Metastasis of Synovial Sarcoma of Thigh to Lung Presenting as Whole Lung Mass
Gourahari Pradhan1, Nibedita Sahoo2, Tapan Kumar Sahoo3, Mamita Nayak4
1 Senior Resident, Department of Pulmonary Medicine, All India Institute of Medical Sciences, Bhubaneswar, Odisha, India.
2 Senior Resident, Department of Pathology, All India Institute of Medical Sciences, Bhubaneswar, Odisha, India.
3 Senior Resident, Department of Radiation Oncology, All India Institute of Medical Sciences, Bhubaneswar, Odisha, India.
4 Senior Resident, Department of Pathology, All India Institute of Medical Sciences, Bhubaneswar, Odisha, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Gourahari Pradhan, Senior Resident, Department of Pulmonary Medicine, All India Institute of Medical Sciences, Bhubaneswar-751019, Odisha, India.
E-mail: drghpradhan@gmail.com
Excision biopsy, Immunohistochemistry, Pleural effusion
A 35-year-old male patient presented with breathlessness for 10 days with vitals as follows, pulse rate 140/minute and blood pressure 100/60 mmHg. Patient had no significant past medical/family history. There was a swelling over anterolateral aspect of right thigh [Table/Fig-1] which was not painful, and stony dull note on percussion over left hemithorax. Surgical resection of the thigh mass was done in January 2016 outside our institute. Patient presented to us in June 2016. Chest skiagram revealed left whole lung opacity, shifting of mediastinum to opposite side and obliterated left costophrenic angle indicating a left massive pleural effusion. Thoracentesis performed to provide immediate symptomatic relief to patient resulted in dry tap. CT scan of thorax showed left whole lung mass lesion of size 21.4 cm x 15.4 cm with right lung multiple macronodules [Table/Fig-2]. CT scan of thigh revealed a heterogenously enhancing spindle shaped mass on anterolateral aspect of right thigh with interspersed areas of calcification [Table/Fig-3]. CT guided biopsy of the mass lesion was done after stabilisation of vitals. Histopathology revealed linear cores of a hypercellular tumour, comprising of monotonous looking spindle cells arranged in short fascicles, vague storiform pattern and focal haemangiopericytoma like areas, the cells had scant cytoplasm and spindle shaped plump hyperchromatic nuclei [Table/Fig-4]. Immunohistochemistry showed tumour cells positive for Bcl-2, CD99 and focally positive for Epithelial Membrane Antigen (EMA) and negative for CD34 suggesting a diagnosis of biphasic Synovial Sarcoma (SS) of lung [Table/Fig-5]. Previously USG colour doppler of right lower limb showed large heterogenous hypoechoic soft tissue mass lesion of approximate size 15 cm x 10.5 cm x 6 cm with appreciable internal vascularity and scattered necrotic areas in posterior aspect of right thigh and popliteal fossa region deep to muscle plane, possible soft tissue sarcoma. Fine Needle Aspiration Cytology (FNAC) of thigh swelling revealed moderately cellular cytosmear with plump spindle cells showing mild pleomorphism present in clusters and discrete manner with haemorrhagic background suggesting spindle cell tumour. Upon excision biopsy, macroscopic appearance [Table/Fig-6] showed irregular brownish soft friable mass lesion measuring 7 cm x 7 cm x 6 cm and microscopic findings demonstrated cellular neoplasm having proliferating fascicles of spindloid to ovoid cells having mostly bland nuclei with occasional mitosis, fibrocollagenous area with foci of haemorrhage. Immunohistochemistry was positive Bcl-2, CD99 and β-catenin and negative for CD34. Biopsy was reported, it to be as SS of thigh. Three months following excision of thigh mass he developed left pleural effusion for which tube thoracostomy was done. At the same time, he was given one cycle of chemotherapy with Adriamycin and Ifosfamide. The FNAC slide and biopsy tissue block were not available for review. Patient opted for palliative home based care and discontinued follow up.
Mass lesion over anterolateral aspect of right thigh.

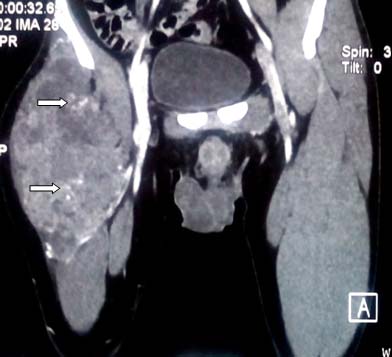
CT scan of thorax showing left whole lung mass with two macronodules in right lung.

CT Scan of thigh showing heterogenously enhancing spindle shaped mass over right thigh with areas of calcifications.
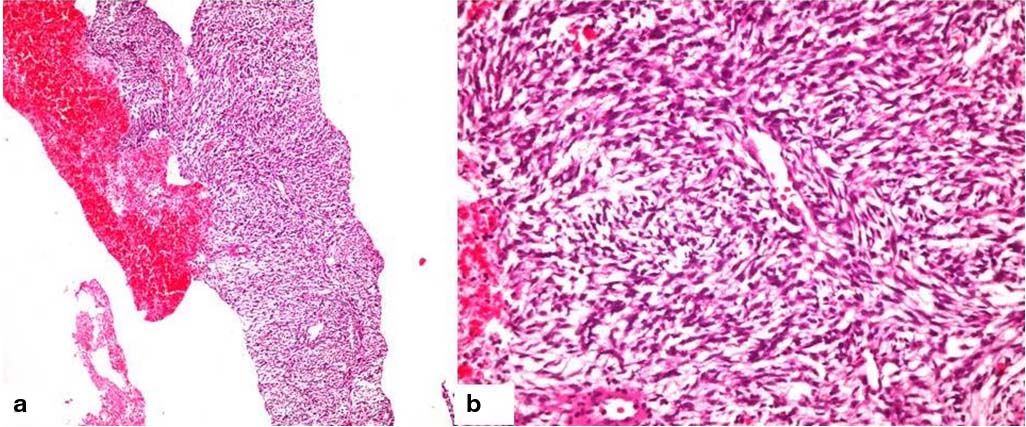
a) low power view showing a cellular tumour comprising of spindle cells arranged in short fascicles and vague storiform pattern (H&E 100X). b) Higher magnification of the same (H&E 400X).
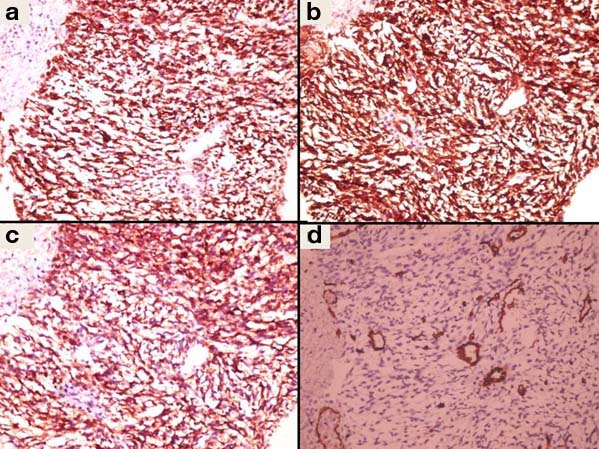
Immunohistochemistry showing tumour cells are immunopositive for Bcl-2 (a); CD99 (b); focal positive for EMA (c); and negative for CD34 (d) (400X).
Irregular brownish friable mass lesion measuring 7cm x 7cm x 6cm.

SS is a morphologically, clinically and genetically distinct entity and accounts for 5-10% of soft tissue sarcomas. It occurs mainly in adolescents and young adults between 15-30 years of age with equal sex distribution. They are located usually in the extremities around large joints most commonly the knee and lower thigh region [1]. In most cases, lung metastasis develop after primary tumour surgery. Metastasis from extrapulmonary sarcomas are more common than primary pulmonary sarcomas. SS is a distinctive soft tissue tumour having epithelial differentiation. Histologically, it can be monophasic or biphasic with no significant difference in prognosis. The classical biphasic type is easily diagnosed based on the presence of both epithelial and spindle cell component. Poorly differentiated SS can be diagnostically challenging as it can occur either in monophasic or biphasic forms. Immunohistochemistry and molecular techniques play an important role in the diagnosis [2]. The prognosis for patients with SS of extremities is poor. The poor prognostic factors are biphasic tumour type, metastasis at first diagnosis and inadequate surgical margins [3]. In general, treatment of soft tissue sarcomas comprises a combination of surgical resection, radiotherapy, and chemotherapy; there are no guidelines for optimal treatment due to the rarity of these tumours. Surgical resection with tumour negative margins is the primary treatment with adjuvant chemotherapy and/or radiotherapy. Systemic chemotherapy is often administered in palliative cases where surgical resection is not possible [4].
We present this case as a primary SS of thigh with bilateral lung metastsis. Points of clinical interest in this case are metastasis to lung initially presented as pleural effusion followed later by mass lesion. Whole lung mass is usually a manifestation of primary malignancy but in this case, it was metastasis. SS are highly malignant tumours with poor prognosis and need to be managed aggressively with multimodality approach i.e., surgical resection, chemotherapy and radiotherapy at the earliest.
[1]. Rajwanshi A, Srinivas R, Upasana G, Malignant small round cell tumoursJ Cytol 2009 26:1-10. [Google Scholar]
[2]. Arafah M, Zaidi SN, Poorly differentiated monophasic synovial sarcoma of the mediastinumIndian J Pathol Microbiol 2011 54(2):384-87. [Google Scholar]
[3]. Wisanuyotin T, Radapat K, Sirichativapee W, Paholpak P, Kosuwon W, Sumnanoont C, Prognostic factors and clinical outcomes in synovial sarcoma of the extremitiesAsia Pac J Clin Oncol 2013 9(1):80-85. [Google Scholar]
[4]. Eilber FC, Dry SM, Diagnosis and management of synovial sarcomaJ Surg Oncol 2008 97:314-20. [Google Scholar]