Paediatric Post-Traumatic Bladder Neck Distraction Injury: Case Series
Ajit S. Sawant1, Lomesh A. Kapadnis2, Vikash Kumar3, Prakash Pawar4, Ashwin S. Tamhankar5
1 Professor and Head, Department of Urology, Lokmanya Tilak Municipal Medical College and Hospital, Mumbai, Maharashtra, India.
2 Senior Resident, Department of Urology, Lokmanya Tilak Municipal Medical College and Hospital, Mumbai, Maharashtra, India.
3 Associate Professor, Department of Urology, Lokmanya Tilak Municipal Medical College and Hospital, Mumbai, Maharashtra, India.
4 Assistant Professor, Department of Urology, Lokmanya Tilak Municipal Medical College and Hospital, Mumbai, Maharashtra, India.
5 Senior Resident, Department of Urology, Lokmanya Tilak Municipal Medical College and Hospital, Mumbai, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Lomesh A. Kapadnis, Department of Urology, Room No 219, 2nd Floor, College Building, Lokmanya Tilak Municipal Medical College, Sion, Mumbai-400022, Maharashtra, India.
E-mail: drlomeshkapadnis@gmail.com
The bladder neck distraction is a rare posterior urethral injury in paediatric age group. It mostly occurs secondary to road traffic accidents. We report three cases of paediatric bladder neck distraction injury. Three paediatric patients aged between 4 to 7 years (mean 5 year), who presented with post traumatic bladder neck distraction injury but no other major injury, they were treated with early urethro-vesical anastomosis. Postoperatively all patients were continent and with good urine flow rates. In paediatric bladder neck distraction injury, immediate urethro-vesical anastomosis gives good results.
Bladder neck injury, Paediatric injury, Urethral injury
Case Series
We report our experience of three paediatric patients aged between 4 to 7 years, who presented with post traumatic bladder neck distraction injury from 2008 to 2015. All 3 patients presented within 6 hours of injury with associated pelvic fracture, inability to pass per urethral catheter and blood at meatus. In all patients, there were no major intra-abdominal solid organ injuries, were haemodynamically stable and had extravasation of contrast on Contrast Enhanced Computed Tomography (CECT) in the region of bladder neck [Table/Fig-1]. All patients had Type 4 urethral injury according to Goldman Modification of Colapinto and McCallum classification of Urethral Injury [Table/Fig-2] [1]. All patients on presentation were first stabilized with intravenous fluids. Prophylactic antibiotics were given preoperatively. All patients were operated within first 12 hours of presentation with midline infraumbilical exploratory laparotomy.
| Characteristic | Patient-1 | Patient-2 | Patient-3 |
|---|
| Age | 5yr | 6yr | 4yr |
| Sex | Male | Male | Female |
| Time of presentation | 1hr | 3hr | ½ hr |
| Pulse (per minute) | 120 | 116 | 110 |
| BP (mm of Hg) | 90/60 | 94/66 | 90/66 |
| Hb (gm/dL) | 10.1 | 11 | 9.0 |
| Creatinine (mg/dL) | 0.5 | 0.7 | 0.5 |
| Associated pelvic fracture | Yes | Yes | Yes |
| Associated abdominal injury | No | No | No |
| CT scan | Defect of 5mm at bladder base with leakage of contrast in a paravesical collection of 4.5 x 3.5 cm | Rent at bladder base with extravasation of contrast in paravesical space.[Table/Fig-3] | Small defect in anterior wall of bladder at bladder base with leakage of contrast extraperitoneally. [Table/Fig-4] |
Goldman Modification of Colapinto and McCallum classification of urethral injury [1].
| Class | Description |
|---|
| I | Posterior urethra stretched but intact |
| II | Tear of the prostatomembranous urethra above the urogenital diaphragm |
| III | Partial or complete tear of both the anterior and posterior urethra with disruption of the urogenital diaphragm |
| IV | Bladder neck injury extending into the urethra |
| IVa | Injury of the bladder base with peri-urethral extravasation simulating posterior urethra injury |
| V | Partial or complete pure anterior urethral injury. |
Two patients had complete disruption of the posterior urethra from the bladder at the level of bladder neck. One patient had the bladder neck injury extending into the right ureteric orifice. Primary urethro-vesical anastomosis was done over Foley’s catheter with 4-0 Polyglactin sutures in interrupted fashion. Ureteric reimplantation was done in one patient who had injury involving the ureteric orifice. A12 Fr SPC insertions were done in all patients. Intraabdominal drain was kept.
Voiding trial was given at 4 weeks. Postoperatively, all patients were continent and were voiding with good urine flow at mean follow up of four years. None of the patients developed stricture at anastomotic site or required any auxillary procedure.
Discussion
Incidence of posterior urethral injuries in children is rare (0.47-4.2%) [2] and it is commonly seen secondary to road traffic accidents. The posterior urethral injury is rare in paediatric age group because paediatric pelvis has greater elasticity of sacroilliac joint and symphysis pubis and greater plasticity of bone, hence greater force of energy is required for pelvic fracture [2]. The risk of complete bladder neck distraction injury is more common in children than in adults. The proposed mechanism behind this could be due to the intra-abdominal location of the bladder which is mobile and smaller, cranially placed prostate which is fixed, which predisposes bladder neck disruption in children.
In all these patients immediate primary urethro-vesical anastomosis was done due to suspicion of bladder injury with extravasation on CECT [Table/Fig-3,4]. There are two schools of thought for the optimal management of paediatric bladder neck distraction injury: immediate repair and delayed repair. Proponents of early repair cite benefits of less dense stricture formation, decreased chance of genitourinary fistulae. Also, in presence of rectal or vaginal injuries, immediate repair is needed to prevent the infectious complications. While proponents of delayed repair cite increased blood loss, poor demarcation of the devitalized tissue planes, increased morbidity due to associated soft tissue or skeletal injuries and advocate suprapubic tube placement and delayed repair when the patient’s general condition improves [3].
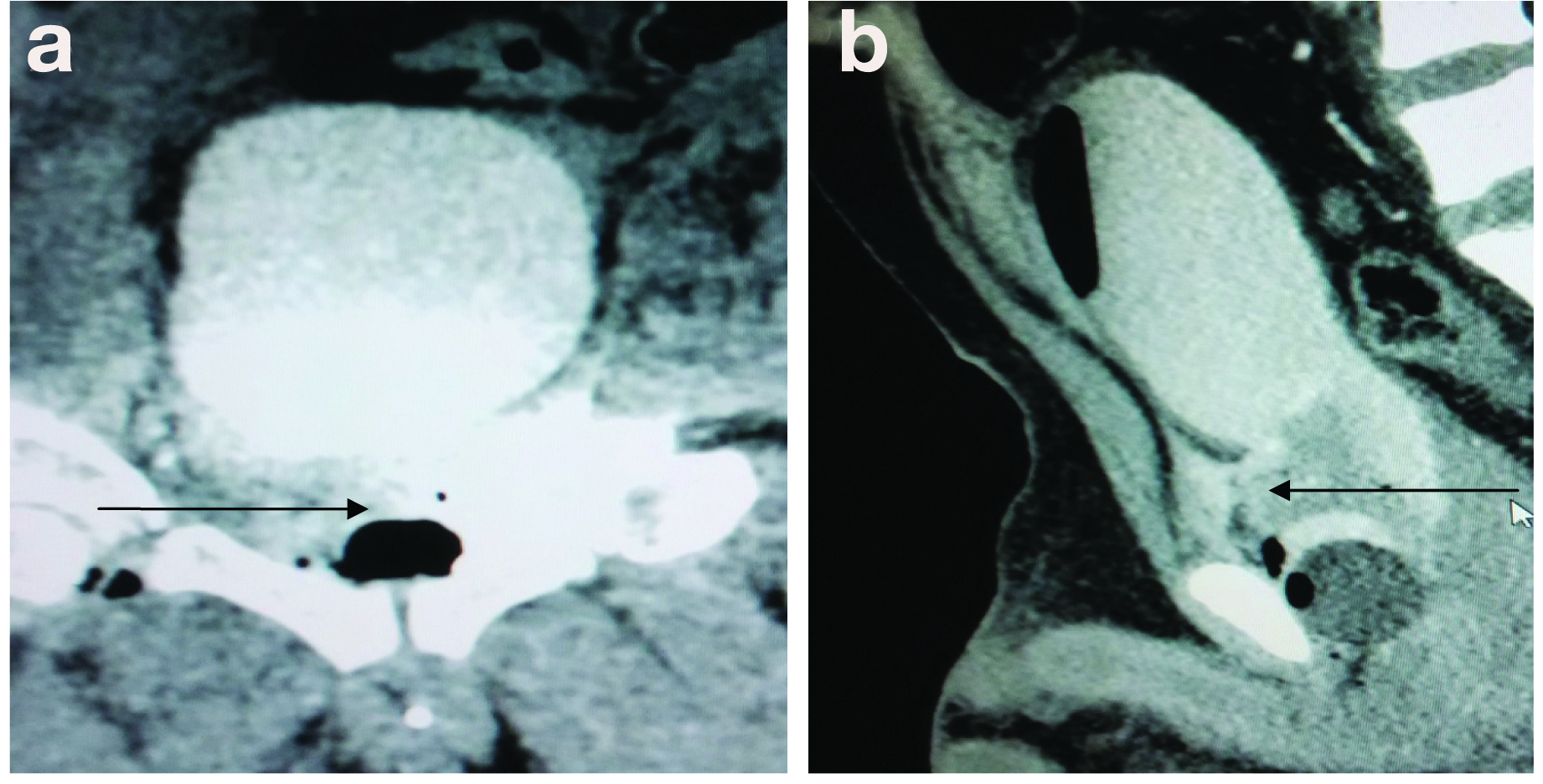
CT scan images of patient-2 showing contrast extravasation at bladder neck: a) Coronal view; b) Sagittal view.
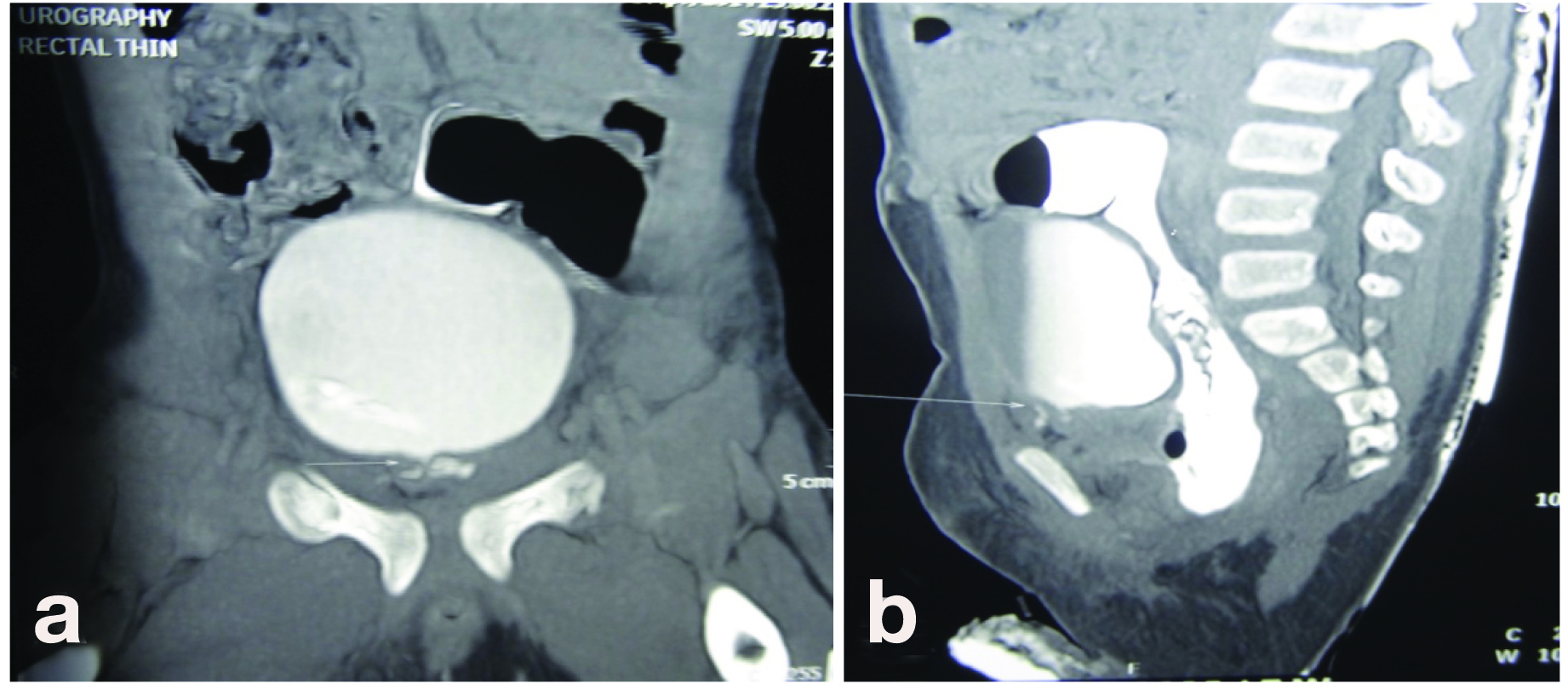
CT scan images of patient-3 showing contrast extravasation at bladder neck: a) Coronal view; b) Sagittal view.
Routh JC and Husmann DA have noted that immediate repair of the bladder neck injury decreases the incidence of acute complications like urinary extravasation which can lead to pelvic urinoma, abscess, osteomyelitis or necrotizing fasciitis, although, they have noted a higher incontinence rate of upto 75% [4]. Balkan E et al., found a lower stricture rate of 16.6% in paediatric patients with posterior urethral injury undergoing early repair versus a stricture rate of 37.5% in patients who underwent delayed repair [5]. Similar to these two studies we have found a low complication rate in paediatric bladder neck distraction injury patients treated with immediate repair. There can be associated ureteric injury, hence abdominal approach is preferred. Voelzke BB et al., have advocated immediate repair for the bladder neck injury to prevent the associated complications by placement of a urethral catheter across the injury site with tacking urethral sutures for tissue approximation in addition to suprapubic tube placement in the acute setting [6]. Even in case of adult bladder neck injuries, Mundy AR supports early repair for better outcome and to reduce morbidity associated with the delayed repair [7]. In our experience with bladder neck distraction injury in paediatric patients, immediate primary repair is easier than the delayed repair because during delayed repair, severe fibrosis with resultant dense stricture limits the optimal reconstruction in the small calibre paediatric urethra.
Conclusion
Considering the rare occurrence of paediatric bladder neck distraction injury and paucity of literature of similar cases, we suggest that immediate urethro-vesical anastomosis can give good long term results in cases of paediatric bladder neck distraction injury.
[1]. Goldman SM, Sandler CM, Corriere JN, McGuire EJ, Blunt urethral trauma: A unified, anatomical mechanical classificationJ Urol 1997 157:85-89. [Google Scholar]
[2]. McAninch JW, Voelzke B, Managing urethral trauma in childrenEuropean Urological Review 2008 :118-121. [Google Scholar]
[3]. Philipraj SJ, Delayed repair is the ideal management for posterior urethral injuries- FOR the motionIndian Journal of Urology 2010 26(2):305-09. [Google Scholar]
[4]. Routh JC, Husmann DA, Long term continence outcomes after immediate repair of pediatric bladder neck lacerations extending into the urethraJ Urol 2007 178:1816-18. [Google Scholar]
[5]. Balkan E, Kilic N, Dogruyol H, The effectiveness of early primary realignment in children with posterior urethral injuryInt J Urol 2005 12(1):62-66. [Google Scholar]
[6]. Voelzke BB, Breyer BN, McAninch JW, Blunt pediatric anterior and posterior urethral trauma: 32-year experience and outcomesJ Pediatr Urol 2012 8(3):258-63. [Google Scholar]
[7]. Mundy AR, Andrich DE, Pelvic fracture-related injuries of the bladder neck and prostate: Their nature, cause and managementBJU Int 2010 105:1302e8 [Google Scholar]