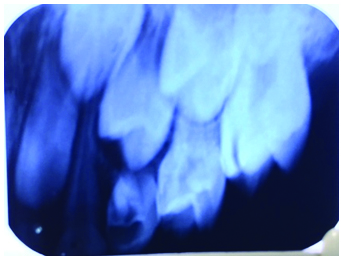
A six-year-old female patient reported to the Department of Pedodontics and Preventive Dentistry, Manubhai Patel Dental College, Vadodara, Gujarat with chief complaint of pain in the upper right back tooth since 15 days. On clinical examination, there was presence of a large deep carious lesion involving the right maxillary primary first molar. There was an associated sinus opening adjacent to the involved tooth about 2 cm above the free gingival margin on the buccal side. The patient had a history of severe pain on intake of hot and cold fluids 15 days back which relieved on its own without any intervention. There was a history of intraoral swelling five days back which subsided on intake of medications. There was no tenderness on percussion. Diagnostic tests revealed negative response to hot and cold tests. Electric Pulp Testing (EPT) results showed no response in the involved tooth as compared to the contralateral healthy tooth. Radiographic examination revealed presence of a large radiolucency in the coronal portion of the involved tooth involving the pulp with complete resorption of mesial and distal roots [Table/Fig-1]. On the radiograph, only the crown of the permanent first premolar was seen to have formed with no signs of root formation. After complete clinical and radiographic examination, a diagnosis of chronic intra-radicular abscess was made for the involved tooth. Extraction of the tooth followed by a ceramic space maintainer was decided as the treatment plan.
Preoperative radiograph of 54 showing a deep carious lesion with resorption of distal and palatal roots;
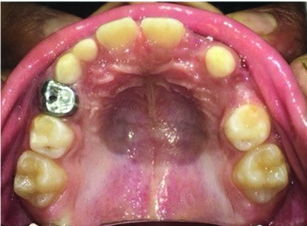
The tooth was anaesthetized with 2% lidocaine with 1:2,00,000 adrenaline and extraction was performed. The patient was prescribed antibiotics and analgesics for the same. The patient was recalled after one day for evaluation of postoperative pain and swelling. Seven days postextraction [Table/Fig-2], impression of the upper and lower arches was made with elastomeric impression material. The impression was sent to the lab for fabrication of space maintainer. BruxZir zirconia was the material of choice for fabrication of the space maintainer. BruxZir is a solid monolithic zirconia material which utilizes CAD/CAM technology for its designing and milling of the restoration. A gingival shade was added to the appliance to make it more aesthetically pleasing [Table/Fig-3].
Intraoral photograph seven days postextraction.
BruxZir space maintainer appliance on the dental cast;

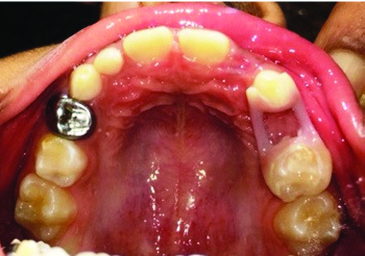
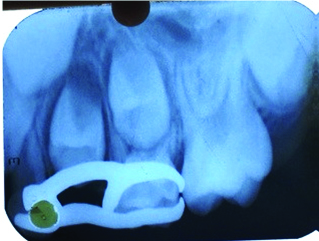
The gingival one-third of the distal surface of canine and gingival one-third of the mesial surface of the primary second molar etched with phosphoric acid for 15 seconds. After water rinse and drying, the hybridization was achieved by using two step etch and rinse adhesive system (Adper Single Bond 2, 3M/ ESPE). The adhesive layer was polymerized during 15 seconds. The inner surface of the space maintainer was cemented with the help of resin luting cement (RelyX ARC – self adhering flowable composite, 3M/ESPE) [Table/Fig-4]. Intraoral radiograph of appliance immediately after placement was taken [Table/Fig-5]. The patient was given instructions for oral hygiene and was asked to report in case of any discomfort or loosening of the appliance. The patient was followed up after one and six months.
BruxZir space maintainer appliance in the patient’s mouth immediately after Placement.
Intraoral radiograph of appliance immediately after placement.
After six months, the patient was completely asymptomatic. No signs of gingival inflammation and tissue irritation were seen at the site of the space maintainer. The patient had no difficulty in mastication [Table/Fig-6].
Intraoral photograph 6 months after placement of appliance.

Lab Procedure: BruxZir is a CAD/CAM-fabricated material and has to be digitally designed by a technician using a digital scanner and design software. The file was “nested” or positioned in the zirconia disk and milled to a full contour approximately 30 percent larger than the final restoration. Once the restoration was milled and removed from the disk, it was dipped in the appropriate coloring solution and sintered in an oven for 6.5 hours at 1,530 degrees Celsius where it shrunk to its final size. The gingival shade was added in the area of the missing tooth to enhance aesthetics [1].
Discussion
One of the critical function of primary teeth is maintenance of space for the successional permanent teeth. Space maintainers are a routine appliance used in paediatric dentistry for proper maintenance of space for the succedaneous permanent tooth in case of early removal of the primary tooth.
A space maintainer was advocated in the present case as the intraoral periapical radiograph revealed an incompletely formed first premolar where the crown of the tooth was almost completed (Nolla’s stage 5) with no sign of root formation. Since, teeth do not erupt till two-thirds of the root is completed (Nolla’s stage 8) thereby, a space maintainer was absolutely necessary. Also, the eruption of the first permanent molar was not to its full occlusal level and it might cause forces on the primary second molar causing the tooth to drift in the space of the first primary molar which was extracted, leading to blockage of the first permanent premolar [2].
Premature loss of primary molars also cause a reduction in arch length. According to Northway WM, when the maxillary primary first molar is lost prematurely, the first premolar erupts in a more mesial direction than normal, due to the mesial incline of the primary second molar, and consumes the space of the permanent canine, which becomes blocked out, exhibiting a more deleterious effect [2]. In a study by Richardson, he stated that maximum amount of space loss occurs in the first six months post extraction [3]. Hence, the space maintainer was recommended immediately after extraction of the tooth.
Various space maintainers as band and loop, crown and loop and lingual arch space maintainers are routinely used in dentistry. Certain disadvantages as corrosion and appliance fracture, have led to the development of more aesthetic and metal-free space maintainers which include Fibre Reinforced Composite Resin (FRCR) space maintainer and CAD-CAM aided ceramic band and loop space maintainer. The comparison between the aesthetic space maintainers is depicted in [Table/Fig-7].
Comparison of FRCR and new CAD-CAM designed ceramic space maintainer.
| Sr No. | Criteria | FRCR SpaceMaintainer | CAD-CAM guidedCeramic Space Maintainer |
|---|
| 1. | Patient Visits | One Visit | Two Visit |
| 2. | Tooth Preparation | Not required | Not required |
| 3. | Finishing and Polishing | Required during appliance cementation | None |
| 4. | Cause of Failure | Debonding commonly seen at enamel composite interface | No Debonding seen |
| 5. | Lab Procedures | No lab work | Space maintainer prepared in the lab |
| 6. | Patient Acceptability | Good | Good |
Bishara SE et al., and Agaoglu G et al., reported that orthodontic appliances, used in oral cavity corrode in the oral environment releasing both nickel and chromium [4,5]. Patients have reported to have metal allergies in the form of gingivitis, burning sensation, gingival hyperplasia, numbness on sides of tongue especially to nickel present in space maintainers and stainless steel crowns [6–8]. Bhaskar VB and Reddy WS in their study have reported that base metal alloys used in the paediatric dentistry in stainless steel crowns and band and loop space maintainers release measurable amount of the nickel ranging from (3.65 to 6.88 ppm for Crowns, 4.95 to 7.78 ppm for Space Maintainer) and chromium (0.48 to 3.76 ppm for Crowns, 0.70 to 4.54 ppm for Space Maintainer) in an artificial salivary medium [9]. Also, the amount of nickel ion release is more in space maintainers than in stainless steel crowns [6,9]. The amount of nickel release has been seen to be more in females as compared to males [10,11]. Hence, an attempt to make a metal-free ceramic space maintainer i.e., BruxZir was done.
BruxZir zirconia has high flexural strength (up to 1,465 MPa) and exhibits three to five times the fracture toughness of typical zirconia. This property gives it high impact resistance to the high masticatory forces in the mouth. It also has excellent resistance to thermal shock with a low thermal expansion which means the restorations will remain stable in the mouth on intake of hot and cold fluids. BruxZir is available in all the vita classic and gingival shades which would fulfill the aesthetic demands of the patient [1]. Hence, BruxZir was considered as the ideal material for fabrication of the space maintainer.
The design of the space maintainer was such that it was supported by the both the canine and the primary second molar to allow for better retention of the appliance and also to prevent tipping of the teeth. The masticatory forces applied in the region of the extracted tooth would be equally distributed on the canine and second primary molar preventing it from getting dislodged. The gingival loop was kept close to the gingiva to prevent food lodgment in the area.
A resin luting cement (conventional or self-adhesive resin cements) is the material of choice for cementation of all-ceramic restorations. Conventional resin cement bond well to enamel in contrast to the self etch resin cements which bond well to dentine [12,13]. As the entire appliance had to be cemented on the enamel surface, conventional resin cement as RelyX ARC was used for cementation due to proper bond strength and marginal sealing [14, 15].
The ceramic space maintainer seems to be a viable alternative to the conventional band and loop space maintainer. The advantages and disadvantages are mentioned in [Table/Fig-8].
Advantages and disadvantages of the new CAD-CAM designed space maintainer.
| Sr No. | Advantages | Disadvantages |
|---|
| 1. | High strength due to monolithic design | Expensive |
| 2. | No gingival lacerations and trauma as no band pinching required | Lab support required |
| 3. | No nickel allergy and corrosion | Expertise needed for fabrication |
| 4. | Tipping of teeth prevented as there is tooth support on both sides | Costly equipment required |
Conclusion
The ceramic space maintainer seems to be a suitable alternative to the conventional band and loop space maintainer. The appliance is well tolerated by the patient and also gives the benefit of advanced aesthetics with improved strength. Since, the material and design of the appliance was the first of its kind, further clinical studies are needed to verify the success of the new space maintainer over increased periods of observation time.
[1]. Mcomie M, Aesthetic Long-Span Bridge Using BruxZirDental Tribune Middle East & Africa Edition September - October 2013 [Google Scholar]
[2]. Northway WM, The not-so-harmless maxillary primary first molar extractionJ Am Dent Assoc 2000 131:1711-20. [Google Scholar]
[3]. Richardson The relationship between the relative amount of space present in the deciduous dental arch and the rate and degree of space closure subsequent to the extraction of the deciduous molarDent Pract (Bristol) 1965 16:111-18. [Google Scholar]
[4]. Bishara SE, Barrett RD, Selim MI, Biodegradation of orthodontic appliances. Part II. Changes in the blood level of nickelAm J Orthod Dentofacial Orthop 1993 103(2):115-19. [Google Scholar]
[5]. Ağaoğlu G, Arun T, Izgi B, Yarat A, Nickel and chromium levels in the saliva and serum of patients with fixed orthodontic appliancesAngle Orthod 2001 71(5):375-79. [Google Scholar]
[6]. Kulkarni P, Agrawal S, Bansal A, Jain A, Tiwari U, Anand A, Assessment of nickel release from various dental appliances used routinely in paediatric dentistryIndian J Dent 2016 7:81-85. [Google Scholar]
[7]. Chaturvedi TP, Upadhayay SN, An overview of orthodontic material degradation in oral cavityIndian J Dent Res 2010 21(2):275-84. [Google Scholar]
[8]. Noble J, Ahing SI, Karaiskos NE, Wiltshire WA, Nickel allergy and orthodontics, a review and report of two casesBr Dent J 2008 204(6):297-300. [Google Scholar]
[9]. Bhaskar VB, Reddy VVS, Biodegradation of nickel and chromium from stainless steel crowns and space maintainers - an in vitro studyAnnals Dent Univ Malaya 1997 4:17-21. [Google Scholar]
[10]. Leenen RL, Kuijpers-Jagtman AM, Jagtman BA, Katsaros C, Nickel allergy and orthodonticsNed Tijdschr Tandheelkd 2009 116(4):171-78. [Google Scholar]
[11]. Feasby WH, Ecclestone ER, Grainger RM, Nickel sensitivity in paediatric dental patientsPaediatr Dent 1988 10(2):127-29. [Google Scholar]
[12]. Abo-Hamar SE, Hiller KA, Jung H, Federlin M, Friedl KH, Schmalz G, Bond strength of a new universal self-adhesive resin luting cement to dentin and enamelClin Oral Investig 2005 9:161-67. [Google Scholar]
[13]. Anchieta RB, Rochaa EP, Almeida EO, Freitas Junior AC, Martini AP, Bonding All-Ceramic Restorations with Two Resins Cement Techniques: A Clinical Report of Three-Year Follow-UpEur J Dent 2011 5:478-85. [Google Scholar]
[14]. Hikita K, Van Meerbeek B, De Munck J, Ikeda T, Van Landuyt K, Maida T, Bonding effectiveness of adhesive luting agents to enamel and dentinDent Mater 2007 23(1):71-80. [Google Scholar]
[15]. Baroni C, Franchini A, Rimondini L, Survival of different types of space maintainersPaediatr Dent 1994 16(5):360-61. [Google Scholar]