Treatment of Skeletal Class III Malocclusion by Surgery First Orthodontic Approach
MSV Kishore Kumar1, N Viveka Vardhan Reddy2, B Sandeep3, Varalakshmi Chandaveni4, Vishal Guntuk5
1 Professor and Head, Department of Orthodontics and Dentofacial Orthopedics, SVS Institute of Dental Sciences, Mahabubnagar, Telangana, India.
2 Professor, Department of Oral and Maxillofacial Surgery, SVS Institute of Dental Sciences, Mahabubnagar, Telangana, India.
3 Senior Lecturer, Department of Orthodontics, SVS Institute of Dental Sciences, Mahabubnagar, Telangana, India.
4 Postgraduate Student, Department of Orthodontics, SVS Institute of Dental Sciences, Mahabubnagar, Telangana, India.
5 Postgraduate Student, Department of Orthodontics, SVS Institute of Dental Sciences, Mahabubnagar, Telangana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Varalakshmi Chandaveni, Postgraduate Student, Department of Orthodontics, SVS Institute of Dental Sciences, Mahabubnagar-509002, Telangana, India.
E-mail: varalakshmichandaveni@gmail.com
Bilateral sagittal split osteotomy, Genioplasty, Region acceleration phenomenon
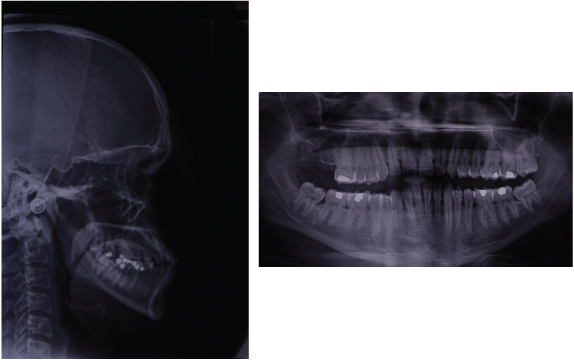
A 26-year-old male patient reported to the Department of Orthodontics, SVS Institute of Dental Sciences, Mahabubnagar, Telangana, India, with a chief complaint of unaesthetic appearance due to forward placement of lower jaw. Extraoral examination revealed mesoprosopic facial form with concave profile, mild incompetent lips, flat smile arc, prominent chin with normodivergent growth pattern and anterior divergence. Intraoral examination revealed Angle’s Class III molar and canine relation bilaterally, spacing in the lower anterior region, anterior cross bite, missing tooth #17 and reverse overjet of 2 mm. Cephalometric analysis revealed Class III skeletal jaw bases (ANB of-2°), Cephalometrics for Orthognathic Surgery (COGS) showing mandibular prognathism (Go-Pg =79 mm) (N-B=13 mm) (N-Pog =16 mm), concave profile (N-A-Pog=-3°), normodivergent growth pattern with mandibular plane angle of 23°, upper anteriors proclined (U1=127°) and lower anteriors retroclined (IMPA=84°) [Table/Fig-1,Table/Fig-2].
Diagnosis and Treatment Planning
Patient was diagnosed as skeletal Class III with normodivergent growth pattern and dental Angle’s Class III malocclusion with proclined upper anteriors and retroclined lower anteriors. Treatment objectives were to correct the skeletal Class III to obtain Class I molar and canine relation, to achieve an ideal overjet, overbite and aesthetic profile. Patient was explained about treatment options: 1) non surgical approach i.e., camouflage by extraction of upper second premolars and lower first premolars; 2) surgical approach: a) conventional surgical approach which includes orthodontic decompensation, surgery, postsurgical orthodontics; b) surgery first approach which includes surgery followed by postsurgical orthodontics. Patient’s choice was Surgery First Orthodontic Approach (SFOA), it was decided to treat in three phases.
Phase I: Bilateral sagittal split osteotomy to setback the mandibular segment by 7 mm and advancement genioplasty by 4 mm.
Phase II: Postsurgical levelling and alignment of upper and lower arches followed by finishing and detailing.
Phase III: Prosthetic implant replacement of tooth #17.
Pretreatment photographs.

Treatment Progress
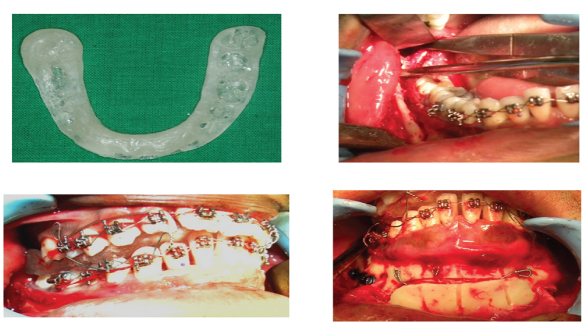
As it was SFOA, surgery was performed first followed by orthodontics, starting with articulation of models and then mock surgery was performed with mandibular setback of 7 mm and splint fabricated with Class I molar and canine relation bilaterally, later bonding was done one day before surgery using preadjusted edgewise appliance with MBT 0.022″x0.028″ slot in upper and lower arches followed by ligature wire consolidation. Under general anaesthesia surgical procedure was performed by bilateral sagittal split osteotomy (mandibular setback 7 mm) and advancement genioplasty of 4 mm. A rigid fixation was done with miniplates, screws and intermaxillary fixation with ligature wires for two weeks. Postoperatively Class I molar and canine relation was achieved with slight lower midline deviation by 1 mm to left side.
Pretreatment radiographs.
Post-treatment photographs.

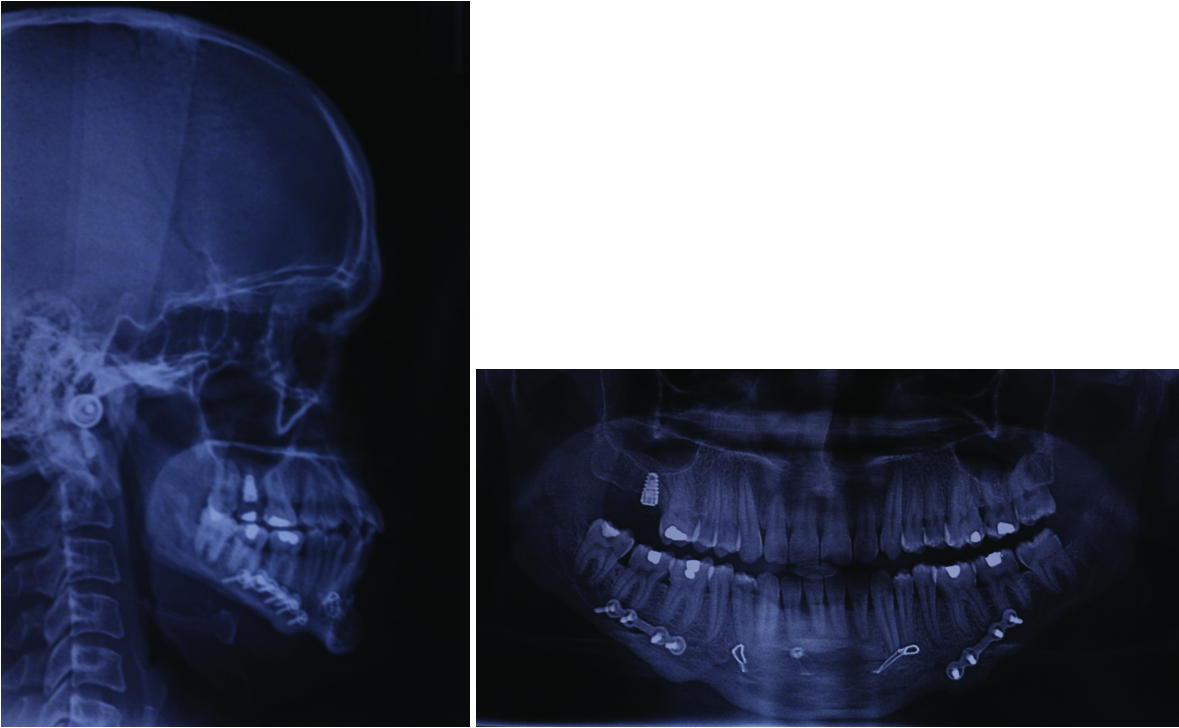
Post-treatment radiographs.
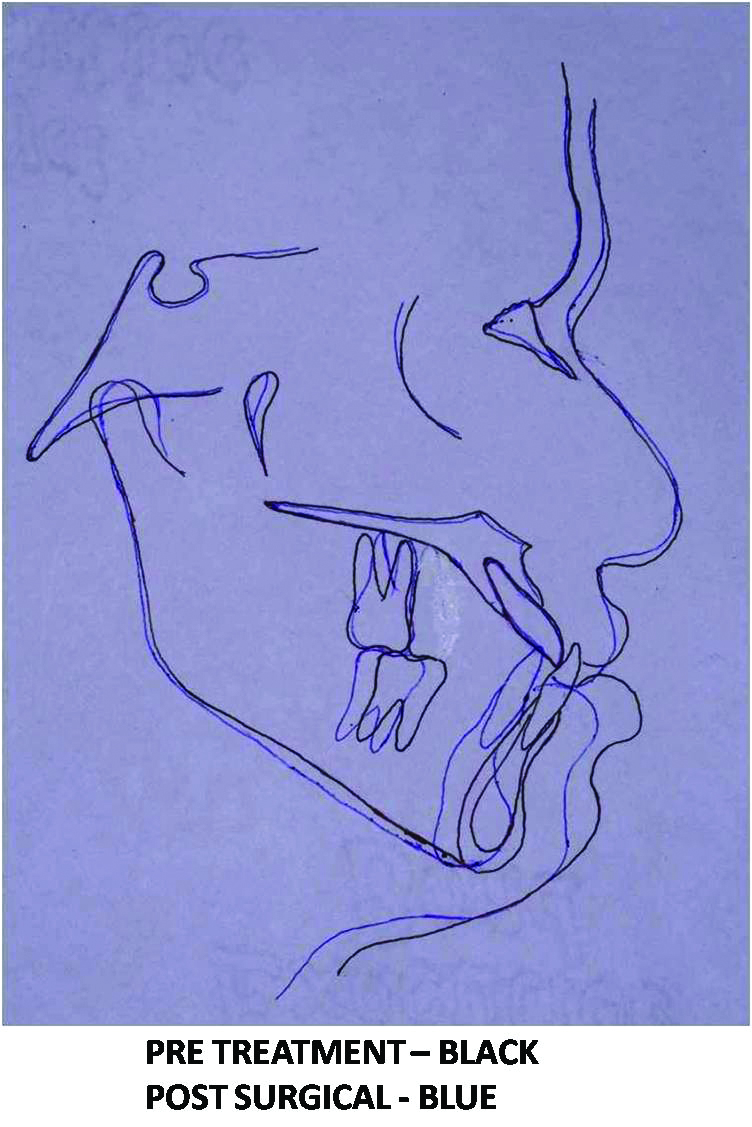
Superimposition tracing.
Black line represents pretreatment, blue line represents post-treatment
After two weeks, phase II treatment was started initially by levelling and alignment of upper and lower arch followed by post surgical finishing and detailing. After debonding maxillary and mandibular Hawley’s retainers were given for retention purpose as there were spacings before treatment. Total treatment duration was 15 months. Finally, patient was referred to department of prosthodontics for replacement of missing tooth #17 with dental implant [Table/Fig-4,Table/Fig-5].
Comparison of cephalometric values had shown acceptable orthognathic facial profile, reduction of mandibular prognathism, increased Frankfort horizontal Mandibular plane Angle (FMA) which cause increase in lower facial height, normal mandibular length, increased gonial angle and improved facial proportions, SNB angle within normal limits with improved Witt’s appraisal. There was a good improvement in the profile of the patient, lower lip protrusion was reduced. Ideal overjet and overbite and Class I molar and canine relation were achieved [Table/Fig-6Table/Fig-7].
Cephalometric comparision.
| Cephalometric Parameters | Normal | Pretreatment | Post-treatment |
|---|
| SNA | 82° | 90° | 91° |
| SNB | 80° | 92° | 89° |
| ANB | 2° | -2° | 2° |
| FMA | 25° | 23° | 26° |
| U1-SN | 102° | 127° | 123° |
| L1-MP | 90° | 84° | 81° |
| L1-FH | 65° | 73° | 67° |
| Nasolabial angle | 102°±8° | 61° | 82° |
Discussion
Class III is a rare malocclusion, it may occur due to prognathism of the mandible, retrognathism of the maxilla, protrusive mandibular dentition, retrusive maxillary dentition or combinations of these [1,2]. For an adult patient with skeletal deformities, orthodontics alone is not sufficient, surgery along with orthodontics is an ideal treatment modality in these type of cases [3]. In the present case there was Class III relation, because of normal maxilla and prognathic mandible, so mandibular setback was the preferred type of surgery. But the length of treatment time is a major concern for the patient, so based on intraoral clinical features we planned surgery first approach by non extraction therapy as there was no major discrepancy in the above case. Thereby addressing, the patient’s chief concern i.e., unaesthetic appearance of face, reduced treatment time.
Surgical procedure was performed by bilateral sagittal split osteotomy (mandibular setback 7 mm) and advancement genioplasty of 4 mm. Bilateral sagittal split osteotomy was performed to provide clockwise rotation of the mandible, chin advancement to enhance dental, skeletal, and soft tissue relationships which were favorable in this case where clockwise rotation of mandible had occurred [4,5].
[1]. Ellis E, McNamara JA, Components of adult Class III malocclusionJournal of Oral and Maxillofacial Surgery 1984 42(5):295-305. [Google Scholar]
[2]. McNamara JA, Brudon WL, Orthodontic and orthopedic treatment in the mixed dentition 1993 Jun 1 Needham Press [Google Scholar]
[3]. Wu J, Jiang JH, Xu L, Liang C, Bai Y, Zou W, A pilot clinical study of Class III surgical patients facilitated by improved accelerated osteogenic orthodontic treatmentsThe Angle Orthodontist 2015 85(4):616-24. [Google Scholar]
[4]. Beukes J, Reyneke JP, Becker PJ, Variations in the anatomical dimensions of the mandibular ramus and the presence of third molars: Its effect on the sagittal split ramus osteotomyInternational Journal of Oral and Maxillofacial Surgery 2013 42(3):303-07. [Google Scholar]
[5]. Furquim BA, de Freitas KM, Janson G, Simoneti LF, de Freitas MR, de Freitas DS, Class III malocclusion surgical-orthodontic treatmentCase Reports in Dentistry 2014 2014(868390):9pages [Google Scholar]