Talon cusp is a rare developmental anomaly presenting as a wisp like structure arising from the cervical region of anterior teeth. They are predominantly seen in permanent dentition with a male predilection and are commonly seen associated with incisors and on the lingual/palatal surface. The aetiology appears to be multifactorial with a possible likelihood of genetic and environmental involvement routing to disturbances in tooth development at the morphodifferentiation stage. Over the years, few cases of talon cusp among the family members have been reported which strongly supports the genetic influence. We report rare presentations of talon cusp among two family members involving the facial surface of incisors.
Eagle, Incisors, Labial, Siblings, Tooth anomaly
Case Report
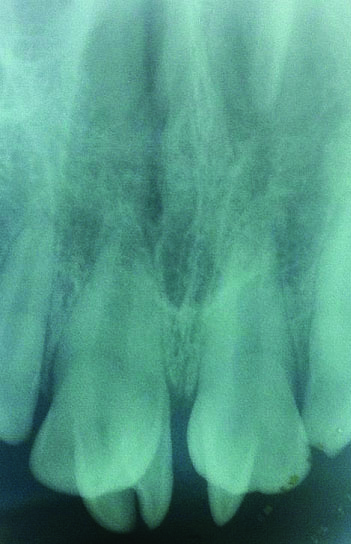
An 8-year-old female patient accompanied by her mother reported to dental out patient department with a complaint of malformed upper front teeth. This was her first visit to the dentist. She did not present any significant medical history. Family history suggested that her father also has similar presentation of upper front teeth. Extraoral examination did not show any abnormalities. Intraoral examination showed a fair oral hygiene with decayed upper right and left second deciduous molars. The maxillary right central incisors were displaced medially and palatally with accessory cusps (three on maxillary right incisor and one on maxillary left incisor) noted on the facial aspect. The cusps were well defined, perpendicularly localized to the mesiodistal plane of the crown and completely attached to it. They projected from the Cemento Enamel Junction (CEJ) and curved toward the incisal edge of the incisor. The cusps were conical/bud shaped and were equal in size except for the one on the middle of the maxillary right central incisor which was 3/4th of the size of the other accessory cusps. Prominent developmental grooves were observed between the accessory cusp and labial surface of the crown [Table/Fig-1,2]. There was no clinical evidence of caries; periodontal pockets, tenderness to percussion and no associated soft tissue changes. The thermal vitality test revealed normal pulp response. Periapical radiograph revealed presence of V-shaped/loop like radio opaque structures superimposed over the maxillary right and left central incisor. The internal structure had differential densities resembling enamel, dentin and pulp; all the features were suggestive of facial talon cusp [Table/Fig-3].
Talon cusp on teeth #11, 21 (facial view) of case 1- daughter.

Talon cusp on teeth #11, 21 (incisal view) of case 1- daughter.

Intra-oral periapical radiograph showing the talon cusp of case 1- daughter.
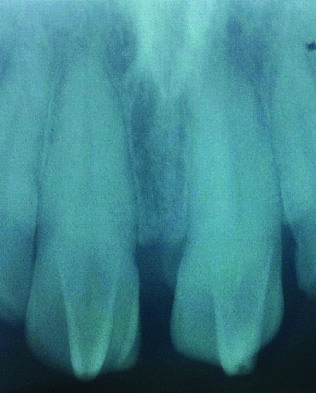
In the subsequent follow up visit, patient’s father was examined and found to have a prominent horn like accessory cusps on the facial aspect of maxillary central incisors. There were two accessory cusps on maxillary right central incisor and one on maxillary left central incisors. The cusps extended from the CEJ towards the incisal edge along the medial plane of the crown. The presentation of the cusp was similar to that of his daughter’s accessory cusp with regard to shape, extent and other clinical and radiographic findings. Additionally, a notched depression was also noted on the middle third on both the accessory cusp which was suggestive of abrasion [Table/Fig-4,5 and 6]. Both the patients were planned for periodic and gradual reduction of the cusp with topical fluoride application and composite resin facing. Unfortunately, the patients refused to undergo treatment. However, they were cautioned about the consequences and advised to report if symptomatic.
Talon cusp on teeth #11, 21 (facial view) of case 2- father.

Talon cusp on teeth #11,21 (incisal view) of case 2- father.

Intra oral periapical radiograph showing the talon cusp of case 2- father.
Discussion
Talon cusp was first recognized by Mitchell in 1892, Ripa and Mellor later coined the term “talon” due to its resemblance to eagle’s talon when viewed from the occlusal edge [1,2]. Over the years, talon cusp has been designated with various terms such as hyperplastic cingulum, horn, cusped cingulum, dens evaginatus, supernumerary cusp, supernumerary lingual tubercle, evaginated odontome, “T” tooth and accessory cusp [3]. The conventional definition of talon cusp considers them as an accessory cusp projecting palatally/lingually from the cingulum to the incisal edge. However, the current definition extends to include talon cusp as an accessory cusp on the palatal/lingual and facial/labial aspect of incisors or canines. In the past, only few cases of facial talon cusp have been reported [Table/Fig-7] [3–25]. The present report is one among the few rare presentation of talon cusp on the facial aspect of the mandibular central incisor and more interestingly, it was noted among two family members.
Data of facial talon cusp reported.
| Author name | No. of teeth with facial talon cusp | FDI notation tooth no’s |
|---|
| Abbott PV et al., [4] | 1 | 13 |
| Chinni SK et al., [5] | 3 | 11,21, 43 |
| Chinni SK et al., [5] | 1 | 21 |
| Chinni SK et al., [5] | 2 | 11, 21 |
| Cubukcu CE et al., [6] | 1 | 12 |
| De sousa SN et al., [7] | 1 | 22 |
| Dunn WJ et al., [8] | 1 | 12 |
| Ekambram ML et al., [9] | 1 | 12 |
| Goswami S et al., [10] | 1 | 42 |
| Jowharji N et al., [11] | 1 | 11 |
| Kulkarni VK et al., [12] | 2 | 41, 42 |
| Lee C et al., [13] | 1 | 11 |
| Lee C et al., [13] | 2 | 31,41 |
| Llena Puy MC and Forner NL [14] | 1 | 31 |
| Ma MS et al., [15] | 1 | 11 |
| Mayes AT et al., [16] | 1 | 11 |
| Mckaig SJ and Shaw L [17] | 1 | 11 |
| Mc Namara T et al., [18] | 1 | 31 |
| Patil R et al., [19] | 1 | 21 |
| Patil K et al., [3] | 1 | 21 |
| Shashikiran ND et al., [20] | 1 | 21 |
| Stojanowski CM and Johnson KM [21] | 1 | 21 |
| Sumer AP and Zengin AZ [22] | 1 | 21 |
| Thakur S et al., [23] | 1 | 13 |
| Tsusumi T and Oguchi H [24] | 1 | 21 |
| Turner CG et al., [25] | 1 | 21 |
The aetiology of talon cusp is not clearly known. However, it is believed that genetic influence, developmental defect, intrauterine environmental disturbances, systemic disorders, nutritional deficiencies, trauma and other factors, especially in prenatal period can clearly influence tooth environmental conditions and lead to this anomaly. Regardless of the aetiology, the pathogenesis begins during the morphodifferentiation stage of tooth development. It may occur as a result of outward/upward folding of inner enamel epithelial cells (precursors of ameloblast) and transient focal hyperplasia of the peripheral cells of mesenchymal dental papilla (precursors of odontoblast) [3,10,23]. Others opine that the formation of talon cusp is purely due to a genetically determined hyper productivity of the anterior ends of dental lamina. Other factors that favour genetic aetiology include presence of this anomaly in siblings and member of the same family, in twins, in patients from consanguineous marriages, and some genetic syndromes. Thus, it can be considered that talon cusp can originate as a result of the interaction of genetic and environmental factors.
The prevalence of talon cusp varies widely in different population groups (0.6%to7.7%). [23,26]. Prevalence of talon cusps in Indian population ranges from 1% to 8% [26]. Talon cusps are more commonly associated with the permanent lateral incisor [12,21,27]. In case of deciduous dentition, it is most commonly seen with the maxillary central incisor. Few cases of facial talon cusp involving the permanent maxillary canines have also been reported [5,23]. Amongst gender, in contrast to the palatal talon, the facial talon cusp has a higher predilection for females [12].
Talon cusps are usually seen on the palatal/lingual surface of the teeth [28,29]. They are rarely seen on the facial/labial surface, as seen in the present case. The appearance of talon cusp on the labial surface of the tooth can be attributed to the hyperplasia of labial central developmental lobe. Regardless of its location, the presentation can vary in shape, size, structure, location, and site of origin. The cusps can be sharp and spiked or rounded with smooth tips. The tooth associated with talon cusp can have a T-form or a Y-shaped crown, the cusps can be conical, bud like, pyramidal or horn shaped [3]. Co-occurrence of talon cusps with other dental anomalies such as supernumery teeth, shovel-shaped maxillary incisors, cusps of Carabelli, dens invaginatus, odontome, fusion, gemination, impacted teeth, Bifid cingula, double teeth, enamel clefts and distorted nasal alae have also been reported [3,23,30]. Our cases did not have any other anomalies and Talon cusps were the only isolated dental anomaly.
Over the years, talon cusps were found in association with various common syndromes such as Rubinstein–Tyabi syndrome, Sturge–Weber syndrome, Ellis-van Creveld syndrome. Few were also seen in association with Mohr syndrome, Berardinelli-Seip syndrome and Allagille’s syndrome [3,10,23]. An unusual case of talon cusp associated with incontinentia pigmenti achromians has also been reported [24]. Our cases did not have any findings representing any syndromes or any medical conditions.
The clinical problems associated with talon cusp include unpleasant aesthetic appearance, displacement of teeth, occlusal interface, plaque retention, caries, cuspal fracture, pulp exposure, periodontal disease and irritation of the soft tissues during speech or mastication [10]. Radiographically, talon cusp can appear as a V-shaped or loop like structure with differential densities suggestive of enamel, dentin and pulp.
Management of talon cusp varies depending on the size of the cusp, presence or absence of pulp horn, the degree of occlusal interferences, aesthetic problems, soft tissue irritation, interference with the tongue space and pulpal involvement. Conservatively, gradual grinding of talon cusps over weeks and then the application of a desensitizing agent to avoid possible dentinal sensitivity and pulpal exposure have been tried. The other treatment modalities are placement of pit- and- fissure sealants or restorations, root canal therapy (in case of pulpal involvement) and extractions (in severely destructed cases) [10,23].
Conclusion
Labial talon cusp is an unusual dental finding, often associated with other anomalies and genetic syndromes. Isolated labial talon as seen in our cases involving two generations is an extreme rarity. This mandates the diagnostician to have adequate knowledge and perform a thorough examination to rule out coexisting morbidities. Considering the complications associated with it, early diagnosis and treatment can play a vital role in recuperating aesthetics.
[1]. Mitchell WH, Case report 1892 34Dental Cosmos:1036 [Google Scholar]
[2]. Mellor JK, Ripa LW, Talon cusp: A clinically significant anomalyOral Surg Oral Med Oral Pathol 1970 29:225-28. [Google Scholar]
[3]. Patil K, VG Mahima, Shreenivas S, “T” Tooth: A sporadic labial talonInternational journal of dental sciences and research 2015 3(1):13-16. [Google Scholar]
[4]. Abbott PV, Labial and palatal “talon cusps” on the same tooth: A case reportOral Surg Oral Med Oral Pathol Oral Radiol Endod 1998 85:726-30. [Google Scholar]
[5]. Chinni SK, Nanneboyina M, Ramachandra A, Chalapathikumar H, A facial talon cusp on maxillary permanent central incisorsJ Conserv Dent 2012 15:87-88. [Google Scholar]
[6]. Cubukcu CE, Sonmez A, Gultekin V, Labial and palatal talon cusps on geminated tooth associated with dental root shape abnormality: A case reportJ Clin Pediatr Dent 2006 31:21-24. [Google Scholar]
[7]. De Sousa SM, Tavano SM, Bramante CM, Unusual case of bilateral talon cusp associated with dens invaginatusInt Endod J 1999 32:494-98. [Google Scholar]
[8]. Dunn WJ, Unusual case of labial and lingual talon cuspsMil Med 2004 169:108-10. [Google Scholar]
[9]. Ekambaram M, Yiu CK, King NM, An unusual case of double teeth with facial and lingual talon cuspsOral Surg Oral Med Oral Pathol Oral Radiol Endod 2008 105:63-67. [Google Scholar]
[10]. Goswami S, Mitra M, Saha S, Halder S, A case of fused teeth with facial and lingual talon cusps in the mandibular anterior region: A case reportArch Med Health Sci 2016 4:75-77. [Google Scholar]
[11]. Jowharji N, Noonan RG, Tylka JA, An unusual case of dental anomaly. A “facial” talon cuspJ Dent Child 1992 59:15-18. [Google Scholar]
[12]. Kulkarni VK, Choudhary P, Bansal AV, Deshmukh J, Duddu MK, Shashikiran ND, Facial talon cusp: A rarity, report of a case with one year follow up and flashback on reported casesContemp Clin Dent 2012 3:125-29. [Google Scholar]
[13]. Lee C, Burnett SE, Turner CG, Examination of the rare labial talon cusp on human anterior teethDent Anthropol 2003 16:81-83. [Google Scholar]
[14]. Llena Puy MC, Forner Navarro L, An unusual morphological anomaly in an incisor crown. Anterior dens invaginatusMed Oral Patol Oral Cir Bucal 2005 10:13-16. [Google Scholar]
[15]. Ma MS, Facial talon cusp: A case reportInt Poster J Dent Oral Med 2006 8:726-30. [Google Scholar]
[16]. Mayes AT, Labial talon cusp: A case study of pre European contact American IndiansJ Am Dent Assoc 2007 138:515-18. [Google Scholar]
[17]. Mckaig SJ, Shaw L, Dens avaginatus on the labial surface of a central incisor: A case reportDent Update 2001 28:210-12. [Google Scholar]
[18]. McNamara T, Haeussler AM, Keane J, Facial talon cuspInt J Pediatr Dent 1997 7:259-62. [Google Scholar]
[19]. Patil R, Singh S, Subba Reddy VV, Labial talon cusp on permanent central incisor: A case reportJ Indian Soc Pedod Prev Dent 2004 22:30-32. [Google Scholar]
[20]. Shashikiran ND, Babaji P, Reddy VV, Double facial and lingual trace talon cusps: A case reportJ Indian Soc Pedod Prev Dent 2005 23:89-91. [Google Scholar]
[21]. Stojanowski CM, Johnson KM, Labial canine talon cusp from the early holocene site of Gobero, central Sahara Desert, NigerInt J Osteoarchaeol 2011 21:391-406. [Google Scholar]
[22]. Sumer AP, Zengin AZ, An unusual presentation of talon cusp: A case reportBr Dent J 2005 199:429-30. [Google Scholar]
[23]. Thakur S, Gupta R, Thakur NS, Gupta M, Facial talon cusp on permanent maxillary canine: A rare dental anomalyEur J Gen Dent 2013 2:324-27. [Google Scholar]
[24]. Tsusumi T, Oguchi H, Labial talon cusp in a child with incontinentia pigmenti achromians: Case reportPediatr Dent 1991 13:236-37. [Google Scholar]
[25]. Turner CG, Another talon cusp: What does it mean? Dent Anthropol 1998 12:10-12. [Google Scholar]
[26]. Safadi RA, Hamasha AH, Prevalence of talon cusps in Jordanian permanent teeth: A radiographic studyBMC Oral Health 2010 10:16 [Google Scholar]
[27]. Hegde KV, Poonancha KS, Sujan SG, Bilateral labial talon cusps on permanent maxillary central incisors: Report of a rare caseActa Stomatol Croat 2010 44:120-22. [Google Scholar]
[28]. Gupta S, Tandon A, Chandra A, Gupta OP, Syndontia with talon cuspJ Oral Maxillofac Pathol 2012 16:266-71. [Google Scholar]
[29]. Rao PK, Mascarenhas R, Shetty SR, Facial talon in mandibular incisor: An unusual occurrenceDent Res J (Isfahan) 2011 8:229-31. [Google Scholar]
[30]. Balcioglu HA, Keklikoglu N, Kökten G, Talon cusp: A morphological dental anomalyRom J Morphol Embryol 2011 52:179-81. [Google Scholar]