In the last decade, we have seen a significant surge in the number of patients whom we can term as “Informed patients”. Informed patients are well read on the medical condition that they are looking to resolve. They may have often over researched and may be paranoid about what they may be going through; they may also know all potential medications that may be used for treatment and also potential side effects of these. However, they may not be in a position to judge what is actually right and what is actually applicable for what they are going through. This causes patients to go through, what we define as hyper information, where they have a lot of information but are unaware what applies to them.
In this paper, we classify patients driven by this hyper-information, and discuss how this may lead to different patient states. We also discuss the need for doctors to adapt themselves to become what we call Hybrid Doctors. We briefly discuss how Hybrid Doctors can handle informed patients of various types and states.
Introduction
The present day use of the Internet for finding health information may affect the relationship between health professionals and patients, as observed by Kivits J [1]. His study findings show the importance of the ‘everyday’ in orientating health information searches and of personal experience in navigating a multiplicity of online sources [1]. The study stresses on the role of doctor-patient relationship changing through the advent of informed patient.
Informed patients are well read on the problem that they are looking to resolve. They may have often over researched and may be paranoid about what they may be going through; they may also know all potential medications that may be used for treatment and also potential side effects of these. However, they may be unaware of what is actually right, what is actually applicable for what they are going through. This causes patients to go through, what we define as hyper information, where they have a lot of information but are unaware what applies to them.
We are also in the midst of what has been termed as “participative patient”, thanks to the advent of Web 2.0 [2], It is important to note that this change in the ecosystem is a good change, and helps the ecosystem to leverage technology and its reach, to solve medical and dental problems across unreachable geographies. There is a need for doctors to help create more informed patients to increase the reach of the doctors in the virtual world and at the same time maintain the sanctity of the medical information available. The doctors will therefore, have to transform themselves into what we call as Hybrid Doctors, where they are available both in physical and virtual world lending their experiences to drive proper decision making.
Hyper-information: When patients can be informed; they can be misinformed too.
In today’s world, 80% people using the internet for searching information do so for getting access to medical information. People are increasingly becoming conscious about their health and want to be well informed about it. Most of the people use a ‘search engine’ when they begin their search for health information on the internet. Many don’t check for the veracity of the medical information they gather online [3].
We believe that the effect of informed patient can go to the extremes. On one hand, it may educate the patient, leading him/her to “self medicate” accurately or equip him/her to rightly ignore some symptoms he/she is seeing as a common seasonal root cause. On the other hand, it may also lead to completely misguided patients who may end up ignoring doctor’s advice while trusting information which may not be authentic or which is authentic but not relevant for the patient.
We classify these patients into various buckets by identifying two important but orthogonal factors.
One: Is the information that is available for the topic authentic? Is it coming from a well read doctor or a half read patient? We call this axis as Authenticity
Two: Is the information accessed by the patient online rightly applicable to the patient’s age, sex, his/her geographical location and other contributory factors? We call this axis as Relevance
[Table/Fig-1] depicts a type quadrant with these two orthogonal factors, to show informed patient types depending on what he/she reads, and how he/she comprehends and applies this understanding. The y-axis shows the accuracy and authenticity of the information a patient is reading while the x-axis shows the relevance of that information. As you can see, each quadrant classifies the patient in different types.
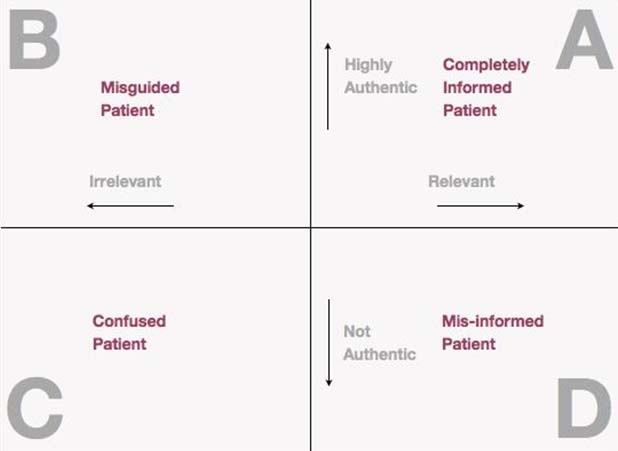
Completely Informed Patient (Type A): In this type, the patient has read authenticated and accurate information, and has applied this information correctly and relevantly to the symptom he/she is seeing. The patient in this quadrant is well informed and even if he/she goes to the extent of self-medication, he/she is most likely going to be right. We choose to call them Completely Informed Patients to distinguish them from the patients in other quadrants.
Misguided Patient (Type B): In this type, the patient has accessed authentic information but he/she is not able to correctly apply this information to his/her symptoms, leading the patient to be misguided. Here, the doctor can intervene to help this Type B informed patient and guide him/her in the right ways to analyze the symptoms and apply the information gathered online to his/her context, thus effectively converting this misguided patient into a well informed patient.
Confused Patient (Type C): In this type, the patient has read mostly unauthentic information, and has applied this to irrelevant symptoms leading him/her to be confused as to what is right. In such a case, the doctors will have to ensure that the patient takes treatment directly from doctor without indulging in self diagnosis and self medication, while slowly helping the patient to start reading authentic sources. The doctors should also help the patient to identify symptoms relevant to the diagnosis properly.
Misinformed Patient (Type D): In this type, the patient has applied unauthentic information to his/her symptoms leading him/her to be misinformed. Doctors should ensure that the right sources are provided to such patients for accessing authentic information.
Brief Survey and Findings
A survey was conducted with a few questions about informed patients relevant to the aim of this study. The intention of this survey was to see if there are patients in all of these types, or is it just a statistical hyperbole. The survey was conducted with doctors across India (n=92). The doctors were from both medical and dental fraternity who responded to this questionnaire. The questionnaire was sent to the known contacts comprising of doctors and dentists. And all of them responded which is n=92. Hence, response rate was 100%. The questionnaire was validated by 5-6 experts and validation was about 90% and was reliable. The meaning of the word informed patient and the brief purpose of the study was explained in the questionnaire followed by the questions. Online questionnaire was sent by mail link and response were recruited online and was recorded in excel spread sheet.
Type A patients were very small in number.
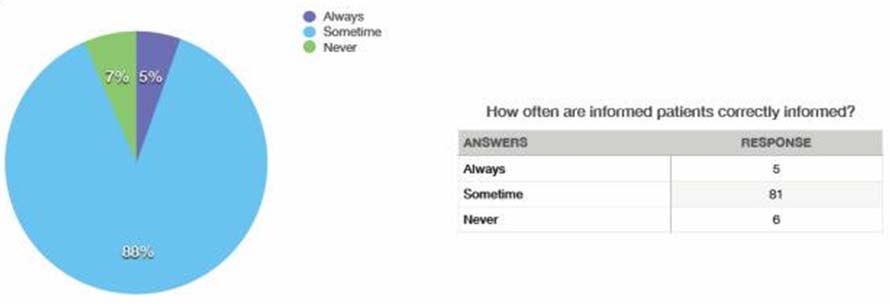
Our survey indicated that, around 5% of the patients of all the doctors we surveyed were completely informed patients – inference drawn by the response “always” which is about 5% as given in [Table/Fig-2] which means, they are correctly informed and have also applied this information to their symptoms correctly.
Response to the question “how often are informed patients correctly informed?”
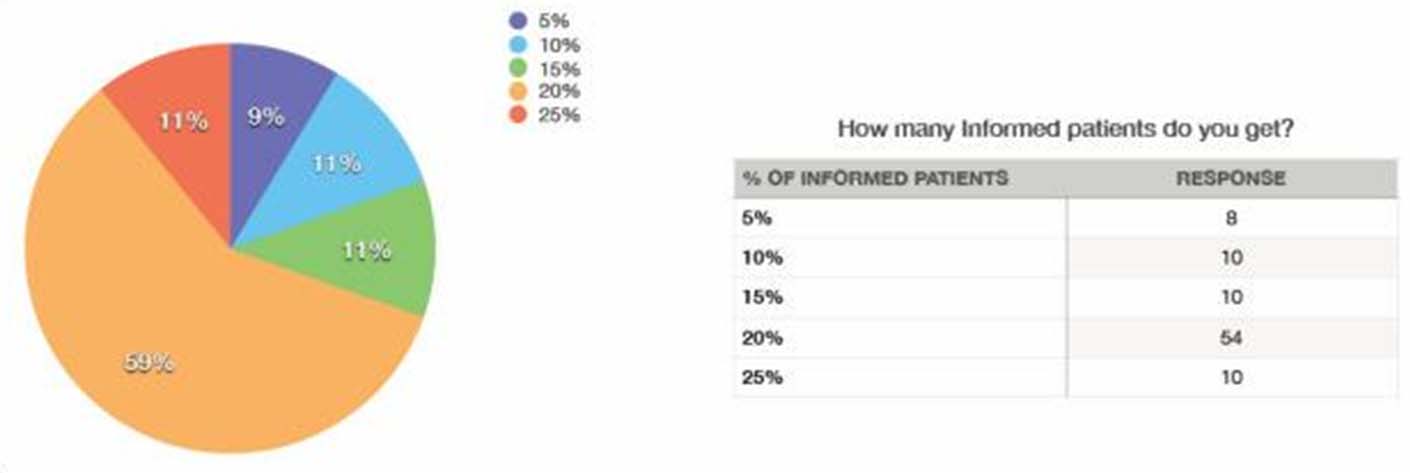
A direct question: how many informed patients do they get? [Table/Fig-3] resulted in 59% doctors answering around 20% are informed patients. In this 20%, 5% are completely informed patients as mentioned above and the remaining 15% (close to 75% of the total informed patients) are Type B, C or D.
Response to the question “How many informed patients do you get?”
It was also interesting to see that the 7% of doctors felt that patients are never correctly informed [Table/Fig-2]. This shows that there is a significant number of patients falling in Type C and Type D, as informed patient according to us are the ones who are completely informed.
Once an Informed patient is NOT always an informed patient.
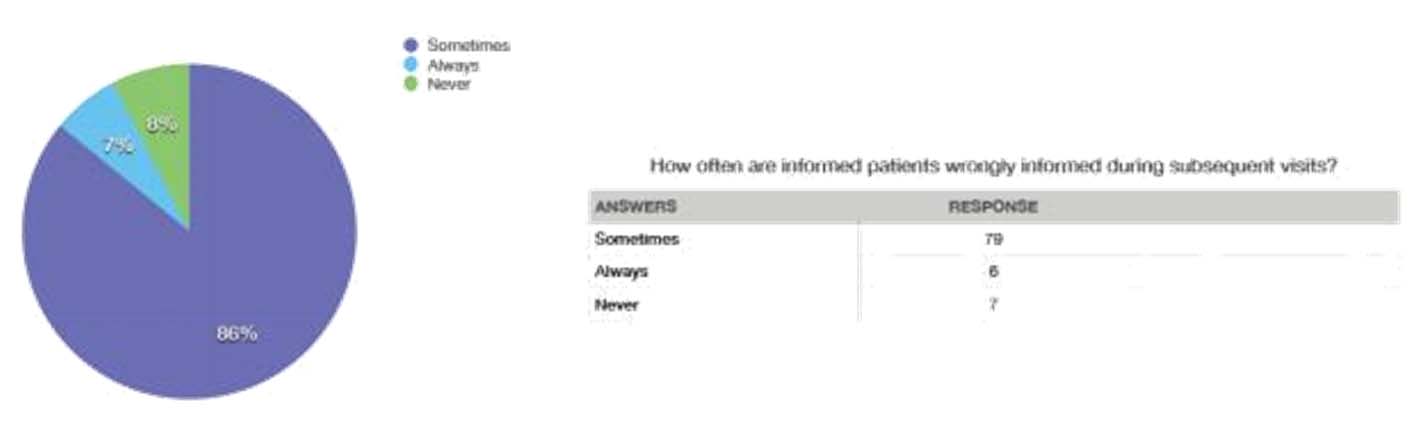
The key thing that emerged from the survey was that the Type is a temporal state, and an informed patient may move to a different type depending on what kind of information he accesses at different points in time. The context in which he/she applies the information also keeps on changing. This is supported by the data in [Table/Fig-4] where 86% of doctors said sometimes and 7% of doctors said patients are always wrongly informed in subsequent visits.
Response to the question. “How often an informed patient wrongly informed during subsequent visits?”
While this was not a direct revelation from the survey, we deduced from discussions during these surveys that the answers were changing depending on how often they had met some of the patients.
States of an Informed Patient
Along with the types, we also define states of these patients to help doctors to involve themselves in moving them into Type A quadrant. The fact to remember here is that the patient always believes that he is a Type A informed patient. He always thinks that he has read the right information and also applied it to the symptoms accurately. It is only when he doesn’t get the desired result or worse when he gets an adverse result that he realizes he may have been wrong, which may be too late in managing the disease.
We identified the following states, a patient can get into:
State of Disillusionment: A person who remains in Type C and Type D, will most likely get into a state of disillusionment. He questions everything that the Doctor says and even the information that is available on the internet.
State of Over Confidence: A person who remains mostly in Type A, feels that he is able to understand nuances of medical treatment by quickly going through the information on the internet and applying it to his symptoms. He may tend to be so over confident that he feels that he is now capable of diagnosing and treating his near and dear ones as well by his internet acquired medical knowledge.
State of Pessimism: A person who remains in Type B will get into a state of pessimism. Since, he is unable to apply the information he has accessed on the internet to arrive at a diagnosis of his problem and for its treatment, he/she naturally starts suspecting the authenticity of this very information, even when it is vouched to be correct by the doctors. He/she will also start seeing medical science and diagnostics with pessimism.
Given that these states are temporal in nature, it is important that there is a serious and continuous effort by Hybrid doctors to understand these states, manage them and try to keep all the patients in Type A quadrant, who are completely informed with highly authentic and relevant information.
Gerber BS and Eiser AR in their article have discussed that the information on net can give rise to two types of informed patients. One is informed decision maker, who not only knows the information about his/her health condition but also takes part in decision making with the doctor. The doctor can utilize the time available in refining his knowledge instead of starting from basics, provided the obtained information is accurate. The second type is the knowledge acquirer i.e., an informed patient but less assertive and does not show interest in participating in decision making. The doctor in this case may be the final formulator of decision making [4,5].
The information quadrant model of our study should help us to identify the specific type of informed patient and this should help doctors to handle their patients better and with confidence.
The Role of a “Hybrid Doctor”
We believe that the patients in any Type (other than Type A), in addition to being treated medically, need to be counseled to help them make sense of the information available on the net and help them make an informed decision. The intention of doctors should be to ensure all of his/her patients remain in Type A quadrant.
Our views on the expectation from such doctors are as follows:
Understanding Information Flow: Doctors should be connected to the internet to understand where information is available, which information is accurate and primarily where this information is getting generated. They should spend time on the net, with this as the main purpose.
Course Correct Deviations: Doctors should also be watching out for misguiding data on the internet and provide authentic and authorized data to clarify any doubts created due to this dubious information present on the net. They should also discuss constraints of using this information available on the net.
Virtual Consultation: Doctors should also consider having their own virtual consultation office to discuss what kind of medical information patients are accessing on the net. They will then be in a position to guide the patients to apply this information properly to solve their own problem. This will also help doctors understand information flow in a much better fashion.
Lending Localization and Seasonal Knowledge: Given that the internet remains global, patients normally are misguided by applying information appropriate for a different geographical location and climate to themselves. Doctors should be watchful to prevent this and bring clarity on what is relevant for a patient given his geographical location and also the season that is currently on.
Discussion Oriented Medication: On encountering an informed patient, the doctors should have an open discussion on what the patient thinks should be the treatment, to understand what they are reading and how they are applying this knowledge. This again helps them to understand the information flow within the internet in a much better fashion.
There have been tectonic societal shifts in the past few years with the emergence of the internet. Plethora of health related websites and many other sources of medical information has given patients a false belief, who think that they can manage their own or even their families medical affairs, with physicians serving primarily as consultants. While this belief may not be totally correct, has lead to the development of a relationship between doctors and patients who involve in shared decision making [6]. This has lead to the development of Hybrid doctors. The Hybrid doctor should aim at incorporating patient preferences in clinical decision making, which in turn requires adequate and right information, communication and education. So, the role of a Hybrid doctor is to guide the wrongly informed or uninformed patients to the right source of information. The National Library of Medicine spearheads several consumer health initiatives, such as Medline Plus, NIH Senior Health, and ClinicalTrials.gov, designed to get medical information directly into the hands of patients [7–9].
The internet age is altering the patient-physician relationship. If physicians actively assist patients in the information-gathering process, an improved relationship may result.
The foundation of a positive patient–physician relationship rests on mutual trust, confidence and respect. Patients are not only more compliant when they perceive their doctors as being competent, supportive and respectful, but also more likely to discuss important information with them [10,11].
Recommendations for doctors to adapt to changing trends to become hybrid doctors:
Doctors should become more conversant with the working of the internet. They should make efforts to learn using the internet for searching information even if they were raised in the era when internet was not the primary source of information.
The doctors should spend time on the internet and zero in on sites which give relevant information in a language free from medical jargon so that the patient can understand it better and apply it sensibly.
Doctors should also educate the patient that medical science is a highly specialized subject which requires both analysis of symptoms and skilful elicitation of signs. The diagnosis can be arrived at only after this and not just by feeding a few symptoms in to a search engine.
The "deliberative" or "participatory" decision-making model is recommended, which involves both doctors and patients’ active participation in treatment decision-making in the clinical encounter [12–14].
Patients’ acceptance of diagnosis and treatment plans depends on education. Patients with poor literacy skills cannot take advantage of the internet to acquire additional medical knowledge. Hence, additional efforts are required to assist persons with lower literacy skills [15].
Physician offices with health information kiosks may be an alternative method for browsing health-related information, being temporally linked to clinician interactions [16].
Conclusion
With our survey, it is clear that the number of informed patients is on the rise and is going to rise further as the net-native (internet savvy) generation reaches its teens. This would mean that the number of informed patients will continue to rise from the figure of 20% that this survey indicates. It is alarming that 3/4th of these 20% informed patients do not fall in the completely informed category. It is also clear that a completely informed patient may not remain in that state always.
Given the above two, it is important that doctors adapt themselves and transform themselves into Hybrid doctors. We discuss the role they can play and help the up coming ecosystem self sustain with the number of Type B, C and D patients kept to the minimum.
[1]. Kivits J, Informed patients and the internet a mediated context for consultations with health professionalsJ Health Psychol 2006 1(2):269-82. [Google Scholar]
[2]. Gardiner R, The transition from ‘informed patient’ care to ‘patient informed’ careStud Health Technol Inform 2008 137:241-56. [Google Scholar]
[3]. Fox S, Health Information Online. [Web Document]Pew Internet Fund 2005 May17. [cited 26 Jul 2006] <http://www.pewinternet.org/PPF/r/156/report_display.asp>. Last accessed on 15th July 2015 [Google Scholar]
[4]. Gerber BS, Eiser AR, The patient-physician relationship in the internet age: Future prospects and the research agendaJ Med Internet Res 2001 3(2):e15 [Google Scholar]
[5]. Beisecker AE, Patient information-seeking behaviors when communicating with doctorsMed Care 1990 28(1):19-28. [Google Scholar]
[6]. Truog RD, Patients and doctors — The evolution of a relationshipN Engl J Med 2012 366:581-85. [Google Scholar]
[7]. Miller N, Lacroix EM, Backus JE, MEDLINE plus: Building and maintaining the National Library of Medicine’s consumer health web serviceBull Med Libr Assoc 2000 88(1):11-17. [Google Scholar]
[8]. National Institutes of Health. NIHSeniorHealth. [Web document]. Bethesda, MD: The Institutes, 2006. [rev. 7 July 2006; cited 25 July 2006]. <http://nihseniorhealth.gov/>. Last accessed on 17th July 2015 [Google Scholar]
[9]. McCray AT, Dorfman E, Ripple A, Ide NC, Jha M, Katz DG, Usability issues in developing a Web based consumer health siteProc AMIA Symp 2000 :556-60. [Google Scholar]
[10]. Truog RD, Patients and doctors—The evolution of a relationshipN Engl J Med 2012 366:581-85. [Google Scholar]
[11]. Petrilli CM, Mack M, Petrilli JJ, Hickner A, Saint S, Chopra V, Understanding the role of physician attire on patient perceptions: A systematic review of the literature— targeting attire to improve likelihood of rapport (TAILOR) investigatorsBMJ Open 2015 5:e006578 [Google Scholar]
[12]. Charles C, Gafni A, Whelan T, Shared decision-making in the medical encounter: What does it mean? (or it takes at least two to tango)Soc Sci Med 1997 44(5):681-92. [Google Scholar]
[13]. Kaplan SH, Greenfield S, Gandek B, Rogers WH, Ware JE, Characteristics of physicians with participatory decision-making stylesAnn Intern Med 1996 124(5):497-504. [Google Scholar]
[14]. Ballard-Reisch DS, A model of participative decision making for physician-patient interactionHealth Communication 1990 2:91-104. [Google Scholar]
[15]. Grueninger UJ, Arterial hypertension: Lessons from patient educationPatient Educ Couns 1995 26(1-3):37-55. [Google Scholar]
[16]. Glasgow RE, Mckay HG, Boles SM, Vogt TM, Interactive computer technology, behavioral science, and family practiceJ Fam Pract 1999 48(6):464-70. [Google Scholar]