Obturation of a Retained Primary Maxillary Second Molar Using BiodentineTM: A Case Report
Ganesh Jeevanandan1
1 Senior Lecturer, Department of Paedodontics and Preventive Dentistry, Saveetha Dental College, Chennai, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ganesh Jeevanandan, 162, Poonamalle High Road, Velappanchavadi, Chennai-600095, Tamil Nadu, India.
E-mail: helloganz@gmail.com
Maxillary molars have highly variable root canal morphology. However, the presence of the two roots is a rare occurrence. The success of pulpectomy treatment depends on removal of infected pulp and filling it with a biocompatible material. In order to achieve it, the clinicians should understand the morphology of the individual root canal and atypical root canal configuration. The purpose of this article was to describe an unusual anatomy in primary maxillary second molar with missing successor tooth. Biodentine™ a new dentine substitute was used as an obturating material for retained maxillary second molar. After 24 months follow up, the success of Biodentine™ for management of primary tooth with missing successor was evaluated and reported.
Dentin substitute, Pulpectomy, Root dysmorphology
Case Report
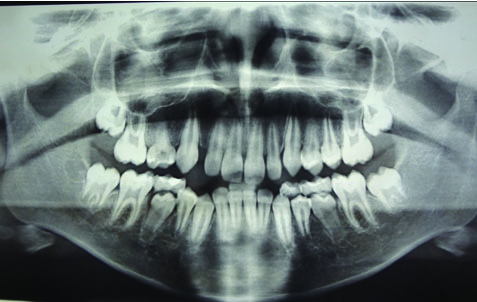
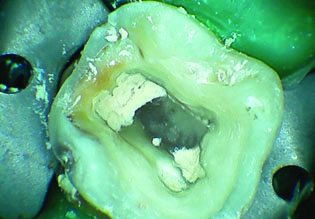
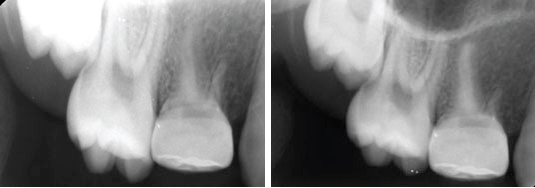
A 12-year-old boy was referred to the Department of Paedodontics and Preventive Dentistry for evaluation and treatment of a carious right primary maxillary second molar [Table/Fig-1]. During clinical examination it was tender on percussion and palpation with no evidence of mobility and sinus tract. The patient had no significant medical history. Intraoral periapical radiograph of right maxillary region revealed radioluency involving pulp with absence of first and second premolars [Table/Fig-2]. A panoramic radiograph was taken to investigate the absence of any other permanent tooth bud [Table/Fig-3]. Based on the clinical and radiographic examination, dental caries with chronic pulpitis in relation to right primary maxillary second molar and congenitally missing premolars was diagnosed. Following parental consent, the tooth was anaesthetized with 2% lignocaine hydrochloride 1:2,00,000 epinephrine (Lignox Indoco Remedies Ltd. Mumbai, India) and isolated using a rubber dam. Access preparation was completed; two canal orifices (mesiobuccal and palatal) were located [Table/Fig-4]. The working length was determined radiographically measuring 13 mm for the palatal canal and 10 mm for the mesiobuccal canal. The root canals were enlarged till 35 K-file (Mani, Inc, Tochigi, Japan). During instrumentation the canals were irrigated using 3% sodium hypochlorite solution and the final irrigation was done with saline. The canals were obturated with Biodentine™ [Table/Fig-5]. Using a measured endodontic plugger the material was vertically condensed from the apex to the canal orifice in both palatal and mesiobucal canals [Table/Fig-6]. The coronal seal of the endodontically treated tooth was done with glass ionomer cement (GC Fuji II, Tokyo, Japan). Finally size five stainless steel crown (3M ESPE, St Paul, MN, USA) was cemented using Type 1 glass ionomer cement [Table/Fig-7]. At six and 24 months follow up [Table/Fig-8,9] the tooth revealed no periapical lesion and no evidence of mobility.
Clinical picture showing caries in primary second molar.

Radiograph showing radiolucency involving pulp in primary second molar with missing I successor.

Orthopantomogram showing radiolucency involving pulp in primary second molar with missing successors.
Intraoral picture showing mesio buccal and palatal canal orifice.

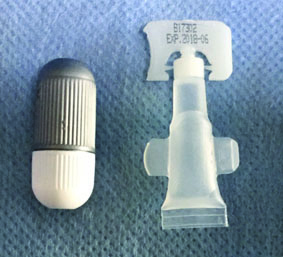
BiodentineTM-powder in capsule and liquid in a pipette.
Intraoral picture showing obturation of mesio buccal and palatal canal with BiodentineTM.
Postoperative radiograph showing obturation of primary maxillary second molar with BiodentineTM.

Follow up radiograph after six and 24 months. (Images left to right)
Discussion
Maintenance of the retained primary tooth with congenital absence of permanent successor is a challenge to the dentist. On literature search, the anomaly of double rooted maxillary second molar in primary dentition has not been documented. This case report describes a retained primary maxillary second molar with two roots and missing premolars. The primary maxillary molars in general have two buccal and one palatal canal, analogous to three distinct roots. Anomalies in root formation occur due to failure in invagination of Hertwig’s Epithelial Root Sheath (HERS). The root sheath grows downward and covers the entire dental papilla during normal development of root. The number of tongue like projection growing inward towards the center from lateral side of root sheath corresponds to the number of roots. Failure of the lateral tongue like projection to form completely, results in dysmorphological root formation like double root molars [1].
Agenesis of one or more teeth is most common anomaly of dental development [2]. The aetiology of dental agenesis is yet to be fully explained. Kurisu K et al., has suggested that tooth agenesis is typically transmitted as an autosomal dominant trait with incomplete penetrance and variable expressivity [3]. Environmental factors (trauma, infection, irradiation and endocrine disorders) are associated with developmental absence of teeth. Ectodermal dysplasia is one of the most common syndrome related with congenital missing of teeth and anodontia [4].
Retained primary teeth having intact crown and root structure with missing successor should be preserved. This would prevent arch length discrepancy and maintain the space without requirement for orthodontic or prosthetic treatment [5]. Obturating material used for filling the root canal space of primary teeth should resorb at a similar rate as the primary root [6]. Various root canal filling materials are available for primary teeth namely, Zinc Oxide Eugenol (ZOE) paste, calcium hydroxide alone or a combination of calcium hydroxide and iodoform paste [7]. ZOE was used as a common material for obturating primary teeth. Accidental extrusion beyond the apex of ZOE remains in the alveolar bone for months to years. The extruded material may also cause a foreign body reaction [8]. Due to this limitation calcium hydroxide based obturating materials were introduced. Calcium hydroxide with iodoform is widely used for obturation of primary teeth due to its better properties compared to ZOE [9]. Primary tooth without permanent tooth bud shows no signs of root resorption. Obturating material for retained primary teeth with missing permanent teeth should be biocompatible and non resorbable [6]. Guttapercha, Mineral Trioxide Aggregate (MTA) and Biodentine™ should be considered as a root canal filling material for retained primary teeth with missing successor. These materials are considered to be biocompatible and non resorbabale. O’ Sulliavan SM et al., reported a case of 20-year-old male with retained primary mandibular second molar, obturated with MTA [10]. Bolla N et al., reported a case of 26-year-old female with retained primary mandibular second molar, obturated with guttapercha [11]. In this case Biodentine™ a recently introduced material was used as a root canal filling material for retained primary maxillary second molar. Biodentine™ is considered to be an alternative to conventional calcium hydroxide based material. It is bioactive cement having similar mechanical properties like dentin. The material is available as liquid and powder component. The powder in the capsule contains tricalcium, dicalicum silicate and calcium carbonate. Zirconium dioxide acts as a contrast medium. The liquid component contains an aqueous solution of calcium chloride with an admix of polycarboxylate. The liquid is added to the powder in the capsule and mixed using amalgamator for 30 seconds. The consistency of the material once mixed is similar to zinc phosphate cement. On follow up, the retained primary second molar was normal in function with no associated pain and periapical changes. Biodentine™ has shown to be a biocompatible material having superior sealing properties [12].
Long term follow up of such cases are required to assess the use of new materials in challenging clinical situation. In dentition having retained primary teeth with missing successor Biodentine™, can be considered as the material of choice for root canal filling. Documentation of such developmental abnormalities with its modified clinical management will aid the clinicians for successful endodontic treatment.
Conclusion
We conclude that this case report presents an unusual case of a primary maxillary second molar with double roots with missing permanent first and second premolars. This paper also adds on the use of a new dentin substitute BiodentineTM as a permanent obturating material for such cases with two years follow up.
[1]. TenCate’s AR, Oral histologyDevelopment, Structure, and Function 1994 4th edSt. LouisMosby:104-07. [Google Scholar]
[2]. Shapiro SD, Farrington FH, A potpourri of syndromes with anomalies of dentitionBirth Defects Orig Artic Ser 1983 19:129-40. [Google Scholar]
[3]. Kurisu K, Tabata MJ, Human genes for dental anomaliesOral Dis 1997 3:223-28. [Google Scholar]
[4]. Lexner MO, Bardow A, Hertz JM, Nielsen LA, Kreiborg S, Anomalies of tooth formation in hypo-hidrotic ectodermal dysplasiaInt J Paediatr Dent 2007 17:10-18. [Google Scholar]
[5]. Kokich VG, Kokich VO, Congenitally missing mandibular second premolars. Clinical optionsAm J Orthod Dentofacial Orthop 2006 130:437-44. [Google Scholar]
[6]. Kubota K, Golden BE, Penugonda B, Root canal filling materials for primary teeth: A review of the literatureJournal of Dentistry for Children 1992 58:225-27. [Google Scholar]
[7]. Pinkham JR, Pediatric dentistry: Infancy Through Adolescence 1999 3rd edPhiladelphiaW.B. Saunders:350 [Google Scholar]
[8]. Mortazani M, Mesbahi M, Comparision of zinc oxide and eugenol and vitapex for root canal treatment of necrotic primary teethInt J of Paed Dent 2004 4:417-24. [Google Scholar]
[9]. Nurko C, Ranly DM, Garcia-Godoy F, Lakshanya KN, Resorption of a calcium hydroxide, iodoform paste (vitapex) in root canal therapy for primary teeth: A case reportPediatr Dent 2000 22:517-19. [Google Scholar]
[10]. O’Sullivan SM, Haretwell GR, Obturation of a retained primary mandibular second molar using mineral trioxide aggregate: A case reportJ Endod 2001 27:703-05. [Google Scholar]
[11]. Bolla N, Naik BD, Kavuri SR, Velagala LD, Obturation of a retained primary mandibular second molar with missing successor using guttapercha: A case reportJIDA 2011 5:194-95. [Google Scholar]
[12]. Wang X, Sun H, Chang J, Characterization of Ca3SiO5/CaCl2 composite cement for dental applicationDent Material 2008 24:74-82. [Google Scholar]