A Case Report on Multiple Stones in the Thyroid Gland in Association with Sclerosing Thyroiditis: An Unusual Encounter
Gaurav Shandilya1, Ravish Kumar Sinha2, Nishith Ekka3, Vinod Kumar4
1 Senior Resident, Department of General Surgery (Trauma and Emergency), AIIMS, Patna, Bihar, India.
2 Assistant Professor, Department of General Surgery, Narayan Medical College and Hospital, Sasaram, Bihar, India.
3 Assistant Professor, Department of General Surgery, Rajendra Institute of Medical Sciences, Ranchi, Jharkhand, India.
4 Associate Professor and Unit Chief, Department of General Surgery, Rajendra Institute of Medical Sciences, Ranchi, Jharkhand, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Gaurav Shandilya, S/o Mr. Tej Narayan Singh, Airport Road, Chhota Bariyarpur, Motihari, East Champaran-845401, Bihar, India.
E-mail: megauravshandilya@gmail.com
Stones are very frequently found in the gallbladder and urinary tract. Rarely the thyroid gland can be a site for stone formation. Few cases of calcification in thyroid gland have been described in the medical literature in association with papillary carcinoma and multinodular goiter. A unique case of a thyroid swelling studded with multiple stones in its parenchyma, in the histopathological background of sclerosing thyroiditis in an 80-year-old male is documented here. Surgical excision was undertaken with an uneventful postoperative period.
Benign, Calcification, Thyroid parenchyma
Case Report
An 80-year-old male presented in the surgical OPD with complains of a gradually increasing swelling in the front and right side of the neck for the last 5 years. Also, there was complain of progressive dysphagia for last 3-months. There was no history of dyspnoea or dysphonia. There was no history of any drug intake or medication for any thyroid disease. There was no history of trauma, fever or any local pathology in the past.
On clinical examination, there was a solitary vague midline swelling of size 8cm x 8cm in the thyroid region, more towards right side. Swelling moved slightly up with deglutition. Surface was smooth, margins ill-defined, hard in consistency with very limited mobility in horizontal and vertical dimensions, non-tender with normal temperature in whole of the swelling. No Lymph-node was palpable in the neck.
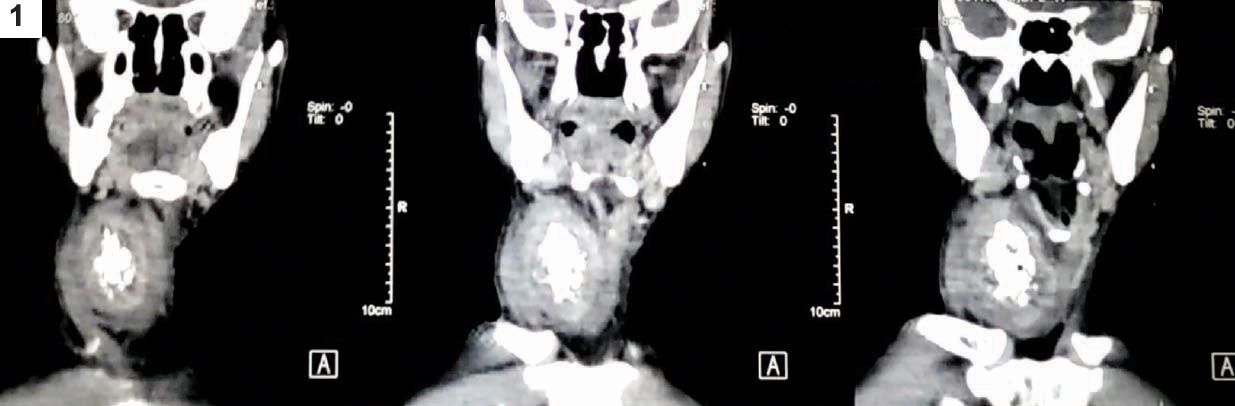
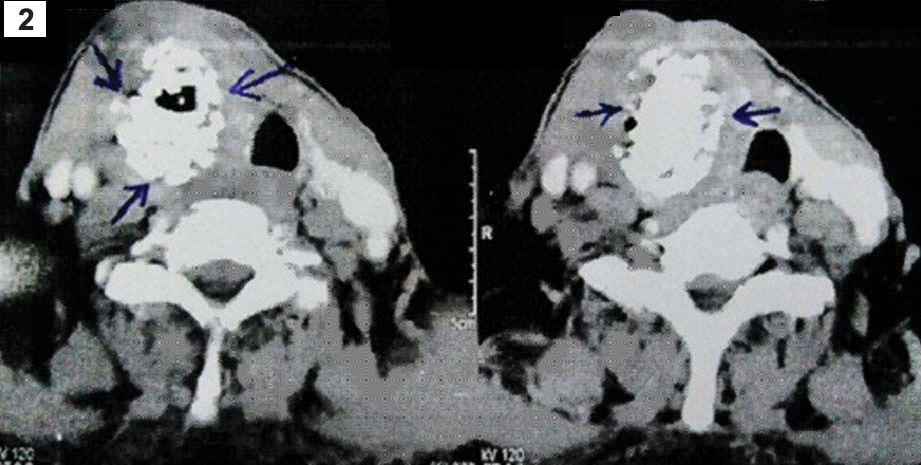
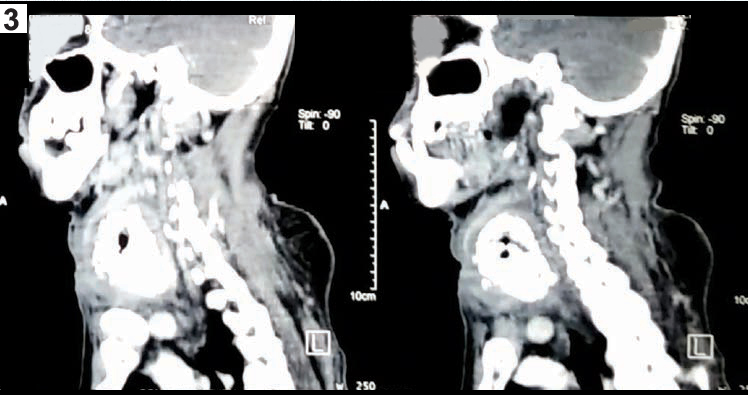
The swelling on ultrasonography, showed a soft tissue mass with multiple hyper-echoic foci suggestive of calcification arising from right lobe of thyroid. Fine Needle Aspiration Cytology (FNAC) was attempted at multiple sites but it was difficult to perform. Bone-like resistance was experienced on passing 22-gauze needle and smear failed to produce any valuable result. CT Scan revealed a heterogeneous enhancing mass of size 7.5cm x 4.8cm x 4.8cm with coarse calcification noted in it, arising from Right lobe of the thyroid gland [Table/Fig-1,2 and 3]. Thyroid Profile of patient was normal.
CT Image showing the front view of neck region, showing coarse calcification.
Cross sectional view of the Thyroid region showing radiodense shadows (marked with arrows), suggestive of calcification within the thyroid parenchyma.
CT Image showing calcification in thyroid region.
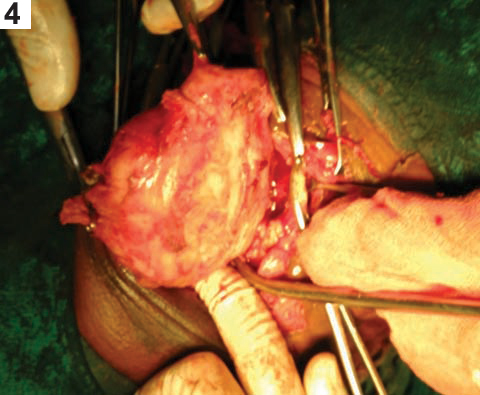
The patient was prepared for surgery and was taken under general anaesthesia. A classical Kocher’s incision was made and the thyroid gland was approached. A stony hard mass was found to be arising from right lobe of the thyroid gland [Table/Fig-4]. Mass was densely adherent to trachea and oesophagus. Right hemithyroidectomy was performed and excised tissue was sent for histopathological examination.
On histopathology a partly cut open soft tissue nodular mass measuring 8cm x 6cm x 4cm was received. External surface was capsulated. Cut surface showed specimen entirely composed of cystic lesion. Lumen and wall showed grey yellow calcification. Normal thyroid tissue was not identified [Table/Fig-5].
Thyroid tissue cut open, showing multiple stones inside the specimen.

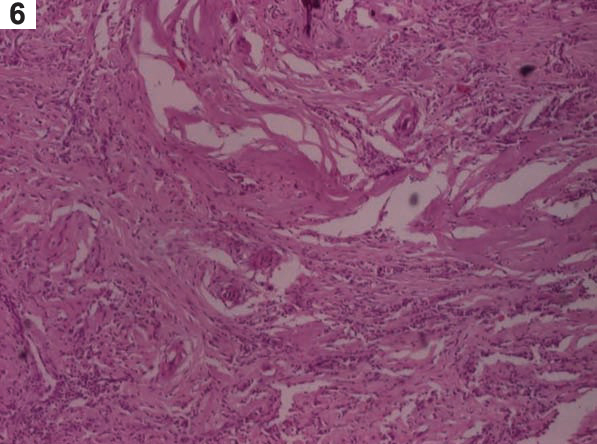
Microscopically multiple micro-sections were examined, showed skin covered cystic thyroid lesion with extensive areas of dense chronic inflammation. Infiltration was composed of lymphocytes, plasma cells, histiocytes. There were marked areas of fibrosis and calcification. Entrapped thyroid follicles appeared benign with tiny foci of Hurthle cell change. There was no evidence of malignancy [Table/Fig-6]. All these histopathological features were suggestive of sclerosing thyroiditis without any evidence of malignancy. Stone analysis showed that the stones were composed of Calcium phosphate or Apatite [Table/Fig-7]. Post operative period was uneventful, patient was lost on follow up.
Marked areas of fibrosis with focal areas of calcification and entrapped thyroid follicles (H&E, 40X).
Photograph showing discrete stones.

Discussion
Calcification in the thyroid gland, though a rare phenomena, has been described in association with both benign e.g., Multi nodular goitre and malignant conditions e.g., Papillary carcinoma [1]. Few other entities simulating this condition are Riedel’s Thyroiditis and Anaplastic carcinoma of the thyroid gland.
Very rarely a fully developed solitary stone can be found, and few such cases has been reported in the medical literature [2,3]. Dhingra et al., and Venugopal et al., both reported a case of solitary thyroid stone in association with colloid goiter [2,3]. None of them, reports a case with multiple thyroid stones. Finding such a case and that too in the histopathological background of another rarer entity i.e., sclerosing thyroiditis seems to be unique.
Histologically, thyroid calcification can be classified as psammomatous and dystrophic types [4]. Psammomatous calcification consists of laminated round calcium deposits in the epithelium [5]. It is now well accepted that papillary thyroid carcinoma frequently forms psammomatous calcification, which can be detected as microcalcification on ultrasonography [6]. By contrast, dystrophic calcification consists of non-laminated amorphous deposits in fibrous septa rather than epithelium [5]. Studies have been carried out providing useful information about thyroid nodules with macrocalcification, and might be especially helpful in cases with inadequate FNAC for predicting malignancy with ultrasonography [7].
Multifocal sclerosing thyroiditis is a condition which has been recognized with increasing frequency in the past few years, and which is characterized by multiple (sometimes innumerable) foci of fibrosis throughout the gland, often having a radial configuration [8]. On low power, the appearance can be indistinguishable from that of papillary microcarcinoma, but on high power one appreciates the lack of a neoplastic glandular component [8]. There are instead entrapped follicles in the midst of the scar, often distorted and lined by cells with vesicular (but not optically clear) nuclei [8]. Sometimes there is also a florid hyperplastic change in the follicles located at the interphase between the fibrotic strands and the surrounding parenchyma [8]. Multifocal fibrosing thyroiditis may be seen in an otherwise normal thyroid or against the background of a Hashimoto thyroiditis [8]. Despite the fact that it shares with Riedel’s thyroiditis, the deposition of abundant collagen, it does not seem to be related to the latter [8].
The evolution of all types of undifferentiated or anaplastic thyroid carcinoma is very rapid, with massive growth in the neck and infiltration of the ribbon muscles, oesophagus, trachea, skin, and even contiguous bones [9]. Nodal and distant metastases are also common [10]. The mortality rate is over 95%, the mean survival is less than 6 months, and the immediate cause of death is usually involvement of vital structures in the neck [11,12]. There is a slightly better chance of cure for patients in whom the undifferentiated component is only a focal change in an otherwise well-differentiated neoplasm. Isolated successes have been obtained with a combination of surgery, radiation therapy, and chemotherapy [13,14]. Even though we are considering conditions like Anaplastic carcinoma and Riedel’s thyroiditis as differential diagnosis, the act of hemithyroidectomy is justified in this case. Surgical planes and anatomical landmarks were obliterated because of the infiltrative nature of disease and vocal-cord paralysis is an anticipated complication in such cases if more extensive dissection is carried out. The primary aim of hemithyroidectomy performed in this case was relieving the pressure symptom e.g., dysphagia.
Conclusion
Rarely well formed stones can be found in the thyroid gland. Though there are significantly high chances of malignancy in association with calcification but the mere presence of stones do not indicate malignancy, as in this case itself. In the absence of definitive tissue diagnosis of the lesion, surgical treatment should be tailored to relieve the symptoms arising due to pressure effect of the lesion.
[1]. Jun P, Chow LC, Jeffrey RB, The sonographic features of papillary thyroid carcinomas: pictorial essayUltrasound Q 2005 21:39-45. [Google Scholar]
[2]. Dhingra V, Misra V, Singh PA, Bhatia R, Sharma N, Pearl pendant around her neck: an unusual case of stone seen in a colloid goiterJ Clin Diagn Res 2010 4(2):2297-99. [Google Scholar]
[3]. Gopal PR, Kumar P, George GK, Hood N, James L, Manoj M, Round pendant around the neck- thyroid a reviewIndian Journal of Surgery 2014 76(5):378-81. [Google Scholar]
[4]. Takashima S, Fukuda H, Nomura N, Kishimoto H, Kim T, Kobayashi T, Thyroid nodules: re-evaluation with ultrasoundJ Clin Ultrasound 1995 23:179-84. [Google Scholar]
[5]. Klinck GH, Winship T, Psammoma bodies and thyroid cancerCancer 1959 12:656-62. [Google Scholar]
[6]. Komolafe F, Radiological patterns and significance of thyroid calcificationClin Radiol 1981 32:571-75. [Google Scholar]
[7]. Park YJ, Kim J, Son EJ, Youk JH, Kim EK, Kwak JY, Thyroid nodules with macrocalcification: sonographic findings predictive of malignancyYonsei Med J 2014 55(2):339-44. [Google Scholar]
[8]. Poli F, Trezzi R, Fellegara G, Rosai J, Images in pathology. Multifocal sclerosing thyroiditisInt J Surg Pathol 2009 17:144 [Google Scholar]
[9]. Banville NM, Timon CI, Bermingham NJ, Toner ME, Anaplastic and squamous thyroid carcinoma masquerading as primary mucosal squamous cell carcinoma of the trachea: morphologic and immunohistochemical findingsLab Invest 2009 89(Suppl.1):245A [Google Scholar]
[10]. Nishiyama RH, Dunn EL, Thompson NW, Anaplastic spindle-cell and giant-cell tumors of the thyroid glandCancer 1972 30:113-27. [Google Scholar]
[11]. Carcangiu ML, Steeper T, Zampi G, Rosai J, Anaplastic thyroid carcinoma. A study of 70 casesAm J Clin Pathol 1985 83:135-58. [Google Scholar]
[12]. Venkatesh YS, Ordóñez NG, Schultz PN, Hickey RC, Goepfert H, Samaan NA, Anaplastic carcinoma of the thyroid. A clinicopathologic study of 121 casesCancer 1990 66:321-30. [Google Scholar]
[13]. Kim JH, Leeper RD, Treatment of anaplastic giant and spindle cell carcinoma of the thyroid gland with combination adriamycin and radiation therapyCancer 1983 52:954-57. [Google Scholar]
[14]. Spanos GA, Wolk D, Desner MR, Khan A, Platt N, Khafif RA, Preoperative chemotherapy for giant cell carcinoma of the thyroidCancer 1982 50:2252-56. [Google Scholar]