A Comparison of Antibacterial Efficacy of 0.5% Sodium Fluoride Impregnated Miswak and Plain Miswak Sticks on Streprococcus mutans - A Randomized Controlled Trial
Romshi Raina1, Vinod Kumar2, Madhusudan Krishna3, Sakshi Raina4, Ashish Jaiswal5, Arul Selvan6, Chaitra Patil7, Sneh Kalgotra8
1 Senior Lecturer, Department of Public Health Dentistry, Maharaja Ganga Singh Dental College and Research Centre, Sri Ganganagar, Rajasthan, India.
2 Reader, Department of Public Health Dentistry, Royal Dental College and Hospital, Palakkad, Kerala, India.
3 Professor and HOD, Department of Public Health Dentistry, Narsinhbhai Patel Dental College and Hospital, Visnagar, Gujarat, India.
4 Postgraduate Student, Department of Orthodontics and Dentofacial Orthopedics, Annasaheb Chudaman Patil Memorial Dental College, Dhule, Maharashtra, India.
5 Senior Lecturer, Department of Public Health Dentistry, Sharad Pawar Dental Colllege, Wardha, Maharashtra, India.
6 Professor and HOD, Department of Microbiology, Krishnadevaraya College of Dental Sciences, Bengaluru, Karnataka, India.
7 Senior Lecturer, Department of Oral and Maxillofacial Surgery, Krishnadevaraya College of Dental Sciences, Bengaluru, Karnataka, India.
8 Registrar, Department of Orthodontics and Dentofacial Orthopedics, Government Dental College and Hospital, Srinagar, Jammu and Kashmir, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Romshi Raina, H. No. 149/C, Wazir Bagh, Surya Vihar, Patta Bohri, Tallab Tillo, Jammu Tawi-180002, Jammu and Kashmir, India.
E-mail: romshi.raina@gmail.com
Introduction
Miswak (Salvadora persica) is a tooth cleaning stick made from the Salvodora Persica tree. It serves as a natural dentifrice with anti-bacterial, anti-plaque and anti-fungal properties. Fluoride, impregnated in chewing sticks will bestow comparable safety against dental caries as the fluoride containing dentifrice.
Aim
The aim of the present study was to assess and compare the anti-bacterial effect of 0.5% sodium fluoride impregnated miswak and plain miswak sticks on Streptococcus mutans.
Materials and Methods
A randomized controlled concurrent parallel triple blind clinical trial was conducted for a period of 8 days. The trial included 30 subjects aged 20–23 years, who were randomly allocated in 1:1 ratio to Group A [0.5% Sodium Fluoride (NaF) impregnated Miswak sticks) and Group B (Plain Miswak sticks) respectively. The participants were instructed to chew miswak sticks for 6 minutes in the morning before breakfast. Unstimulated saliva was collected at baseline and after chewing miswak sticks to estimate S. mutans count using Mitis Salivarius Bacitracin agar. Data was statistically analyzed using paired and unpaired t-test.
Results
A statistically significant reduction in S. mutans Colony Forming Units (CFU) count in saliva was observed after using fluoridated miswak sticks compared to the baseline count (p=0.001). There was no significant difference in anti-bacterial effect of fluoridated miswak sticks and plain miswak sticks on S. mutans count (p=0.58).
Conclusion
The efficacy of miswak impregnated with 0.5% NaF and plain miskaw sticks in reducing S. mutans counts in saliva is analogous.
Dental caries, Mitis salivarus agar, Natural toothbrush, Oral self care, Salvadora persica
Introduction
Oral health has a major influence on one’s general quality of life and well-being. Several chronic and systemic diseases have been attributed to poor oral health [1]. Poor oral hygiene due to lack of proper knowledge of dental care has led to increased prevalence of dental caries around the world [2]. This increased global burden of oral disease has led to the surge for prudent, effective and cost–effective alternate prevention modalities [1].
In developing countries where dental care facilities are out of reach for most of the population, there is a need for health education and to promote traditional means of oral hygiene maintenance [2]. Oral hygiene methods have been practiced worldwide since olden times. These measures have been adapted in some populations depending on factors, like educational level, cultural background, religious norms and as well as socio-economic status [3]. The widely used methods for maintaining oral health are toothbrushes and dentifrices. Babylonians in 3500 BC are considered as the forerunners of the modern day toothbrushes and toothpicks [4].
In spite of global practice of toothbrush and paste, for developing countries like India these are still a luxury and majority of people have access only to the local home grown oral hygiene aids [4]. Rural population of India which accounts to about 80% of the total population still use datun (chewing stick) to clean their teeth [5]. In India, there are at least six different varieties of datun which are in use viz., Neem (Azadirachta-indica), Babul (Vachellia-nilotica), Mango (Mangifera-indica), Guava (Psidium-guajava) and Dandarasa [6].
Miswak, belongs to the Salvadora species of Salvadoracea family. Scientifically known as Salvadora persica, it is anti-bacterial, anti-caries, anti-periopathic disinfectant having anti-plaque and anti-fungal properties. In indian subcontinent it is also called by the names like Arak tree, Meswak, Peelu, Kharjal or Jhank [7].
According to World Health Organisation (WHO) Consensus Report on Oral Hygiene, chewing sticks could play a pivotal role in the oral health promotion as they are traditionally acceptable, economical and easily accessible [8,9].
Invention of fluoride therapy played a major role in caries preventive strategies over five decades [10]. Topical fluoridation is the most commonly utilized method by which fluoride products are directly applied to the tooth surfaces either in the clinic or at home; this treatment modality has shown reduction in caries prevalence to about 30% [11]. Fluoride dentifrice is the commonest form of topical fluoride used worldwide [12]. The benefit of fluoride in reducing caries experience is throughout life [13]. Although dentifrices are widely used in the world, in developing countries, its use is limited among people, especially rural population because of their cost and compliance issues [14]. This problem can be overcome by fluoridating indigenous oral hygiene aids like miswak. Fluoride if present in chewing sticks will confer similar protection against dental caries as fluoride dentifrice. However, there is limited scientific information on anti-bacterial property of fluoridated miswak.
Thus, the present study was conducted to test the hypothesis that there is no difference in the anti-bacterial effect of plain and 0.5% Sodium Fluoride (NaF) impregnated miswak against Streptococcus mutans.
Materials and Methods
A randomized controlled concurrent parallel triple blind clinical trial was conducted in the Department of Public Health Dentistry, Krishnadevaraya College of Dental Sciences and Hospital, Bengaluru, Karnataka, India. The sample was drawn through non-probability sampling technique. The sample size of 30 subjects was selected based upon an earlier study by Yavagal PC et al., [15]. Subjects, aged between 20-23 years, who fulfilled the following eligibility criteria, were selected from the Krishnadevaraya College of Dental Sciences and Hospital.
Inclusion Criteria:
Subjects in the age group of 20–23 years
Healthy non-smokers
Subjects with good manual dexterity
Exclusion Criteria:
Systemically compromised
Subjects undergoing orthodontic treatment
Subjects under antibiotic therapy or using anti-microbial mouthwash for past one week.
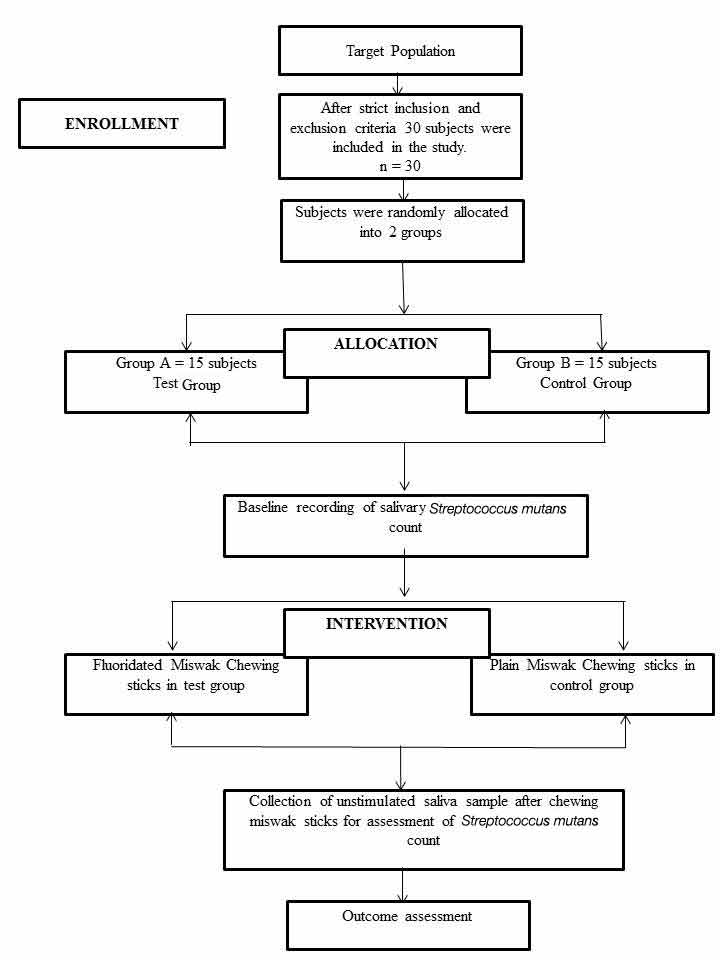
These students were randomly assigned using lottery method into two groups with 15 in each group (Group A and Group B) [Table/Fig-1]. Study participants were refrained from eating or drinking two hours before using miswak sticks to standardize the saliva collection technique. Informed consent was taken from the participants and ethical clearance was obtained from the institutional ethical committee.
Flow diagram of study protocol according to CONSORT.
In the trial, all the three i.e., the primary investigator, study subjects and the trial statistician were unaware of the study details.
Intervention Procedure
Collection of miswak sticks: Fresh miswak sticks were purchased from the local market. Fifteen sticks were randomly selected and it was made sure that they resemble in their size, diameter and colour. Each miswak stick was cut into two equal parts using a scalpel. One part was used as plain miswak and the other part was impregnated with 0.5% NaF. The sticks were then coded by an independent investigator who was not aware of the study method and grouping. NaF impregnated miswak sticks were coded as A (A1, A2….A15) while plain miswak sticks were coded as B (B1, B2…B15).
Preparation of fluoridated miswak sticks: The miswak sticks were then placed in a sterile bottle containing 500ml of 0.5% NaF solution for a day. After impregnation, the miswak sticks were removed from the bottle using forceps and placed on a filter paper at room temperature overnight for 12 hours in order to dry.
Collection of Saliva Sample
Baseline sample: All the study participants were instructed to expectorate 2ml of unstimulated saliva in a sterile container.
Intervention (chewing miswak): The study participants were asked to peel off the bark of the Miswak stick to about half an inch from the tip and then chew the tip gently until it becomes like a brush. They were instructed to move the Miswak stick around the dentition for six minutes.
Test sample: After the intervention (chewing miswak sticks) the study participants were instructed not to swallow the saliva but to spit 2ml of unstimulated saliva in the sterile container. The sterile containers were coded and sent for the microbiological analysis.
Microbiological assessment: The saliva sample was vortexed in the vortex mixer (REMI M101) for one minute. A 100μl of the sample was transferred to 9.9ml of sterile Brain Heart Infusion Agar (BHA) broth and vortexed again for one minute. The 100μl of the diluted sample was transferred to a sterile Mitis Salivarius Bacitracin Agar (HI MEDIA, Mumbai) and spread uniformly using a sterile L spreader (TARSONS, Kolkata). Inoculated culture media were incubated at 37°C in a candle extinction jar for 48 hours. The colonies on the agar plate were observed. Small convex deep blue colonies were further studied by gram stain and identification tests. S. mutans were identified by gram stain morphology of gram positive cocci occurring in chains. They were confirmed by a positive mannitol and sorbitol fermentation. The colonies were counted using a digital colony counter (LABTRONICS) and the Colony Forming Unit per ml (CFU/ml) of the saliva sample was calculated.
Debriefing: At the end of the study the details regarding group allocation and results were disclosed to the study subjects.
Statistical Analysis
The data was analyzed using SPSS (Statistical Package for Social Sciences) software version 20.1. The significance level was fixed at 5%. Frequency distribution, mean, and Standard Deviation (SD) were generated. Paired t-test (two-tailed, dependent) was used to compare the mean differences at the baseline and after the intervention within each group. Unpaired t-test (two-tailed, independent) was used for comparison of mean difference in S. mutans between the groups (NaF impregnated miswak sticks group and plain miswak sticks group).
Results
The Group-A, fluoridated miswak group, consisted of total 6 male (40%) and 9 female subjects (60%), and the Group B, plain miswak stick group, had 5 male (33.3%) and 10 female subjects (66.7%) study. The mean age of the study participants in Group A and Group B was 21.47±1.25 and 21.53±1.25 respectively.
[Table/Fig-2] shows the difference in S. mutans count of each group before and after chewing miswak sticks. A statistically significant reduction in S. mutans count was observed after using fluoridated miswak sticks (Group A) as compared to the baseline count (p<0.001). Similarly in Group B (plain miswak sticks), the decrease in mean S. mutans count from before chewing to after chewing miswak sticks was found to be statistically significant (p<0.001). It was observed that there was no statistically significant difference in the mean of S. mutans counts (CFU/ml x 103) between the two groups (p>0.05) [Table/Fig-3].
Comparison of S. mutans counts (CFU/ml x 103) within the group pre- and post- chewing miswak stick.
| Group | ChewingMiswak | Mean S. mutans Count(Mean±SD) | Mean Difference(Mean±SD) | 95% CIof theDifference | t-value | p-value |
|---|
| Group A(NaF impregnated Miswak)n=15 | Before | 932.33±455.64 | 508.40±369.39 | 303.84-712.96 | 5.330 | 0.001 |
| After | 423.93±230.32 |
| Group B(Plain Miswak)n=15 | Before | 901.47±377.02 | 417.60±250.45 | 278.91-556.29 | 6.458 | 0.001 |
| After | 483.87±339.40 |
Statistical test applied: Paired t test
Comparison of S. mutans counts (CFU/ml x 103) between the two groups.
| Chewing Miswak | Group | Mean S. mutans Count(Mean±SD) | M.D. | 95% CI of the Difference | Levene’s Test for Equality of Variances | t-value | p-value |
|---|
| Lower | Upper | F | Sig. |
|---|
| Before | Group A | 932.33±455.64 | 30.86 | -281.92 | 343.66 | 0.280 | 0.601 | 0.202 | 0.841 |
| Group B | 901.47±377.02 | | | | | |
| After | Group A | 423.93±230.32 | -59.93 | -276.87 | 157.01 | 0.955 | 0.337 | -0.566 | 0.576 |
| Group B | 483.87±339.40 | | | | | |
Statistical Test applied: Unpaired t test
Discussion
This study was based on the concept that chewing sticks are frequently utilized in many countries including India, for cleaning purposes and are often used up to 5 times/day. The idea of fluoridating Miswak chewing sticks in order to have a dual effect, combining the mechanical cleaning and the anti-cariogenic effect achieved through fluoride release into the oral cavity allures scientific research.
As this is an in-vivo study, it was important to fix the NaF solution at a safer concentration. In the current research work Miswak sticks were impregnated with 0.5% NaF were utilized. Baeshan H and Birkhed D considered this to be safe and effective in their study, where different concentrations of NaF were used to impregnate Miswak sticks [16].
S. mutans strains were considered in the study as they are most commonly implicated microorganisms in the causation of dental caries [17]. Mitis Salivarius Bacitracin agar was used for inoculation of S. mutans as it is considered to be a standard media to be used for respective strains [18].
The results of the present clinical study indicate that 0.5% NaF impregnated miswak was as effective as plain miswak chewing sticks in reducing the S. mutans count in saliva. There are very few studies that report on the anti-bacterial efficacy of fluoridated Miswak chewing sticks. A randomized controlled trial conducted by Yavagal PC et al., in 2014 showed a significant decline in salivary S. mutans count but not in salivary Lactobacilli count [15].
A study by Bhat PK et al., using miswak extract rinse reported a significant reduction in both S. mutans and Lactobacilli count [19].
Another study by Almas K et al., showed similar results where significant reduction in S.mutans counts was observed after using miswak extract mouthrinse [20].
Limitation
This study is confined by certain limitations. The smaller sample-size and the influence of oral hygiene practices and dietary habits on the study results cannot be ignored. Albeit it can be recommended that NaF impregnated miswak stick may offer itself as an affordable and effective oral hygiene aid and can be used as an effective vehicle for fluoride delivery in countries where Miswak use is common or a tradition.
Conclusion
Sodium fluoride impregnated miswak sticks were able to reduce the S. mutans counts as effectively as plain Miswak sticks.
The public health aspect of this study is that fluoridated miswak chewing sticks may have a great role in community oral health programmes, for the prevention of caries in rural areas especially in communities which do not have access to community water supply, where water fluoridation and fluoride supplement programmes are not feasible. The use of miswak conforms not only to the subject of primary healthcare approach, but also to certain cultural, long-established, societal, and religious beliefs. Use of fluoridated miswak into the healthcare system will significantly help the masses with financial constraints, as well as limited oral health care facilities. Further research on the role of fluoridated miswaks as a preventive medicament should be conducted in large populations for example school children.
Statistical test applied: Paired t test
Statistical Test applied: Unpaired t test
[1]. Halawany HS, A review on miswak (Salvadora persica) and its effect on various aspects of oral healthSaudi Dent J 2012 24:63-69. [Google Scholar]
[2]. Naseem S, Hashmi K, Fasih F, Sharafat S, Khanani R, In vitro evaluation of antimicrobial effect of miswak against common oral pathogensPak J Med Sci 2014 30(2):398-403. [Google Scholar]
[3]. Asadi SG, Asadi ZG, Chewing sticks and the oral hygiene habits of the adult Pakistani populationInt Dent J 1997 47:275-78. [Google Scholar]
[4]. Wu CD, Darout IA, Skang N, Chewing sticks: Timeless natural toothbrushes for oral cleansingJ Periodont Res 2001 36:275-84. [Google Scholar]
[5]. Johri M, Neem: Rightly called the ‘village pharmacy’IST 2007 15:42:27 [Google Scholar]
[6]. Bhambal A, Kothari S, Saxena S, Jain M, Comparative effect of neemstick and toothbrush on plaque removal and gingival health – A clinical trialJ Adv Oral Res 2011 2(3):51-56. [Google Scholar]
[7]. Chaurasia A, Patil R, Nagar A, Miswak in oral cavity: An updateJ Oral Biol Craniofac Res 2013 3:98-101. [Google Scholar]
[8]. WHO. Prevention methods and programmes for oral diseases. World Health Organization Technical Report Series 713. Geneva 1984 [Google Scholar]
[9]. WHOConcensus statement on oral hygieneInt Dent J 2000 50:139 [Google Scholar]
[10]. Centre for Desease Control. Recommendation for using flouride to protect and control dental caries in the United State. CDC. USA, 2001; 1-42. Available from: http://www.cdc.gov/mmwr /preview/mmwrhtm/rr5014al.htm. Accessed on: 05 September 2014 [Google Scholar]
[11]. Murray JJ, Nunn JH, Steele JG, The prevention of oral diseases 2003 4th EditionNew YorkOxford University Press [Google Scholar]
[12]. Bratthall D, Peterson GH, Sundberg H, Reasons for the caries decline. What do the experts believe?Euro J Oral Sci 1996 104:416-22. [Google Scholar]
[13]. Griffin SO, Regnier E, Griffin PM, Huntley SO, Effectiveness of fluoride in preventing caries in adultsJ Dent Res 2007 86(5):410-15. [Google Scholar]
[14]. Tewari A, Fluoride and dental cariesJ Indian Dent Assoc 1986 1:5-12. [Google Scholar]
[15]. Yavagal PC, Kumbhar S, Nagesh L, Kulkarni A, Antimicrobial effect of miswak sticks and 0.5% sodium fluoride impregnated miswak sticks on Streptococcus mutans and lactobacilli - A randomized controlled trialUnique J Med Dent Sci 2014 2(2):79-82. [Google Scholar]
[16]. Baeshan H, Birkhed D, Release of fluoride from fresh and old NaF impregnated chewing sticks (miswaks) in vitro and oral retention in vivoOral Health Prev Dent 2010 8:93-99. [Google Scholar]
[17]. Nishikawara F, Katsumura S, Ando A, Tamaki Y, Nakamura Y, Sato K, Correlation of cariogenic bacteria and dental caries in adultsJ Oral Sci 2006 48(4):245-51. [Google Scholar]
[18]. Ananthnarayan CK, Panniker J, Textbook of microbiology 2009 8th EditionHyderabadUniversities Press [Google Scholar]
[19]. Bhat PK, Kumar A, Sarkar S, Assessment of immediate antimicrobial effect of miswak extract and toothbrush on cariogenic bacteria – A clinical studyJ Adv Oral Res 2012 3(1):13-18. [Google Scholar]
[20]. Almas K, Al-Zeid Z, The immediate effect of a toothbrush and miswak on cariogenic bacteria: A clinical studyJ Contemp Dent Pract 2004 5(1):105-14. [Google Scholar]