Physiological Root End Closure in a Traumatized Young Permanent Tooth Using Collagen Particles as Pulpal Dressing
V Krishnapriya1, Divya Gaur2, CH Santosh Kumar3, G Shilpa4
1 Head of Department, Department of Paedodontics and Preventive Dentistry, Army College of Dental Sciences, Secunderabad, Telangana, India.
2 Postgraduate Student, Department of Paedodontics and Preventive Dentistry, Army College of Dental Sciences, Secunderabad, Telangana, India.
3 Reader, Department of Paedodontics and Preventive Dentistry, Army College of Dental Sciences, Secunderabad, Telangana, India.
4 Reader, Department of Paedodontics and Preventive Dentistry, Army College of Dental Sciences, Secunderabad, Telangana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Divya Gaur, 154 Gunrock Enclave, Phase 2, Secunderabad-500003, Telangana, India.
E-mail: drdivyagaur@hotmail.com
The management of traumatized young permanent teeth has always been a challenge to the clinician, considering the importance of retaining the vitality of the tooth. Recently, collagen particles have been successfully used as pulpotomy medicaments in primary teeth. This case report shows the use of collagen particles as pulpal dressing in a traumatized young permanent tooth of a nine-year-old child presenting with complicated fracture of young permanent left maxillary central incisor. Partial pulpotomy was performed with collagen particles (Biofil-AB) as pulpal dressing. At six months follow up, apexogenesis was found to be nearly complete. Thus, collagen can be considered as a potential pulpal medicament for apexogenesis procedures.
Anterior tooth trauma, Apexogenesis, Pulpal medicament
Case Report
A nine-year-old boy reported to the Department of Paediatric Dentistry at Army College of Dental Sciences, Secunderabad, Telangana, India, with chief complaint of broken upper front tooth due to a fall from bicycle about one hour before presentation. Clinical examination revealed laceration on upper lip and complicated crown fracture with pulpal exposure on left maxillary central incisor [Table/Fig-1,2]. The tooth was sensitive to percussion but no mobility was observed. Radiographic examination showed immature apex of the fractured tooth [Table/Fig-3]. The child’s medical history was noncontributory. Informed consent was obtained from the child’s parents and ethical clearance was obtained from the institutional ethical committee as we intended to use a novel material for the procedure.
Preoperative clinical presentation.

Palatal view. Site of pulp exposure can be appreciated.

Radiographic examination at the time of presentation. Immature apex is visible in with tooth #21.

Local anaesthesia was administered and the exposed pulpal tissue was irrigated with normal saline. Rubber dam could not be placed because of absence of supporting tooth structure, thus cotton rolls were used for isolation. Partial pulpotomy was done and bleeding was controlled by cotton pellets moistened with normal saline. Once haemostasis was achieved, Biofil-AB (Eucare pharmaceuticals, Chennai, India) [Table/Fig-4] particles were mixed with normal saline as per manufacturer’s instructions and placed in contact with pulpal tissue with filling instrument [Table/Fig-5]. A thick mix of zinc oxide eugenol was placed over it and glass ionomer cement restoration was done. Finally, composite was used as the coronal restoration.


The patient was then monitored clinically and radiographically after 24 hours, one week and then every three months [Table/Fig-6,7], to check continued root development and to check for clinical and radiological signs of irreversible pulpal damage, root resorption or periapical pathology. After six months, radiograph [Table/Fig-8] revealed almost completed root development. A calcific barrier was also observed on the radiograph below Biofil-AB and electric pulp testing revealed that the tooth was vital.
Twenty four hours radiograph.

Three month radiograph. Slight increase in root length is observed.

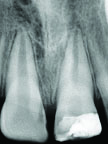
Six month radiograph. Increased root length and approximate apical closure is observed.
Discussion
Management of tooth fractures depends on various factors like severity of fracture, involvement of alveolar bone, concomitant soft tissue injury and availability of fractured fragment, aesthetics and occlusion. In young permanent teeth, the aim is to preserve the vitality of the pulp to promote physiological root lengthening and dentin deposition at the apex.
The goal of apexogenesis as described by Webber RT [1], emphasized on sustaining a viable Hertwig’s root sheath and maintaining pulp vitality to allow dentin deposition at the root apex. He also insisted on inducing the formation of dentinal bridge at pulpotomy site to ensure pulp vitality.
Collagen is a unique biomaterial with exceptional properties including low immune response, low toxicity, ability to promote cellular attachment and growth, among others [2]. Other properties like facilitating wound maturation by enhancing the initial blood clot and fibrin linkage formation, assisting in wound healing by attracting monocytes and other inflammatory cells [3] have also been utilized in medicine and dentistry. Various studies demonstrating favourable properties of collagen have been tabulated in [Table/Fig-9] [3–6]. Kakarla P et al., demonstrated regenerative characteristics of collagen which were similar to the study conducted by Marsan T et al., where collagen bioresorbable membrane, when used as pulp capping material in Mongrel dogs resulted in increased vascularization and pulp healing [4,5].
Various studies with collagen as pulp dressing medicament [3–6].
| Study/Article | Material/ Form of Collagen | Procedure | Result/Outcome |
|---|
| Postlethwaite AE et al., [3] | Human Type I, II, III collagen | Fibroblast chemotaxis assay using blind well modified boyden chemotaxis chambers | Collagen promotes wound healing by acting as chemotactic stimuli for fibroblasts |
| Kakarla P et al., [4] | Biofil-AB | Standard pulpotomy procedure on human primary teeth indicated for orthodontic extraction | Regeneration of pulp tissue on histological evaluation |
| Marsan T et al., [5] | Bio-Gide (collagen bioresorbable membrane) | Direct pulp capping in Mongrel dogs | Histological evaluaiton revealed preservation of morphology of all histological structures and increased number of blood vessels |
| Brett D [6] | Review: Collagen based wound dressings | NA | Collagen dressings act as sacrificial substrate for MMPs in chronic wounds |
In the present case, collagen particles (Biofil-AB; Eucare pharmaceuticals, Chennai, India) with antibiotics were used as pulpal medicament. Biofil-AB are sterile medicated Type I collagen particles that are lyophilized and incorporated with muciprocin 2% w/w and metronidazole 1% w/w [4]. It is non-allergenic, non-immunogenic and non-toxic. Incorporating antibiotics in it, ensures sterile local environment.
According to the studies by Sheehy EC and Roberts GJ [7], 74%-100% of the cases where calcium hydroxide was used, resulted in apical barrier formation and on an average it took five to 20 months for apical barrier formation.
In this case report, the quality of apical barrier cannot be judged radiographically and thus, it is too early to conclude that collagen as a pulp dressing medicament leads to faster root end closure while maintaining the vitality of pulp tissue. It requires further research and stringent clinical trials as well as long term studies.
Conclusion
The healing potential of the pulp of immature teeth, as proven and documented in numerous studies can be utilized for managing traumatic injuries to young permanent teeth. By carrying out further histological research and long term clinical studies with newer pulp dressing materials, we will be able to understand the physiology of pulp better.
[1]. Webber RT, Apexogenesis versus apexificationDent Clin N Am 1984 28:669-97. [Google Scholar]
[2]. Silva L, Leonardo M, Nelson-Filho P, Medeiros A, Rossi M, Pulp response of anionic lyophilized collagen matrix with or without hydroxyapatite after pulpotomy in dog’s teethMat Res 2006 9(2):175-80. [Google Scholar]
[3]. Postlethwaite AE, Seyer JM, Kang AH, Chemotactic attraction of human fibroblasts to type I, II, and III collagens and collagen-derived peptidesProc Natl Acad Sci 1978 75(2):871-75. [Google Scholar]
[4]. Kakarla P, Avula JS, Mellela GM, Bandi S, Anche S, Dental pulp response to collagen and pulpotec cement as pulpotomy agents in primary dentition: A histological studyJ Conserv Dent 2013 16(5):434-38. [Google Scholar]
[5]. Marsan T, Prpic-Mehicic G, Karlovic I, Sostaric B, Anic I, Karlovi Z, Pulpal response to direct pulp capping with collagen bio-resorbable membraneActa Stomat Croat 2003 37:59-62. [Google Scholar]
[6]. Brett D, A review of collagen and collagen-based wound dressingsWounds 2008 20(12):347-56. [Google Scholar]
[7]. Sheehy EC, Roberts GJ, Use of calcium hydroxide for apical barrier formation and healing in non-vital immature permanent teeth: A reviewBr Dent J 1997 183:241-46. [Google Scholar]