“Zebra Stripe” Sign and “Bone in Bone” Sign in Cyclical Bisphosphonate Therapy
Partha Pratim Chakraborty1, Sugata Narayan Biswas2, Shinjan Patra3, Gouranga Santra4
1 Assistant Professor, Department of Medicine, Midnapore Medical College and Hospital, Midnapore, West Bengal, India.
2 Postgraduate Trainee, Department of Medicine, Midnapore Medical College and Hospital, Midnapore, West Bengal, India.
3 Postgraduate Trainee, Department of Medicine, Midnapore Medical College and Hospital, Midnapore, West Bengal, India.
4 Associate Professor, Department Medicine, Midnapore Medical College and Hospital, Midnapore, West Bengal, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Partha Pratim Chakraborty, House No. BE:64; Bidhan Nagar (East); PO: Midnapore-721101, West Bengal, India.
E-mail: docparthapc@yahoo.co.in
Metaphysis, Osteoclastic activity, Picture frame vertebrae
With expanding usage of bisphosphonates as an antiresorptive agent in a wide spectrum of paediatric skeletal disorders, physicians need to be familiar with the expected adverse drug reactions including imaging changes of bones.
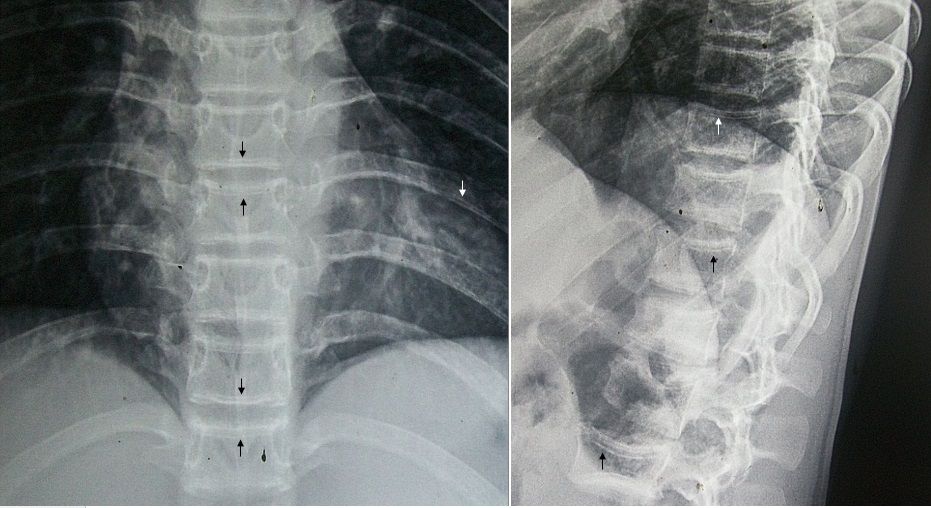
A 15-year-old boy with history of multiple fragility fractures of the long bones since early childhood and subsequently diagnosed with juvenile osteoporosis, presented to our outpatient facility for follow up. Oral calcium, cholecalciferol and intravenous zoledronate had been prescribed to mitigate increased bone fragility and associated musculoskeletal symptoms. A total of three cycles of intravenous Zoledronate (5 mg per year) were administered prior to this presentation. Radiological skeletal survey revealed transverse sclerotic bands (maximum three in number, corresponding to the number of bisphosphonate doses received) in the metaphysis of femur, proximal tibia, proximal fibula, ilium, ischial tuberosities, acetabulum, radius, distal ulna, metacarpals, phalanges and vertebral bodies, analogous to the striped-appearance of a zebra [Table/Fig-1,2,3 and 4]. “Zebra stripe” sign is radiological manifestation of cyclical bisphosphonate therapy prior to closure of epiphyseal growth plates and are seen in about half of the users. Appearance of these bands in the vertebral bodies gives rise to a “bone in bone” (after intermittent use) or a “picture frame” (after continuous use) appearance equivalent to the “zebra stripe” sign in the long bones [1]. Bisphosphonates inhibit osteoclastic activity, reduce bone resorption and turnover, with resultant prolonged lifespan of bone tissue and increased duration for secondary mineralisation of bone. These lines usually develop after about two months of initiation of therapy and are believed to be the outcome of establishment of a new balance between osteoblastic and osteoclastic activities [2]. Temporary interruption of growth plate cartilage resorption induced by bisphosphonates and the relative increase in bone formation with high levels of osteoblastic activity on the metaphyseal side of the growth plates leads to the development of sclerotic lines.
Antero-posterior radiograph of pelvis showing zebra stripes (white arrows) in the metaphyses of ilium, ischium, acetabulum and femoral head bilaterally.

Antero-posterior radiograph of knee joints showing zebra stripes (arrows) involving metaphyses of distal femur, proximal tibia and fibula, bilaterally.

Antero-posterior and lateral radiographs of vertebral column showing “bone in bone” appearance (arrows) in the vertebral bodies.
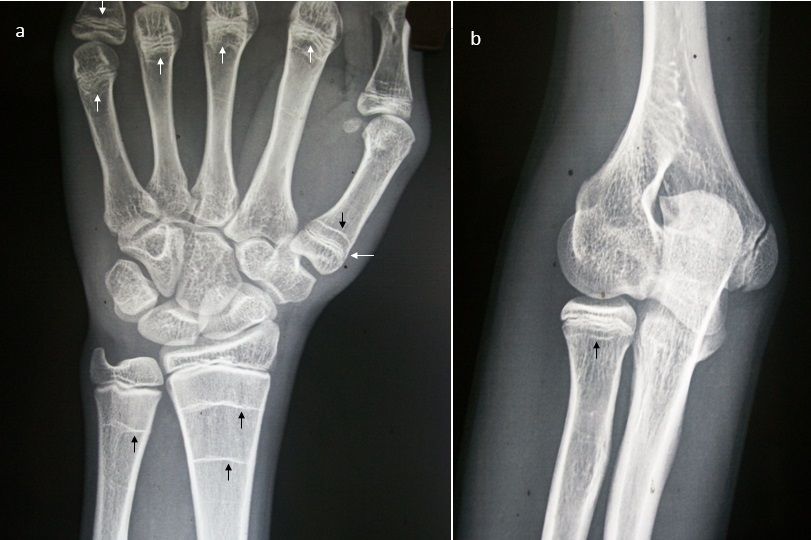
Antero-posterior radiograph of right wrist joint revealing zebra stripes (arrows) involving metaphyses of distal radius, distal ulna, metacarpal heads and fifth proximal phalanx (a) and antero-posterior radiograph of right elbow joint revealing zebra stripes (arrow) involving metaphysis of proximal radius (b).
Histologically, there is a failure of physeal differentiation of primary spongiosa into secondary. In between cyclical bisphosphonate therapy, further growth leads to formation of new bone with normal lucency and the growth plate gradually moves away from these newly created horizontal trabeculae, which then become visible as sclerotic lines on radiographs. Thus, areas of radio-opaque sclerotic bands alternating with those of normal lucency give rise to stripes akin to a zebra. The number of radio-opaque lines corresponds closely to cycles of bisphosphonates received. The inter-linear distance depends on rate of bone growth, frequency of bisphosphonate administration and age of patient. With discontinuation of therapy, zebra lines progressively migrate and disappear into diaphysis. After physeal closure, further bands do not appear, irrespective of ongoing bisphosphonate therapy. Moreover, they are reversible after discontinuation of the medication, although the exact time span to complete disappearance is not known due to prolonged half-life of bisphosphonates when incorporated into bones [3].
The clinical implications of this imaging finding are largely unknown. Conditions which lead to repeated growth suppression with subsequent recovery may give rise to similar transverse bands, known as growth arrest lines or Harris lines. Thus, healing rickets, heavy metal and thorotrast intoxication, oxalosis and chronic anaemia should be considered while evaluating similar radiographic appearance in a growing child.
To conclude, with expanding usage of bisphosphonates in a wide spectrum of paediatric skeletal disorders physicians need to be familiar with the expected imaging changes of bones associated with usage of this agent.
[1]. van Persijn MEL, Kroon HM, Papapoulos SE, Epi and metaphyseal changes in children caused by administration of bisphosphonatesRadiology 1992 184(1):249-54. [Google Scholar]
[2]. Reitsma PH, Bijvoet OL, Verlinden-Ooms H, Van der Wee-Pals LJ, Kinetic studies of bone and mineral metabolism during treatment with (3-amino-1-hydroxypropylidene)-1, 1-bisphosphonate (APD) in ratsCalcif Tissue Int 1980 32:145-57. [Google Scholar]
[3]. Fernandes JL, Viana SL, Rocha AL, Ribeiro MC, Castro LC, Bisphosphonate-induced radiographic changes in two pediatric patients with rheumatic diseasesSkeletal Radiol 2004 33:732-36. [Google Scholar]