Morphometry of Proximal Femur in Indian Population
Minakshi Verma1, Sheetal Joshi2, Anita Tuli3, Shashi Raheja4, Priyanka Jain5, Priyanka Srivastava6
1 Assistant Professor, Department of Anatomy, Lady Hardinge Medical College, New Delhi, India.
2 Assistant Professor, Department of Anatomy, Lady Hardinge Medical College, New Delhi, India.
3 Director Professor, Department of Anatomy, Lady Hardinge Medical College, New Delhi, India.
4 Director Professor, Department of Anatomy, Lady Hardinge Medical College, New Delhi, India.
5 Statistician, Department of Statistics, ILBS, New Delhi, India.
6 Assistant Professor, Department of Physiology, PGIMER and RML Hospital, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Minakshi Verma, Flat No. 2010, D2, Vasant Kunj, New Delhi-70, India.
E-mail: minakshi.malhotra77@gmail.com
Introduction
Total hip arthroplasty is a commonly performed surgery now-a-day. There are regional and racial variations in the stature of the population worldwide. So there is always need of population specific data for making best fit prosthesis.
Aim
The present study was done to measure the parameters of proximal femur and to analyse their correlation by using standard statistical analysis.
Materials and Methods
Ninety one dry bones (44 left and 47 right) were used. Femur Head Diameter (FHD), Femur Neck Length (FNL), Femur Neck Diameter (FND), Femur Neck Thickness (FNT), Cervicodiaphyseal Angle (CDA) was directly measured with the help of anthropometric instruments. Femur Head Offset (FHO) and Vertical Offset (VO) were measured in the anteroposterior digital photographs.
Results
Normally distributed variables were compared using Student’s t-test (Unpaired data) to analyse significant effect. There was a significant difference between right and left side of FND and CDA. Pearson correlation coefficient was used to analyse the relationship among variables. FHO had high correlation with the VO (0.687, p<0.001).
Conclusion
These parameters can be used for designing the prosthesis and plates for hip joint reconstructive surgeries suitable for Indian population.
Femur head offset, Hip prosthesis, Vertical offset
Introduction
Prevalence of hip osteoarthritis, fracture neck femur and other hip joint ailments are increasing day by day. Arthroplasty is the definite treatment for these patients. The femur forms the skeleton of the thigh, carries body weight, supports the movements of leg and provides attachment to the muscles [1]. Morphology of bones is very much affected by race, sex, environmental factors and life style. A population based study by Nurzenski et al., showed that life style factors also influence geometric indices of bone strength in the proximal femur [2]. FHO and VO are significant tools for range of motion and abductor muscle strength after total hip arthroplasty [3]. Commercially available hip prostheses are made based on European data [4,5]. So the undersize and oversize hip prosthesis in THA (Total Hip Arthroplasty) can affect these functions. Goal of the surgical intervention is mostly to achieve anatomical reduction with a stable fracture fixation which helps bone reunion and allows early mobilization. A better contour fit bone and plate is crucial to establish a stronger bone plate construction [6]. Morphometric study of the proximal femur was performed in different population and communities [7]. Data obtained from these studies demonstrated that femoral morphometry had regional features and social differences. A statistically significant difference was observed in measurements taken with calliper than values obtained with the measurement using the software [8]. In our study we obtained data from direct measurement of dry bones and linear data with digital photographs of the same bones. Unnanuntana A in 2009 used digital photographs to compare 200 cadaveric femora and stated that, accuracy is improved over radiographs and direct measurement because of the ease of positioning and reproducibility of consistent landmark identification [9].
Aim
To compare the right side parameters with the left side parameters of proximal femur and to analyse the relationship among variables of proximal femur.
Materials and Methods
For the prospective morphometric study, 91 dry femurs from human Indian cadavers of both sexes were used in the Department of Anatomy of Lady Hardinge Medical College, New Delhi from January 2015 to January 2016. Out of 91 dry femurs, 47 were of right side and 44 were of left side.
Sample size selection was done with reference to the research paper by Mourao AL et al., on the geometry of the proximal femur in Brazilians [10]. (N=91, α=5%, power 80%).
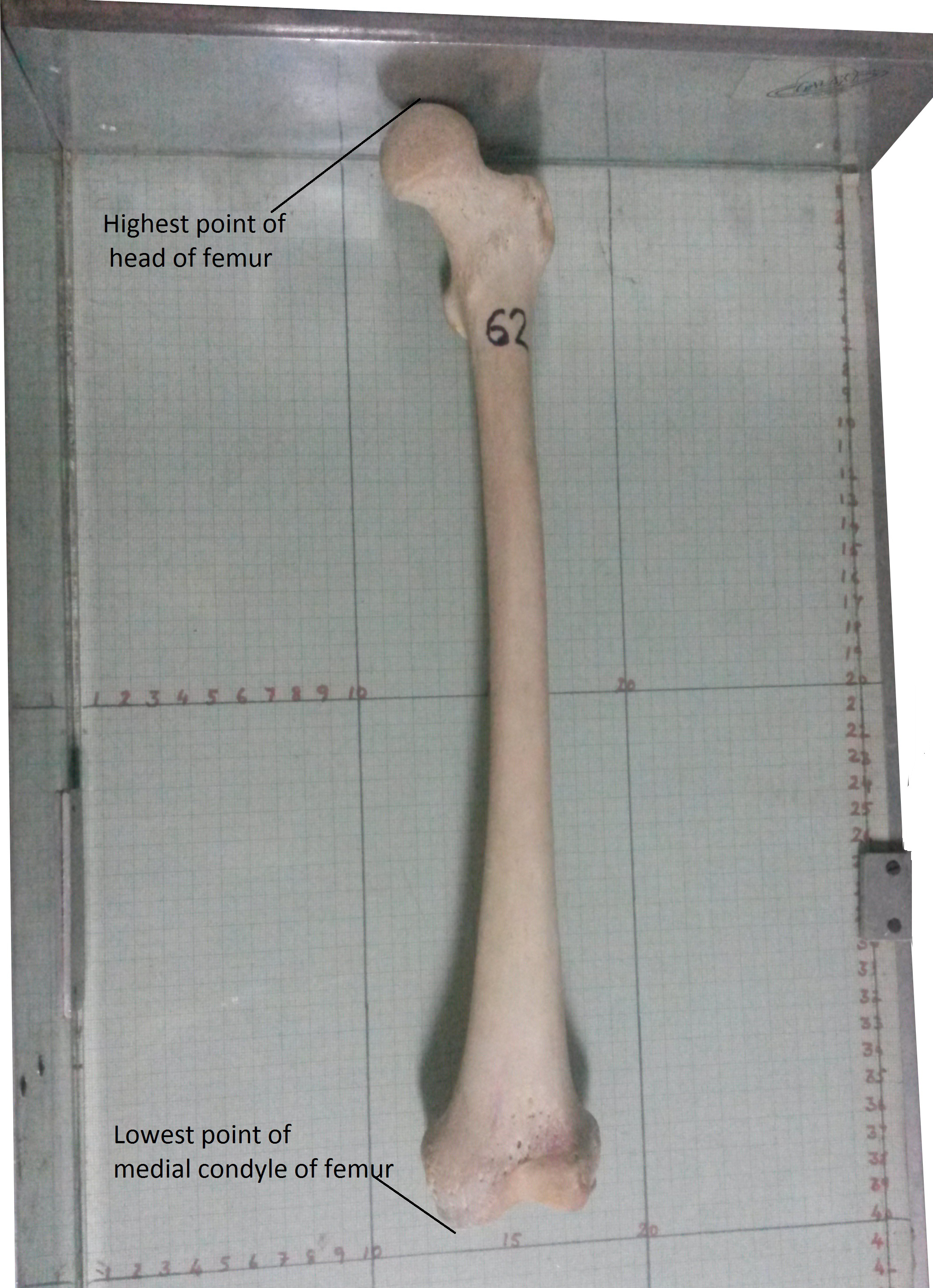
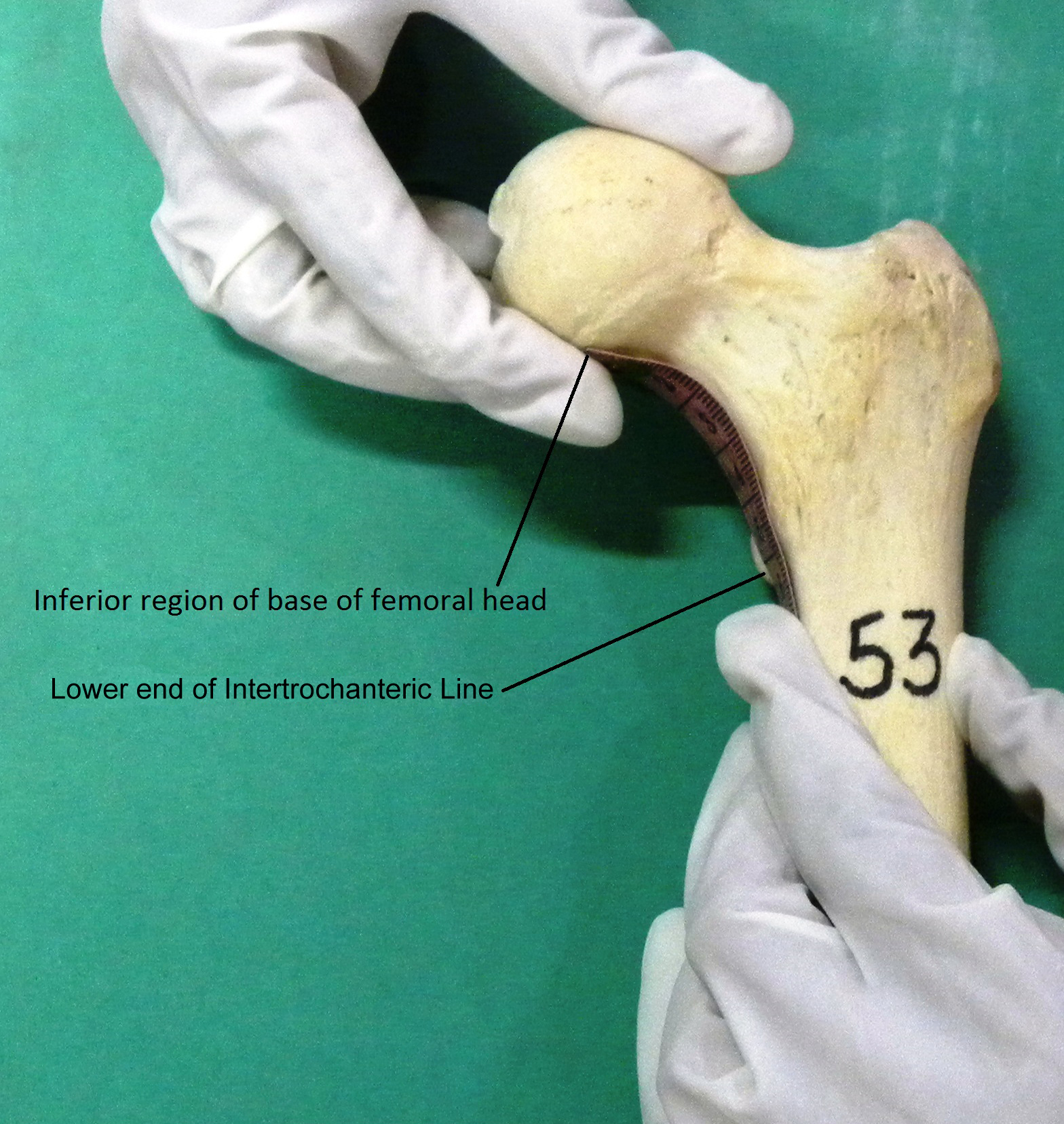
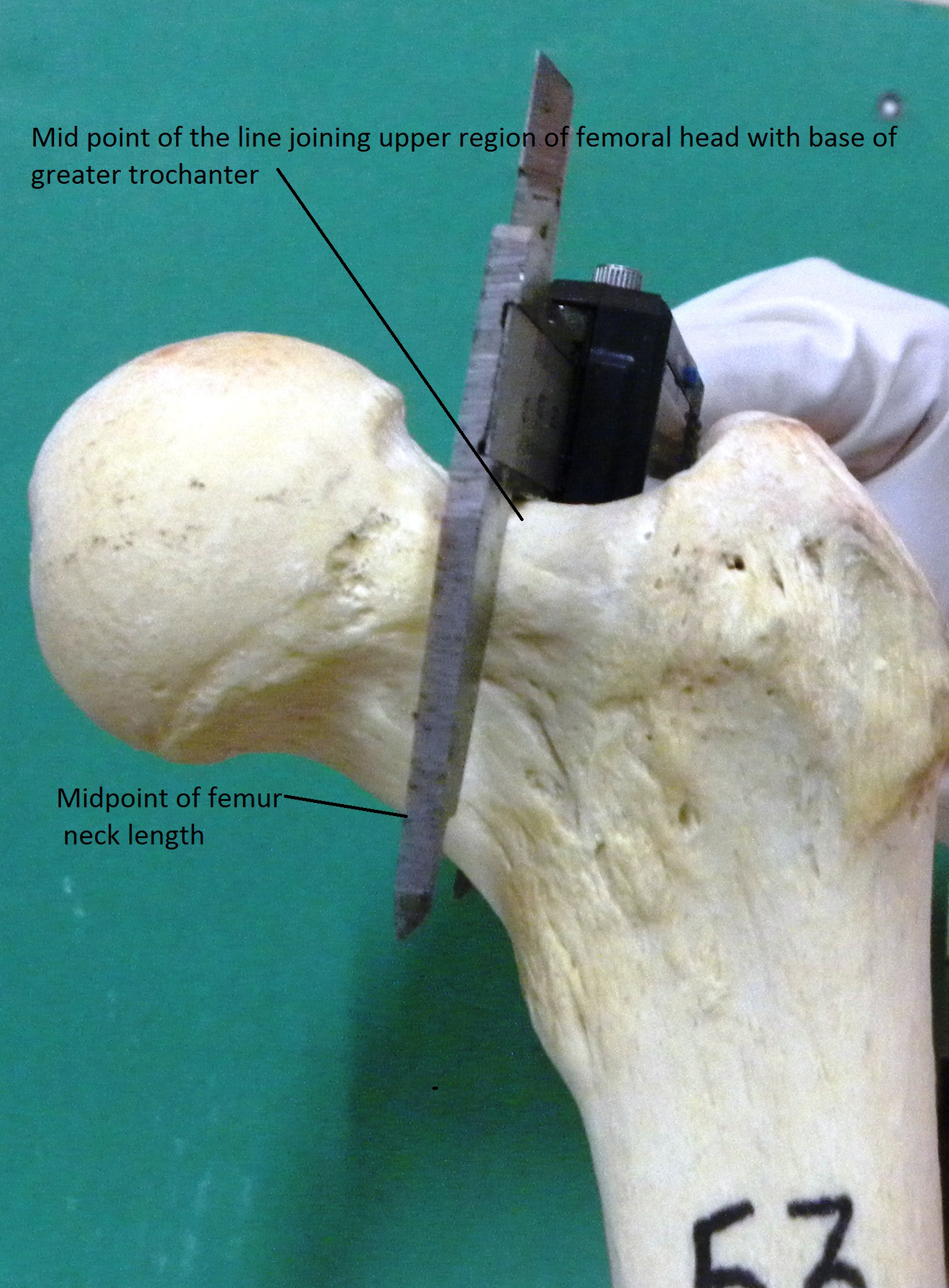
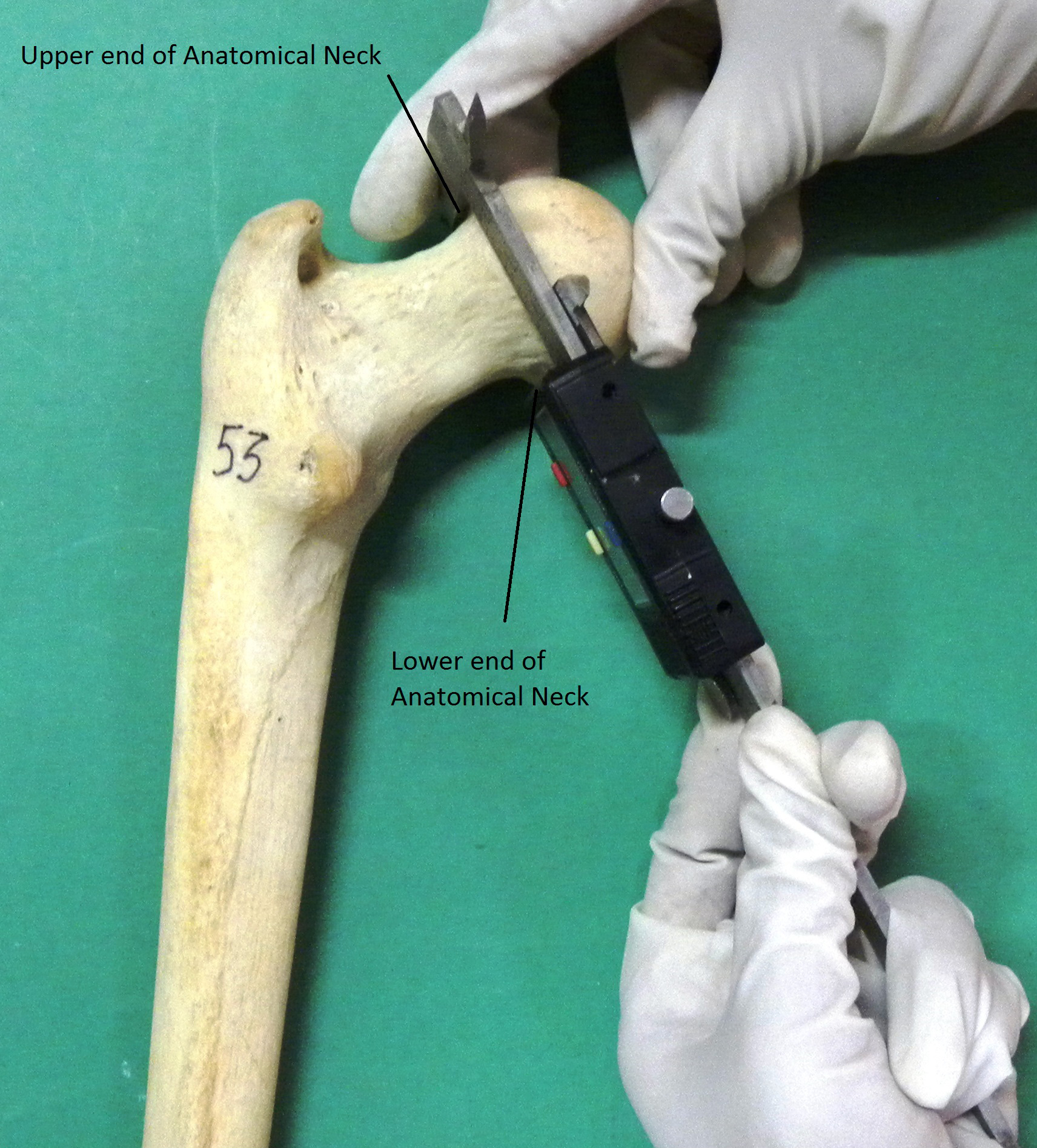
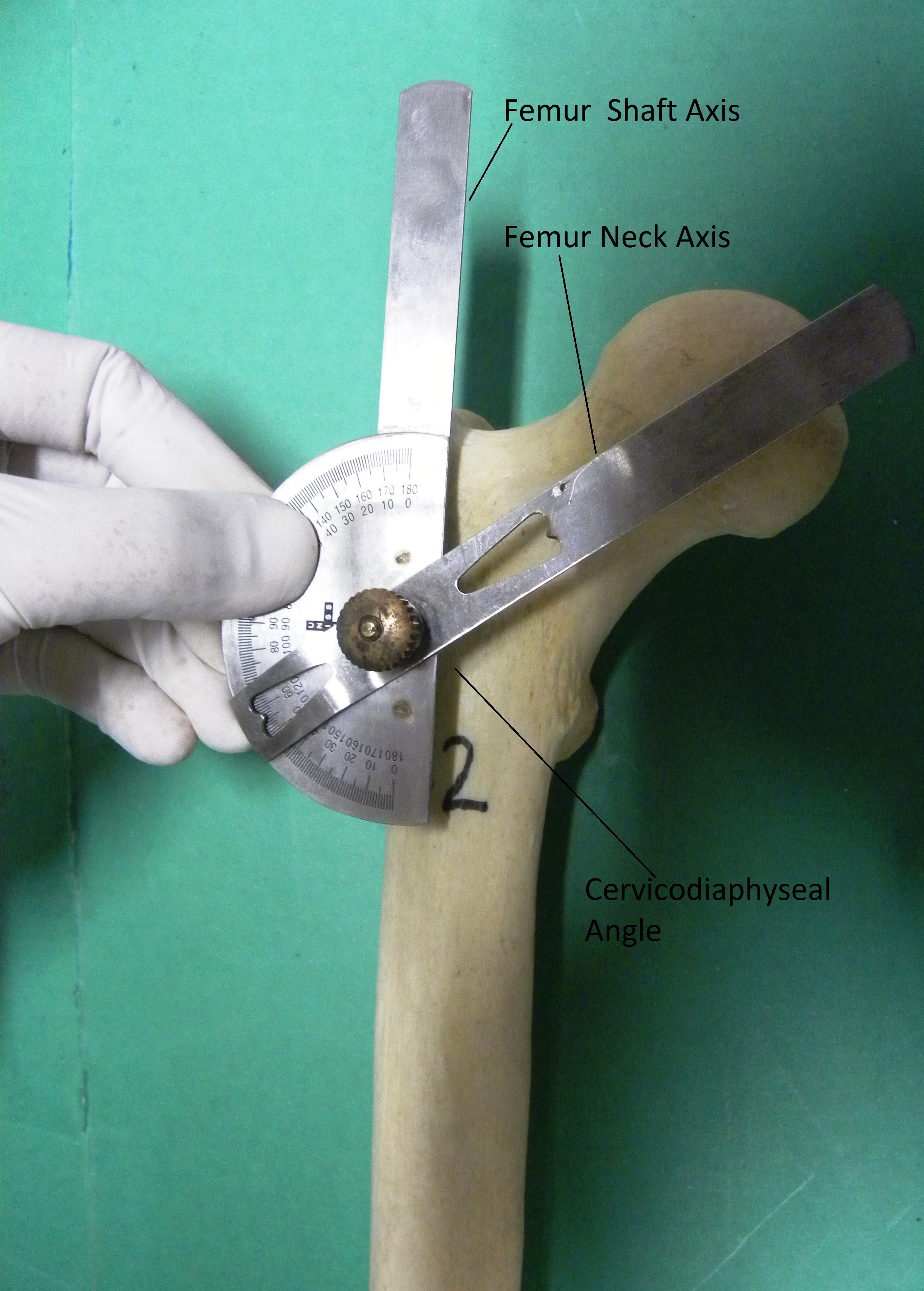
We excluded the bones with visible osseous pathologies like tumours, deformities, fractures, trauma. These are the ailments which could affect the result of study. The study was divided in two steps. In first step we measured femur manually by using Anthropometric instruments like osteometric board, goniometer and digital calliper. Parameters measured were Femur Length (FL) for which femur was placed in a position parallel to the surface of Osteometric board by rotating the femur shaft internally then the distance between the highest point of the femur head to the lowest point of the medial condyle was measured as the femur length [Table/Fig-1]. FHD was the distance in a straight line between the upper end to the lower end of the femoral head in cranio caudal axis [Table/Fig-2]. FNL was the distance between the inferior region of base of femoral head and the lower end of intertrochanteric line [Table/Fig-3]. FNT was thickness of neck of femur in antero posterior axis [Table/Fig-4]. FND was the distance in a straight line from upper end to the lower end of the anatomical neck of femur in craniocaudal direction [Table/Fig-5], and Cervico Diaphyseal Angle (CDA) was the angle between the line joining the center of head of femur and the midpoint of Intertrochantric line (Femur Neck Axis) and vertical line from the tip of greater trochanter (Femur Shaft Axis) [Table/Fig-6].
Length of femur in craniocaudal axis with osteometric board.
Diameter of femoral head in the craniocaudal axis.

Length of femoral neck in craniocaudal axis.
Femur neck thickness in anteroposterior axis.
Femur neck diameter in craniocaudal axis.
Cervicodiaphyseal angle with goniometer.
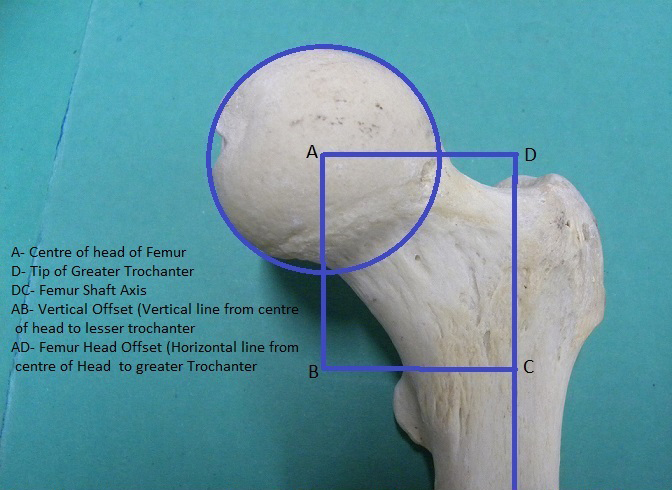
In second step all these bones were photographed anteroposteriorly by digital camera. Femur was placed in a position parallel to the surface of a table by rotating the femoral shaft internally. At a distance of 50 cm superior from the surface of the femur photographs were taken to obtain the anteroposterior pictures. Then the photographs were transferred to the microcomputer for processing with the help of Image J Software. The scanned images were measured after converting from pixels to cm (78 pixels on the scale corresponded to 1 cm.) Three anatomical points were marked. The center of the femoral head, the lesser trochanter and the tip of greater trochanter. The center of head of femur was obtained using Image J Software by drawing a circle around the femoral head, its center was plotted. Linear measurements, the FHO was the horizontal distance among the center of femoral head to the axis of femoral shaft and the VO was the vertical distance between proximal extent of lesser trochanter to the center of femoral head [Table/Fig-7]. All measurements were performed twice by a single person and then arithmetic average was taken. The data were tabulated into a computer.
An anteroposterior photograph demonstrating linear measurements of proximal femur.
Aim of the study was to provide the morphometric data of proximal femur for Indian population and to analyse the relation among the parameters of proximal femur, hence groups were not formed as the male and female. Literature has various studies that were done on dry femur without differentiating the sex [4,8,11].
Statistical Analysis
Statistical analysis comparing morphological features between right and left femur were performed using unpaired t-test. Correlation coefficient was also calculated to analyse the relationship among variables of proximal femur.
All results and observations obtained were thoroughly analysed as per standard statistical methods. Data was reported as proportions or mean±SD. Normally distributed continuous variables were compared using the student’s t-test (unpaired data) to analyse significant effect. Pearson correlation coefficient was used to analyse the relationship among variables.
Results
There was a significant difference between right and left side of neck diameter and cervicodiaphyseal angle. The average femoral head diameter for the entire sample was 42.32±4.11, average FNL was 44.75±8.09, Average FHO was 42.92±5.52 and average VO was 58.13±7.69 [Table/Fig-8].
Morphometric variables of right and left side femur.
| Parameters | Side | N(Number of bones) | Mean | Standard deviation | Total (91 bones) | p-value |
|---|
| Femur length (FL)cm | left | 44 | 42.70 | 3.016 | 42.82±2.87 | 0.703 |
| right | 47 | 42.94 | 2.769 |
| Head Diameter (FHD) mm | left | 44 | 42.11 | 4.530 | 42.32±4.11 | 0.564 |
| right | 47 | 42.51 | 3.729 |
| Femur neck length (FNL)mm. | left | 44 | 44.66 | 6.982 | 44.75±8.097 | 0.920 |
| right | 47 | 44.83 | 9.094 |
| Femur neck thickness (FNT) mm. | left | 44 | 23.86 | 3.092 | 24.01±3.05 | 0.598 |
| right | 47 | 24.15 | 3.043 |
| Femur neck diameter (FND) mm. | left | 44 | 31.73 | 3.662 | 33.02±4.22 | 0.006 |
| right | 47 | 34.23 | 4.395 |
| Cervicodiaphyseal angle (CDA) | left | 44 | 130.3 | 3.875 | 128.90±4.49 | 0.003 |
| right | 47 | 127.57 | 4.661 |
| Femur head offset (FHO) mm. | left | 44 | 43.07 | 5.243 | 42.92±5.52 | 0.838 |
| right | 47 | 42.79 | 5.759 |
| Vertical offset(VO) mm. | left | 44 | 57.93 | 8.222 | 58.13±7.69 | 0.826 |
| right | 47 | 58.32 | 7.248 |
It can be seen in [Table/Fig-9] that head diameter had high correlation with neck thickness (0.748, p<0.001), neck length (0.704, p<0.001) and neck diameter (0.816, p<0.001). FHD had moderate correlation with VO (0.633, p<0.001) and FHO (0.572, p<0.001). For designing the dual offset stem the FHO, VO and neck length are important. On the right and left side femur there was significant difference in neck diameter and cervicodiaphyseal angle [Table/Fig-8] but these two parameters have low correlation with the FHO (0.381 and 0.245, p<0.001) and with VO (0.469, p<0.001 and 0.212, p<0.044) respectively. FHO had a high correlation with the VO (0.687, p<0.001) [Table/Fig-9].
Correlation in morphometric measurements of proximal femur.
| | FHD | FNL | FNT | FND | CDA | VO | FHO |
|---|
| Femur Head Diameter(FHD)(mm) | Pearson correlationSig.(2- tailed) | 1 | .704<0.001 | .748<0.001 | .816<0.001 | .269.010 | .633<0.001 | .572<0.001 |
| Femur Neck Length(FNL)mm. | Pearson correlationSig. (2-tailed) | .704<0.001 | 1 | .429<0.001 | .623<0.001 | .370<0.00 | .602<0.001 | .514<0.001 |
| Femur Neck Thickness(FNT) mm. | Pearson correlationSig.(2- tailed) | .748<0.001 | .429<0.001 | 1 | .653<0.001 | .189.073 | .316<0.001 | .381<0.001 |
| Femur Neck Diameter(FND) mm. | Pearson correlationSig.(2- tailed) | .816<0.001 | .623<0.001 | .653<0.001 | 1 | .214.042 | .469<0.001 | .381<0.001 |
| Cervicodiaphysealangle(CDA) | Pearson correlationSig.(2- tailed) | .269.010 | .370<0.001 | .189.073 | .214.042 | 1 | .212.044 | .245.019 |
| Vertical Offset(VO) mm | Pearson correlationSig.(2- tailed) | .633<0.001 | .602<0.001 | .316.002 | .469<0.001 | .212.044 | 1 | .687<0.001 |
| Femur head offset(FHO) | Pearson correlationSig.(2- tailed) | .572<0.001 | .704<0.001 | .381<0.001 | .381<0.001 | .245.019 | .687<0.001 | 1 |
FHD-Femur Head Diameter; FNT-Femur Neck Thickness; FNL-Femur Neck Length; FND-Femur Neck Diameter; CDA-Cervicodiaphyseal; VO-Vertical Offset; FHO-Femur head offset
Discussion
Over 80,000 artificial hip joint replacement are done annually worldwide [12]. There are regional differences in the stature of human beings so prosthesis should be designed according to specific population. Reddy et al., highlighted that a mismatch between femoral bone and stem may definitely result in micromotion which can lead to thigh pain, osteolysis and aseptic loosening [13]. If the implant is too large the femur can fracture so the tendency is to undersize for safety but highly undersized implant may fail to bond with bone [14].
Mahaisavariya B et al., combined the CT imaging with the reverse engineering technique to obtain and analyse the three dimensional inner and outer geometry of the proximal cadaveric femur [7]. Deshmukh TR et al., studied the geometry of femur in the Vidarbha (central) region of India by using the mathematical approach [15].
The anthropometric measured values and values obtained through mathematical models showed good correlation. Siwach RC and Dahiya S compared the parameters of femur of Indian cadavers with those of western, Chinese and Hong Kong population [16]. Ho Jung Cho et al., also observed the anatomic geometric differences of femur in Korean subjects from Americans and Japanese [17]. He suggested to design new hip prosthesis system for Asian population. De Sousa E et al., also evaluated the variables of proximal femur in Brazilian Population with Auto CAD 200 Software and compared it with other studies of different regions [11]. Rawal BR et al., has proposed dimensions of the cementless femoral stem for Indian population [18]. A difference of 16.8% was found in the FHO between Indian and Swiss population which can affect soft tissue tension and range of motion.
Various studies of proximal femur parameters were conducted in Asian countries also as in Malay population [19], Chinese population [20] and in Pakistani population [21]. These studies also favour the fact of regional difference in the parameters of proximal femur but the data obtained from Asian population is similar with the parameters obtained from our study [Table/Fig-10]. Some frequently described measurements that are associated with an increased risk of fracture include a longer hip axis, length of femur, a larger neck shaft angle and a larger femoral neck width [22].
Different studies of morphometry of proximal femur [9,17,19–21].
| Parameters | Present StudyN= 91 | Americans &Caucasians [9]N=200 | Chinese Population[20]N=100 | Malay Population [19]N=60 | PakistaniPopulation [21] | Korean Population [17]N=202 | Thai Population [7]N=108 |
|---|
| FHD (mm) | 42.32±4.11 | 52.09±4.43 | 45.4 | 40.81±3.43 | 50.1±3.8 | 45.50±3.39 | 43.98±3.47 |
| FNL (mm) | 44.75±8 | -- | -- | -- | -- | -- | 46.22±5.14 |
| FND (mm) | 33.02±4.22 | -- | 31.91 | -- | -- | -- | -- |
| FNT (mm) | 24.01±3.0 | -- | -- | -- | -- | -- | -- |
| CDA (deg) | 128.90±4.49 | 132.69±5.91 | 129.88 | 130.46±4.02 | 130±6.1 | 130.27±5.39 | 128.04±6.14 |
| HO (mm) | 42.92±5.5 | 41.16±6.02 | -- | 40.81±3.43 | 41.9±6.9 | 37.88±5.39 | -- |
| VO (mm) | 58.13±7.6 | 49.35±6.88 | -- | -- | -- | -- | -- |
FHD- Femur Head Diameter, FNL- Femur Neck Length, FND- Femur Neck Diameter, CDA- Cervicodiaphyseal Angle, HO- Horizontal Offset, VO- Vertical Offset.
In a retrospective study, El-Kaissai et al., suggested that Caucasian postmenopausal women with hip fracture have a longer length on femoral neck, compared to women without fractures. The risk of hip fracture increased by 24% with every one millimetre increase in the thickness of femoral neck [23]. Calis et al., obtained a similar result in Turkish women, where the width and angle of femoral neck were significantly greater in patients with hip fractures [24]. In males with increase in age, neck thickness is also increased, which contribute to the development of osteoarthritis by increasing cam impingement [25]. In the present study mean neck length was 44.75±8.0, neck thickness was 24.01±3.05 and neck diameter was 33.02±4.22 [Table/Fig-8]. Prasath RA and Ismail BM observed that femur head diameter in south Indian population was 41.98±1.98mm [26]. The Synergy hip with a 131° neck-shaft angle and a dual offset, replaced hip more reliably than does the Mallory Head component with a valgus 135° neck shaft angle [27]. So the high offset stem is also detrimental for the success of hip arthroplasty. Various population based studies have been done on proximal femur. Caucasian and Americans femurs were different from the studies done in Asian population including the Indian population too [Table/Fig-10]. In India various studies were carried out regionally. Femur parameters as FHD was 43.95±3.06, 45.41±3.06, 43.3±4.17,45.30±4.7, Femur head offset was 40.23±4.85,38.18±4.21, 36.93±5.2 and FNA was 124.42±5.49, 131.87±4.64, 123.5±4.34 and 130.57±3.0 in various studies of Indian population [7,15,16,18,28]. FNL was 48.4±5.56 and 37.2±4.65 [16,19]. FNT and diameter was 31.87±2.91 and 24.90±2.94 [16]. Regional differences in morphometry of femur in Indian population are not significant.
Limitation
Study was done on the dry bones so right and left femurs did not belong to the same individual.
Conclusion
European data based hip prosthesis are mismatched in Indians. For Indian population best fit prosthesis can be made with the help of the published data of proximal femur. These prostheses can also be used by other Asian countries as morphologically they are similar to Indian population. Structurally and functionally FHO, VO, FNL and FHD are the detrimental parameters for designing the hip prosthesis and correlation coefficient among these variables was moderate to high in our study which proves relationship among these mentioned variables.
FHD-Femur Head Diameter; FNT-Femur Neck Thickness; FNL-Femur Neck Length; FND-Femur Neck Diameter; CDA-Cervicodiaphyseal; VO-Vertical Offset; FHO-Femur head offset
FHD- Femur Head Diameter, FNL- Femur Neck Length, FND- Femur Neck Diameter, CDA- Cervicodiaphyseal Angle, HO- Horizontal Offset, VO- Vertical Offset.
[1]. Chowdhary S, Naushaba H, Begum J, Ahmed S, Khan LF, Parash TH, Morphometrical and topographical anatomy of position of nutrient foramen on fully ossified left femurDelta Med Coll J 2013 1(1):13-18. [Google Scholar]
[2]. Nurzenski MK, Briffa NK, Price IR, Khoo CCB, Devine A, Beck JT, Geometric indices of bone strength are associated with physical activity and dietary calcium intake in Healthy older womenJ Bone Miner Res 2007 22(3):416-24. [Google Scholar]
[3]. McGrory J, Morrey BF, Chahalan TD, Kai-Nan AN, Cabanela ME, Effect of femoral offset on range of motion and abductor muscle strength after total hip arthroplastyJ Bone Joint Surg 1995 77(B):865-69. [Google Scholar]
[4]. Rubin PJ, Leyvraz PF, Aubaniac JM, Argenson JN, Esteve P, Roguin BD, The morphology of the proximal femur: a three dimensional radiographic analysisJournal of bone and Joint Surgery B 1992 74(1):28-32. [Google Scholar]
[5]. Hushmann O, Rubin PJ, Leyvraz PF, De Roguin B, Argenson JN, Three dimensional morphology of the proximal femurJ Arthroplasty 1997 12(4):444-50. [Google Scholar]
[6]. Ahmad M, Nanda R, Bajwa AS, Couto JC, Green S, Hui AC, Biomechanical testing of the locking compression plate: when does the distance between bone and implant significantly reduce construct stability? Injury 2007 38(3):358-64. [Google Scholar]
[7]. Mahaisavariya B, Sitthiseripratip K, Tongdee T, Bohez EL, Vander SJ, Oris P, Morphological study of the proximal femur: A new method of geometrical assessment using 3-dimensional reverse engineeringMed Engg Phys 2002 24(9):617-22. [Google Scholar]
[8]. Menezes TM, Rocha TDS, De Oliveira BDR, De Albuquerque YML, Caiaffo V, Proximal femoral epiphysis: Manual morphometry versus digital morphometryInt J Morphol 2015 33(3):1114-19. [Google Scholar]
[9]. Unnanuntana A, Toogood P, Hart D, Cooperman D, Grant RE, Evaluation of proximal femoral geometry using digital photographsJournal of Orthopaedic Research 2010 28:1399-404. [Google Scholar]
[10]. Mourao AL, Vasconcellos H, Geometry of the proximal femur in Brazilian bonesActa Fisiatrica 2001 8(3):113-19. [Google Scholar]
[11]. De Sousa E, Fernandes RMP, Mathias MB, Rodrigues MR, Ambram AJ, Babinski MA, Morphometric study of the proximal femur extremity in BraziliansInt J Morphol 2010 28(3):835-40. [Google Scholar]
[12]. Granger C, Schutte HD, Bigger SB, Kennedy JM, Latour RA, Failure analysis of composite femoral component for hip arthroplastyJ Rehab Res Develop 2003 40:131-46. [Google Scholar]
[13]. Reddy VS, Moorthy GV, Reddy SG, Do we need a special design of femoral component of total hip prosthesis in our patients?Indian J Orthop 1999 33:282-84. [Google Scholar]
[14]. Vaidya SV, Ranawat CS, Aroojis A, Laud NS, Anthropometric measurements to design total knee prostheses for the Indian populationJ Arthroplasty 2000 15:79-85. [Google Scholar]
[15]. Deshmukh TR, Kuthe AM, Ingole DS, Thakre SB, Prediction of femur bone geometry using anthropometric data of Indian population: A Numerical ApproachJ Med Sci 2010 10(1):12-18. [Google Scholar]
[16]. Siwach RC, Dahiya S, Anthropometric study of proximal femur geometry and its clinical applicationIndian Journal of Orthopaedics 2003 37(4):247-51. [Google Scholar]
[17]. Cho HJ, Kwak DS, Kim IB, Morphometric evaluation of Korean Femur by geometric computation: comparisons of the sex and the populationBiomed Research Int 2015 2015:7305389 pages [Google Scholar]
[18]. Rawal BR, Rubeiro R, Malhotra R, Bhatnagar N, Anthropometric measurements to design best fit femoral stem for Indian populationIndian J Orthop 2012 46(1):46-53. [Google Scholar]
[19]. Baharuddin MY, Zulkifly AH, His M, Aziz AA, Three dimensional morphometry of the femur to design the total hip Arthroplasty for Malay PopulationAdvanced Science Letters 2013 19(10):2982-87. [Google Scholar]
[20]. Lin KJ, Wei HW, Lin KP, Tsai CL, Lee PY, Proximal femoral morphology and the relevance to design of Anatomically precontoured plates: A study of the Chinese populationThe Scientific World Journal 2014 2014:1069416 pages [Google Scholar]
[21]. Umer M, Sepah A, Khan A, Morphology of the proximal femur in the Pakistan populationJ Orthop Surg 2010 18:279-81. [Google Scholar]
[22]. Bhattacharya S, Chakraborty P, Mukherjee A, Correlation between neck shaft angle of femur with age and anthropometry: A Radiographic studyIndian Journal of basic and applied Medical Research 2014 3(3):100-07. [Google Scholar]
[23]. El Kaissai S, Pasco JA, Henry MJ, Panahi S, Nicholson JG, Nicholson GC, Femoral neck geometry and hip fracture risk: the Geelong osteoporosis studyOsteoporosis Int 2005 16:1299-303. [Google Scholar]
[24]. Calis HT, Eryavuz M, Calis M, Comparison of femoral geometry among cases with and without hip fracturesYonsei Med J 2004 45:901-07. [Google Scholar]
[25]. Johnson JK, Renner JB, Dahners LE, Anteroposterior thickening of the femoral neck with aging decreases the offset in menAm J Sports Med 2012 40(10):2213-17. [Google Scholar]
[26]. Prasath RA, Ismail BM, A correlative study of morphometric analysis of acetabulum and femoral head in male and female south Indian human cadaversJournal of Science 2014 4(1):4-8. [Google Scholar]
[27]. Dolhain P, Tsigaras H, Bourne RB, Rorabach CH, Donald SM, Mc Calden R, The effectiveness of dual offset stems in restoring offset during total hip replacementActa Orthopaedica Belgica 2002 68(5):490-99. [Google Scholar]
[28]. Roy S, Kundu R, Medda S, Gupta A, Nanrah BK, Evaluation of Proximal femoral geometry in plain anteroposterior radiograph in Eastern-Indian populationJournal of Clinical and Diagnostic Research 2014 8(9):1-3. [Google Scholar]