Dental plaque is a tooth associated biofilm which plays an important role in the causation of dental caries. The cariogenic organisms such as Streptococcus mutans, Streptococcus sanguis, Streptococcus salivarius, Streptococcus mitis, Streptococcus oralis and Lactobacillus acidophilus play a vital role in the aetiology of the caries. The growth of these organisms would have a profound influence on the initiation and progression of disease [6]. Conventional anticariogenic agents are although numerous, majority of them are known to have side effects such as multiple drug resistance [1]. Herbal medicine has gained importance in the field of dentistry due to its minimal adverse effects on the oral tissue and is, as effective as the conventional anticariogenic agents [7]. World Health Organisation (WHO) proposed that, any medicinal herb has to go through various scientific studies to establish the potential for its therapeutic use [8]. The purpose of this study was to find the antimicrobial properties of mangosteen pericarp on cariogenic organisms by measuring the zones of inhibition. The MIC of the mangosteen extracts was also estimated to find out the minimal concentration at which the mangosteen pericarp will inhibit the growth of the bacteria. MBC was also estimated to identify the bacterial lysis. MBC is the lowest concentration at which 99.99% of the bacteria analyzed, show lysis [9]. These would open up newer avenues in using mangosteen as an antibacterial agent.
Materials and Methods
The cross-sectional in vitro study was performed in Central Research Laboratory, Meenakshi Ammal Dental College and Research Institute, Chennai, Tamil Nadu, India for a period of eight weeks. The institutional ethical committee and Institutional Review Board, MAHER University approved the study. (MAHER-MU-004-IEC/2016)
Test Organisms used for the Study
Standard strains of the microorganisms Streptococcus oralis MTCC 2696 Streptococcus mutans MTCC no. 890, Lactobacillus acidophilus MTCC no. 10307, Streptococcus salivarius ATCC no. 13419 and Streptococcus sanguis ATCC no. 10556 for the study were procured from MTCC and ATCC.
Crude Solvent Extraction
The pericarp was extracted from the fruit of Garcinia mangostana by drying in shade and then powdered. The resulting powder was then stored in air tight wide mouth containers. The crude extract of mangosteen pericarp powder was prepared using an organic solvent, chloroform at room temperature. Almost 25 mg of the mangosteen powder was dissolved in 75 ml of chloroform (1:3 w/v) [10]. The resulting mixture was placed in an orbital shaker for three consecutive days. The solution obtained was then filtered using a whatman filter paper. The filtrate was allowed to evaporate in a rotary evaporator. Almost 100 mg of the crude extract was mixed with 1 ml of Dimethyl Sulphoxide (DMSO) and the product was stored in amber coloured storage containers for further use.
Antibacterial Assay of Mangosteen
The antibacterial effect of the pericarp was tested by using agar well diffusion method [11]. The bacterial inoculums were prepared and were adjusted to 0.5 McFarland turbidity standards [12]. Nearly, 100 μl of the suspension was then streaked uniformly on TSA-BA and MRS agar to form lawn cultures. Three wells were cut on the surface of each culture plate with a sterile borer of 0.5 cm diameter, in all the five plates streaked with the respective organisms. Nearly, 50 μl of pericarp extract was poured into the wells that were seeded with the bacterium to be tested. The plates were then placed at room temperature for an hour, followed by incubation for 24-48 hours at 37°C. The degree of antibacterial activity against tested bacteria was assessed by measuring the diameter of zone of inhibition. The zones of inhibition produced were recorded at the end of 24-48 hours. Chlorhexidine in 0.2% was used as positive control, while DMSO without the test ingredient was taken as a negative control. The test was repeated for each microorganism thrice. The results of the tests were recorded in triplet culture plates.
Determination of Minimum Inhibitory Concentration (MIC) and Minimum Bactericidal Concentration (MBC)
MIC was done by a broth dilution method, where in pure cultures of each microorganisms was grown in their respective broth 1:1 dilutions were made in 96 well microtitre plates [12]. Nearly, 100 μl of the organisms obtained from the logarithmic phase of growth were mixed with 100 μl of the herbal extract. Once diluted, the volume of the diluted herbal extract was added to each dilution wells. The inoculated, serially diluted mangosteen pericarp extract was then incubated for about 24-48 hours at 37°C. The dilution wells were observed for microbial growth indicated by turbidity at the bottom of the well. The final tube devoid of any turbidity determines the MIC of the mangosteen crude extract. The lowest concentration of the extract which causes the lysis of majority of bacteria was recorded as MBC. The turbidity control was the organism with DMSO and the drug turbidity control was drug along with DMSO for determination of MIC and MBC.
Statistical Analysis
Statistical analysis was done by using SPSS Software version 16 for calculating the mean of the zones of inhibition on tested microorganisms. Mann-Whitney test was done to compare the zones of inhibition of mangosteen and 0.2% chlorhexidine.
Results
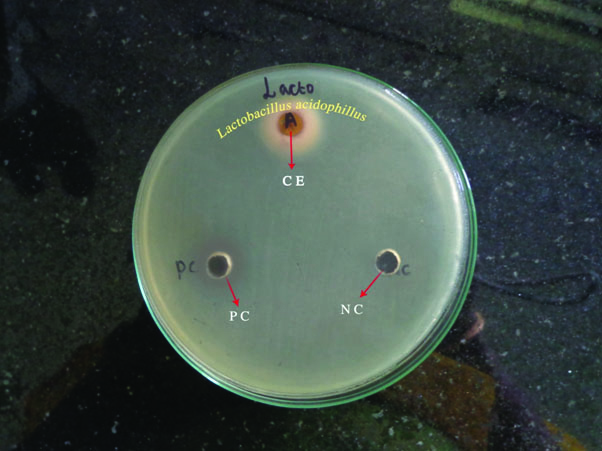
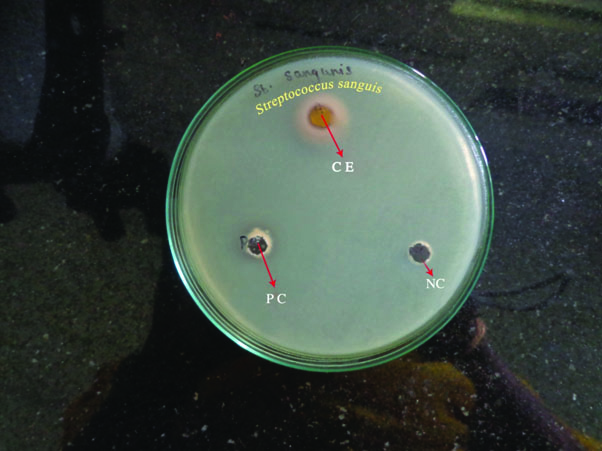
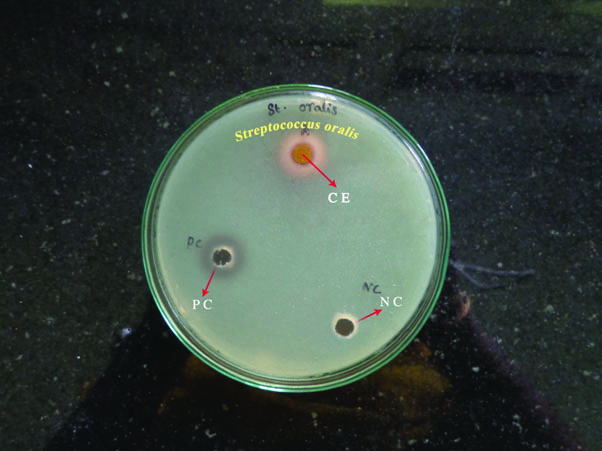
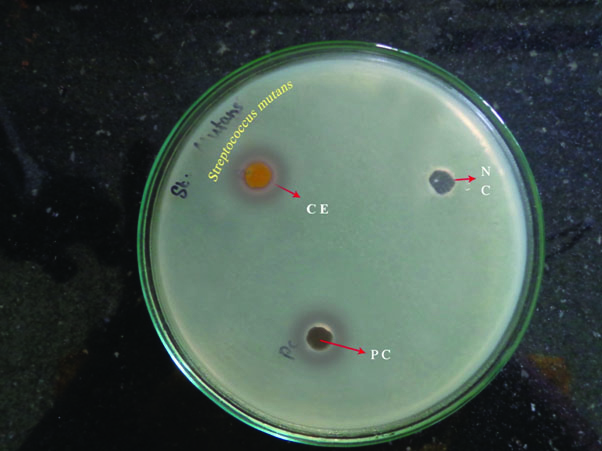
Mangosteen pericarp extract showed a maximum zone of inhibition for Lactobacillus [Table/Fig-1] and Streptococcus sanguis [Table/Fig-2] as compared to Streptococcus oralis [Table/Fig-3], and Streptococcus mutans [Table/Fig-4]. It was least for Streptococcus salivarius [Table/Fig-5]. When compared with standard antiplaque agent such as chlorhexidine at 0.2%, it showed a higher zone of inhibition and was found to be statistically significant [Table/Fig-6]. The MIC and MBC values of the mangosteen pericarp was lowest for Lactobacillus acidophilus (MIC 25 mg/ml, MBC 50 mg/ml) and Streptococcus oralis (MIC 50 mg/ml, MBC 100 mg/ml) compared to the other tested organisms namely Streptococcus mutans, Streptococcus salivarius and Streptococcus sanguis showing the mangosteen pericarp as an effective antibacterial agent at low concentrations [Table/Fig-7].
Antibacterial zones of inhibition produced by chloroform extract of mangosteen against Latobacillus acidophilus.
CE- Chloroform extract of mangosteen, PC- positive control, NC- negative control
Antibacterial zones of inhibition by chloroform extract of mangosteen against Streptococcus sanguis.
CE- Chloroform extract of mangosteen, PC- positive control, NC- negative control
Antibacterial zones of inhibition by chloroform extract of mangosteen against Streptococcus oralis.
CE- Chloroform extract of mangosteen, PC- positive control, NC- negative control
Antibacterial zones of inhibition by chloroform extract of mangosteen against Streptococcus mutans.
CE- Chloroform extract of mangosteen, PC- positive control, NC- negative control
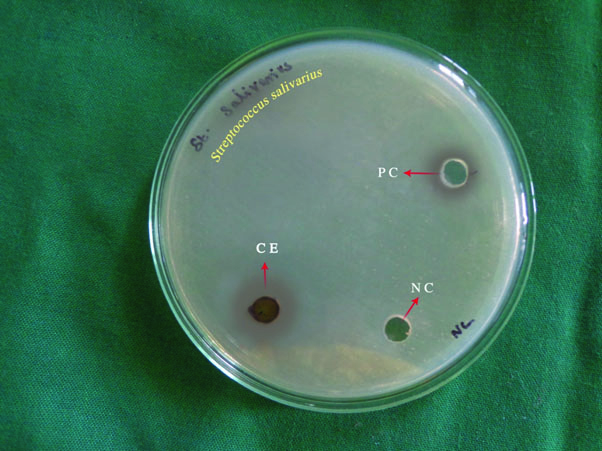
Antibacterial zones of inhibition by chloroform extract of mangosteen against Streptococcus salivarius.
CE- Chloroform extract of mangosteen, PC- positive control, NC- negative control
Mann-Whitney test to compare the effect of Garcinia mangostana pericarp extract and chlorhexidine on oral microorganisms.
| Organism | Group | Mean | Mean Rank | p-value |
|---|
| Streptococcus sanguis | Mangosteen | 13.6 | 3.83 | 0.658 |
| Chlorhexidine | 15 | 3.17 |
| Streptococcus salivarius | Mangosteen | 3 | 2.00 | 0.049* |
| Chlorhexidine | 13 | 5.00 |
| Streptococcus oralis | Mangosteen | 11.3 | 2.00 | 0.046* |
| Chlorhexidine | 13 | 5.00 |
| Streptococcus mutans | Mangosteen | 10.6 | 2.00 | 0.043* |
| Chlorhexidine | 14 | 5.00 |
| Lactobacillus acidophillus | Mangosteen | 13.6 | 2.33 | 0.099 |
| Chlorhexidine | 14 | 4.67 |
*-Significant
Determination of MIC and MBC of Garcinia mangostana on microorganisms.
| Organisms | MIC mg/ml | MBC mg/ml |
|---|
| Streptococcus sanguis | 100 | 200 |
| Streptococcus salivarius | 100 | 200 |
| Streptococcus oralis | 50 | 100 |
| Streptococcus mutans | 100 | 200 |
| Lactobacillus acidophilus | 25 | 50 |
Discussion
Herbal medicine is an inherent part of our ancient culture and is being used in ayurveda and siddha systems of medicine for decades. Currently, a number of herbs are also being used in oral health care. Dental caries is a common microbial disease affecting the tooth predominantly caused by the Streptococcus and Lactobacillus group of bacteria. Since, microorganisms play a key role in the aetiology of this disease, agents impeding the growth of these cariogenic organisms would have a significant role in inhibiting the disease [6]. Today various conventional anticariogenic agents are available, but they have numerous side effects [13].
Herbal medicine has proven to be more promising with respect to antimicrobial activity [14]. The chemotherapeutic property of certain herb derived drugs is capable of restraining the antibiotic resistance as well as the side effects caused by the conventional drugs, leading to a new revolution using these herbal molecules. Thus, the herb derived molecule used as antibacterial therapy is an added advantage to the modern medicine [15,16].
Mangosteen pericarp is an inherent part of this herbal medicine and is widely used in treatment of numerous disorders ranging from, stomach ailments, diarrhoea, and dysentery. It is also being used as an anti-inflammatory, antibacterial and an antifungal agent to treat thrush [4]. It also has an antibacterial property which remains unexplored on oral bacteria [10]. We hypothesize that the mangosteen pericarp extract is as effective as chlorhexidine in inhibiting the growth of the cariogenic organisms grown in vitro. This was determined by evaluating the zones of inhibition produced by the mangosteen pericarp when grown in the presence of the tested microorganisms. For any agent with proven antibacterial effect, the zone of inhibition should be 3 mm or more. Larger the zone, the more effective is the antimicrobial potential [17].
In our study, the majority of the microorganisms showed antimicrobial zones above 3 mm [Table/Fig-6] showing considerable antibacterial inhibitory effect of the pericarp against these microorganisms. The mangosteen extract gave a range of zone of inhibition from 3-13.6 mm at an extract concentration of 100 mg/ml on the tested bacteria. Streptococcus salivarius showed a 3 mm wide zone. The zones of inhibition were compared to standard chlorhexidine at 0.2% [13–15] which gave a comparable range and it was statistically significant for Streptococcus salivarius, Streptococcus mutans and Streptococcus oralis. Similar results have been reported by Linuma et al., who showed that the pericarp extracts of mangosteen had an antibacterial effect on methicillin resistant Staphylococcus aureus [18]. Similarly, Fernando KMEP et al., evaluated the antibacterial activity of methanolic extracts of mangosteen, which showed inhibitory activity on Bacillus subtilis, Staphylococcus aureus and Streptococcus faecalis [19].
The MIC and MBC were lowest for Lactobacillus acidophilus and Streptococcus oralis when compared to the other microorganisms inferring that the mangosteen was effective, even at very low concentration in inhibiting these above organisms among the five tested bacteria [Table/Fig-7]. The results were in agreement with Torrungruang K et al., who showed the similar values for MIC and MBC of mangosteen on two different strains of Streptococcus mutans [9]. In our study, the MIC and MBC of the crude extract of mangosteen pericarp for Lactobacillus acidophilus (25 mg/ml) was comparable to that of gold standard chlorhexidine having an MIC of 20 mg/ml. Similar study was reported by Linuma et al., who showed the presence of one active isolate, alpha mangosteen, a xanthone derivative with a MIC of 1.57 -1.5 μg/ml [18]. Our study was one of the few study to assess the effect of mangosteen extract on a group of oral cariogenic microorganisms.
Limitation
The crude form of mangosteen pericarp was used in our study. The major active compound in mangosteen pericarp was not isolated and identified. It is possible that a combination of active compounds may be responsible for inhibition rather than a single compound giving the synergistic effect as a whole.
Conclusion
We concluded that the crude chloroform extract of mangosteen pericarp showed an effective zone of inhibition against Streptococcus mutans, Streptococcus sanguis, Streptococcus salivarius, Streptococcus oralis and Lactobacillus acidophilus. Thus, the mangosteen pericarp extract showed promising activity against the dental pathogens. Further purification studies to analyze the active biocompound from chloroform extract would aid in designing a novel drug in the treatment of dental infections like caries.
*-Significant