Mullerian Agenesis Associated with Turner’s Syndrome
Padmanabhan Elamparidhi1, Rudrappa Ramesh Kumar2, Selvakkalanjiyam Sivaranjinie3, Rajakumar Sibhithran4
1 Senior Resident, Department of Radio-Diagnosis, Sri Manakula Vinayagar Medical College and Hospital, Madagadipet, Puducherry, India.
2 Professor and Head of the Department, Department of Radio-Diagnosis, Sri Manakula Vinayagar Medical College and Hospital, Madagadipet, Puducherry, India.
3 Junior Resident, Department of Radio-Diagnosis, Sri Manakula Vinayagar Medical College and Hospital, Madagadipet, Puducherry, India.
4 Junior Resident, Department of Radio-Diagnosis, Sri Manakula Vinayagar Medical College and Hospital, Madagadipet, Puducherry, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Padmanabhan Elamparidhi, Department of Radio-Diagnosis, Sri Manakula Vinayagar Medical college and Hospital, Madagadipet, Puducherry- 605107, India.
E-mail: pepsantosh@gmail.com
Turner’s syndrome is a chromosomal disorder with 45 X0 due to absence of a set of gene from the short arm of X chromosome. The incidence of Turner’s syndrome is 1 in 2500 live births. Primary amenorrhea is well known in Turner’s syndrome, the reason being streak ovaries; but mullerian agenesis as a cause of primary amenorrhea in Turner’s syndrome is a very rare entity. The incidence of Turner’s syndrome associated with mullerian agenesis is extremely rare as there is only a hand full of cases reported in literature. We report a rare case of adolescent female who presented with primary amenorrhea and found to have Turner’s syndrome with mullerian agenesis.
Gonadal dysgenesis, Missing X chromosome, Mullerian development, Mullerian anomaly, Sex chromosome
Case Report
A 17-year-old female presented to the gynaecology OPD with complains of primary amenorrhea, short stature and absence of secondary sexual characters. Her height was 135cm and weight of 30 kg with normal intelligence. She was born of consanguineous marriage and had normal milestones. Her siblings were normal and did not have similar complaints.
On examination, her vitals were PR – 66/min, BP – 110/68 mm Hg; CVS, RS, CNS examination showed no significant findings. On local examination, there was no pubic hair, no axillary hair and no breast bud development. On examination of external genitalia labia majora and minora were developed but clitoris was under-developed. On laboratory investigations, blood routine, renal function test and thyroid function test were normal. FSH was elevated but LH was in normal range.
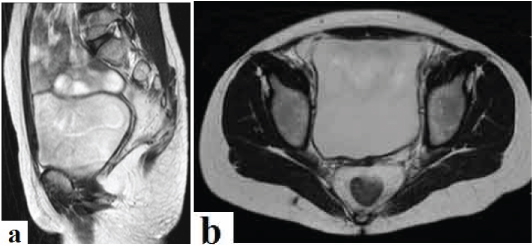
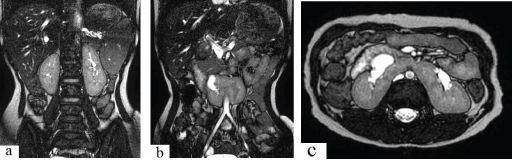
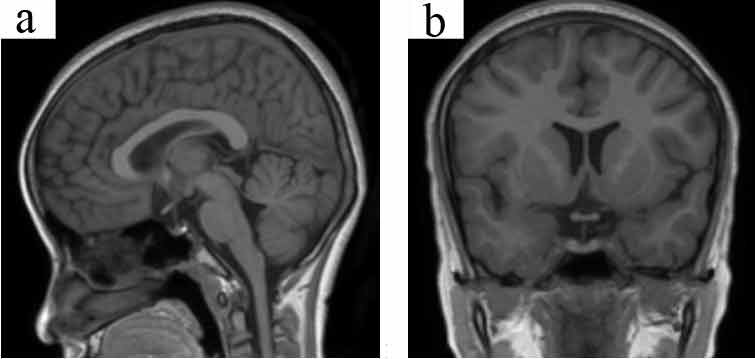
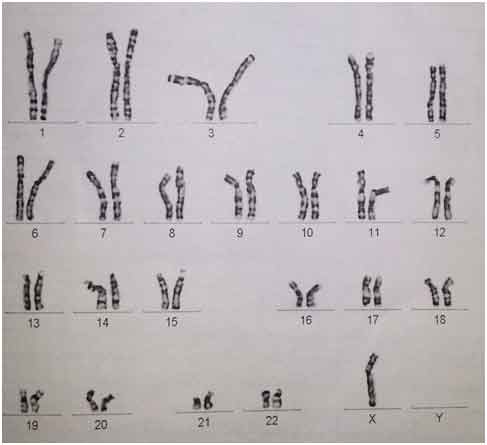
She was referred to radiology department for Ultrasonography of abdomen which revealed horse shoe kidney with absence of uterus and ovaries. MRI abdomen and pelvis confirmed the absence of uterus and ovaries [Table/Fig-1a,b] along with the presence of horse shoe kidney [Table/Fig-2a-c]. MRI brain was screened for any pituitary pathology in view of amenorrhea, but turned out to be normal [Table/Fig-3a,b]. With the suspicion of Turner’s syndrome, karyotyping was performed which supports the diagnosis by the absence of one X chromosome (45 XO) [Table/Fig-4].
T2WI sagittal and axial sections showing absent uterus and ovaries in the pelvis.
T2WI Coronal and Axial sections of upper abdomen shows parallel orientation of both the kidneys with fusion of their lower poles forming isthmus across the midline. Both the renal pelvis face anteriorly.
T2WI sagittal and coronal sections of brain showing normal pituitary gland with stalk.
Karyotyping – 72 hour PHA stimulated lymphocyte culture showed chromosomal pattern of Turner’s Syndrome (45 XO).
Hence a diagnosis of Turner’s syndrome with mullerian agenesis was made. A skeletal survey was performed as a workup for Turner’s syndrome which showed positive metacarpal sign-shortening of 4th metacarpal [Table/Fig-5]. A 2D echo was performed to look for bicuspid aortic valve and was negative. Screening of chest for coarctation of aorta was taken which showed normal aortic knuckle and no inferior rib notching-ruling out any abnormality.
X-Ray AP view of both hands showing positive metacarpal sign – shortening of 4th metacarpal leading to line joining the 4th and 5th metacarpals dissecting the head of the 3rd metacarpal in both hands.

Patient was counseled and was put on Estrogen therapy for the development of secondary sexual characters.
Discussion
During the first 6 weeks of development the male and female fetus is indistinguishable which demonstrates both mesonephric and para mesonephric duct. The presence of Y chromosome is associated with production of mullerian inhibiting factor [1]. The absence of mullerian inhibiting factor in females promotes the growth of paired mullerian ducts along the lateral aspect in conjunction with regression of the mesonephric ducts. Interruption in this development leads to aplasia or hypoplasia of the vagina, cervix or uterus. If proximal 2/3rd of the vagina, cervix and uterus show agenesis or hypoplasia, it is a part of Mayer Rokitansky Kuster Hauser (MRKH) syndrome-most extreme form of mullerain duct anomalies. Though primary amenorrhea will be the major complaint, mullerian agenesis usually presents with normal secondary sexual characters and normal hormonal profile [2].
Imaging features show absence of uterus, fallopian tubes and upper 2/3rd of vagina with normal appearing ovaries. MRKH features with absence of bilateral ovaries should raise the suspicion of associated Turner’s syndrome. The incidence of Turner’s syndrome associated with mullerian agenesis is not known as only very few cases have been reported [3].
Turner’s syndrome is a form of gonadal dysgenesis that affects 1 in 2500 live births. Pathogenesis is unclear. It is one of the causes for primary amenorrhea. It is a chromosomal disorder that is characterized by the absence of X chromosome which maybe partial or complete. Patients are usually females and present with streak ovaries that leads to primary amenorrhea or premature ovarian failure. The ovaries usually develop normally at first, but the egg cells die prematurely and most of the ovarian tissue degenerates before birth. In most of the females, hormonal therapy is required for attaining menarche and development of secondary sexual characters [4]. There will be streak ovaries but the uterus, fallopian tube, vagina will be developed normally. In almost 95% of cases there will be short stature and loss of ovarian function.
Turner’s syndrome is usually present with increased skin fold (webbed neck), low hairline at the back, puffiness or swelling of the face (lymphoedema) of hand and foot, skeletal abnormalities, horse shoe kidney and congenital heart diseases. In congenital heart disease the most common one is coarctation of aorta. Intelligence is usually normal. On hormonal studies, patients usually have associated hypothyroidism. On imaging studies, chest X-Ray PA view shows inferior rib notching characteristic of coarctation of aorta and USG abdomen will show horse shoe kidney with streak ovaries and normal uterus. Skeletal abnormalities that are present in concordance would be scoliosis, positive metacarpal sign which is shortening of the 4th metacarpal, made lung deformity [5].
Hormonal therapy in these patients can help in development of secondary sexual characters. In vitro fertilization with donor oocytes also helps in successful reproduction.
It is difficult to find out the cause of association of both the syndromes in a single patient. The most possible cause may be the activating mutation of anti-mullerian hormone gene located on q13 on chromosome 12 might be contributory to the regression of mullerian duct derivatives like fallopian tube, uterus, cervix and upper one third of vagina in a patient who has Turner’s phenotype [6].
It is essential to differentiate this condition from isolated MRKH or Turner’s syndrome. In MRKH syndrome there is complete absence of uterus, fallopian tubes and upper 2/3rd of vagina but the ovaries appear normal. In Turner’s syndrome, ovaries appear streaky but uterus, tubes, cervix and vaginal development will be normal.
Such an association of Turner’s syndrome along with mullerian agenesis leads to a very poor or no chance of conception in these patients. Estrogen therapy can result in development of breast and bone growth, but induction of menstruation is very rare [7].
Conclusion
Mullerian agenesis with Turner syndrome is a very peculiar and unique association. Imaging of a patient with primary amenorrhoea showing absence of bilateral ovaries in addition to features of mullerian agenesis should raise the suspicion of associated Turner’s syndrome as there is no chance of conception in such alliance.
[1]. Bhuyan AK, Sarma D, Saikia UK, Contemporary issues in primary amenorrhea: An experience from a Tertiary Care CenterIndian J Endocrinol Metab 2012 16:S387-88. [Google Scholar]
[2]. Behr SC, Courtier JL, Qayyum A, Imaging of Müllerian Duct AnomaliesRadio Graphics 2012 32(6):E233-50. [Google Scholar]
[3]. Suresh V, Ramana S, Rahul C, A rare case of Turner’s syndrome presenting with Mullerian agenesisJ Hum Reprod Sci 2013 6(4):277-79. [Google Scholar]
[4]. Bondy C, Bakalov V, Cheng C, Olivieri L, Rosing D, Arai A, Bicuspid aortic valve and aortic coarctation are linked to deletion of the X chromosome short arm in Turner syndromeJ Med Genet 2013 50:662 [Google Scholar]
[5]. Kim HK, Gottliebson W, Hor K, Backeljauw P, Gutmark-Little I, Salisbury SR, Cardiovascular Anomalies in Turner Syndrome: Spectrum, Prevalence, and Cardiac MRI Findings in a Pediatric and Young Adult PopulationAJR Am J Roentgenol 2011 196(2):454-60. [Google Scholar]
[6]. Reindollar RH, Byrd JR, McDonough PG, Delayed sexual development: a study of 252 patientsAm J Obstet Gynaecol 1981 140:371-80. [Google Scholar]
[7]. De Leon FD, Hersh JH, Sanfilippo JS, Schikler KN, Yen FF, Gonadal and müllerian duct agenesis in a girl with 46, X, i (Xq)Obstet Gynaecol 1984 63(3 Suppl):81-3. [Google Scholar]