Hearing function is a special sense present among higher animals and is one of the most important sensory inputs for sustenance of life. It is amazing to think that such a small organ like the ear subserves such a vital function of hearing. More wonderful is that, within this minute organ, there are three small bones–malleus, incus and stapes strategically placed to form a semi rigid bony chain for conducting sound inside the middle ear and are the cornerstones for transmission of sound waves from the tympanic membrane to the inner ear [1]. Malleus is the lateral most ossicle, shaped like a hammer. It consists of a head, neck, lateral process, anterior process and a handle or manubrium. Incus resembles an anvil and consists of a body, a short process and a long process [2,3]. At the tip of long process, the incus has a small medially projecting mass called the lenticular process. This has sometimes been called the ‘fourth ossicle’ because of its incomplete fusion with the tip of the long process, thereby giving the appearance of separate bone or at least a sesamoid bone [1]. The lenticular process articulates with the head of stapes. Stapes is the smallest bone in the body that looks exactly like a miniature stirrup and consists of a small button like head on top, neck, two crura and a foot plate or base. The articular surface of the malleus is like an elongated saddle which articulates with the body of the incus by way of a saddle type of synovial joint. On the other hand, the head of stapes presents a cup shaped depression, which articulates with the lenticular process to form a synovial ball and socket type ‘incudo-stapedial’ joint. The development of the ear ossicles begins at fourth week of intrauterine life, fully ossify in the fourth month of intrauterine life and attain their full life-time size at birth [2,3].
For proper conduction of sound waves, an intact ossicular chain is required. The ossicular chain has a contributory effect in the direct reduction of the impedance mismatch caused as a result of sound waves traversing through different media before stimulating the auditory hair cells [1].
Another important factor is the mobility of the ossicles. Any fixation or ankylosis of these joints also impedes sound waves captured by tympanic membrane to be transmitted from one ossicle to the other and finally to the inner ear. Damage to ossicles by disease or trauma can lead to hearing loss. Disruption of the continuity of the ossicular chain or the fixation of even one of the ear bones, either congenitally or due to disease, can both lead to decreased hearing [1].
Ossicles and their anomalies are known to form definitive components of many congenital craniofacial defects like Goldenhar syndrome (hemifacial microsomia), Treacher Collins syndrome, Branchio-oto-renal syndrome etc. Prenatal infection as well as medications (e.g., isotretinoin, thalidomide, anti-convulsants etc.) taken during pregnancy are associated with a host of abnormalities in the morphology of middle ear ossicles [1]. Abnormalities of malleus include absence of a part or the whole ossicle. The malleus may be fused to the lateral epitympanic wall or anteriorly to the tympanic ring. Occasionally all three ossicles are fused together. More frequently the incudo-malleolar joint is ossified. Abnormalities of the incus include absence of the long process or the lenticular process. Abnormalities of the stapes include absence of the superstructure, a decrease in size and a columella type stapes. Occasionally, the stapedial tendon is ossified and the stapes head may be fused to the promontory. There may be fixation of the stapes footplate [1].
Ossicular chain affected by acquired lesion of middle ear like Chronic Suppurative Otitis Media (CSOM) may lead to avascular necrosis of long process of the incus and the superstructure of stapes [3] or there is bone resorption owing to the bone eroding property of cholesteatoma in which ossicular chain involvement is relatively early [1].
Otolaryngologists employ advanced microsurgical reconstruction techniques in order to re-establish the audiological functions in patients who have lost them as a consequence of some disease process. Although, we have data on ossicles regarding their morphometry, morphology, anomalies, embryology, function and structure from different parts of the world, but the study on morphology of ossicles from Indian subjects is meagre.
Taking into consideration the burden of this disease in developing countries like India, where neglected CSOM with its complications are quite common among the lower socioeconomic group and thus, higher is the need for various reconstructive surgeries (sometimes using ossicular prosthesis); an attempt has been made in this study to compile data on these bones to find out the morphological variations on right and left sides.
Materials and Methods
The study was an institution based observational study, carried out in the Department of Anatomy in collaboration with the Department of ENT to observe the morphological variations of middle ear ossicles for a period of approximately one year from September 2014 to August 2015, on 26 cadaveric heads of both sexes and all ages with intact temporal region having intact ossicular chain with no discontinuity or erosion. The ossicles which were found to be eroded as a consequence of CSOM or other diseases, or affected by ankylosis (as with head of malleus or Stapes footplate fixation as in Otosclerosis) were excluded from the study. Approval of the proposal by the institutional authority was obtained. The procedure that was followed for obtaining the ear ossicles was similar to initial steps of ‘classic intact canal wall mastoidectomy-inside out technique’ [4,5]. To expose the head of malleus, body and short process of incus, the attic needed to be opened up by using the micro drill. On drilling out the lateral wall of the epitympanum, the head of malleus, body of incus were seen. On further drilling posteriorly across the aditus towards the mastoid antrum, the fossa incudis with the short process of incus were visualized. The ligaments of these ossicles which attach them to the walls of tympanic cavity were cut. First, the malleus was disarticulated from the body of incus. Then, the incudo-stapedial joint was divided and stapes was seen postero-medially. Ultimately, stapes was brought out by introducing curved hook in the foramen obturatum. The variations of ossicles were observed under the magnification of the operating microscope. All the morphological parameters were compared on the basis of side of origin – between right and left sided ossicles. Results were statistically analysed using the SPSS software, Version -16 using chi-square test in which p < 0.05 was considered as statistically significant.
Results
The study was conducted on 52 sets of malleus, incus and stapes, of which 26 sets of ossicles were right sided and 26 sets were left sided. The following morphological variations in the ossicles were noted.
Malleus:
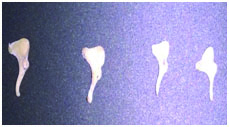
The malleus showed variations in its distal portion, i.e., in the free ends of the manubrium, lateral process and anterior process. The free end of manubrium varied between anteriorly directed curve and straight line [Table/Fig-1].
Malleus with variations in the free ends of manubrium – showing straight and curved handle.

Out of 52 mallei, 29 (55.8%) had the free ends curved anteriorly (Right-15 and Left-14) and 23 (44.2%) had straight free ends (Right-11 and Left-12) of manubrium [Table/Fig-2]. No statistical significant difference was observed when such morphological parameters were compared (Chi-square value=0.078, df=1, p=0.78). In some mallei, the lateral processes were quite long and sharp while others were blunt. The length of the anterior process was also variable. One had a very small and blunt process, almost to the point of absence [Table/Fig-3].
Assessment of morphological parameter of malleus according to curvature of manubrium.
| Side | Curved manubrium | Stright manubrium | Total |
|---|
| Right | 15 (57.7%) | 11 (42.3%) | 26 (100%) |
| Left | 14 (53.8%) | 12 (46.2%) | 26 (100%) |
| Total | 29 (55.80%) | 23 (44.2%) | 52 (100%) |
Malleus whose anterior process is ‘almost absent’ (shown with arrow).

Incus:
Variations in incus were found to be much less as compared to other ossicles [Table/Fig-4].
Incus - the ossicle with least variations.
The long processes of incii did not show much variation. But one peculiar short, stubby incus was found in this study, which had a small short process and almost triangular projecting long process and a small body [Table/Fig-5].
A peculiar short stubby incus with a small short process and triangular projecting long process.

The short process of 21 (40.4%) incii showed a notch in inferior border (Right-13 and Left-8). [Table/Fig-6]. Courses of these notches were either forward or upward. Out of the 21 incii, 12 (57.1%) incii showed an upward course (Right–7 and Left–5), whereas 9 (42.9%) showed a forward course (Right-6 and Left–3) of the notches [Table/Fig-7]. Statistical significant difference was not observed when such morphological parameters were compared (Chi-square value=1.99, df=1, p=0.26).
The short process of incus showing a notch in inferior border.

Assessment of morphological parameter of incus according to notch in short processes.
| Variation of notch in inferior border | Right side | Left side | Total |
|---|
| Notch present | 13 (50%) | 8 (30.8%) | 21 (40.4%) |
| Upward course of notch | 7 (53.8%) | 5 (19.2%) | 12 (57.1%) |
| Forward course of notch | 6 (46.2%) | 3 (62.5%) | 9 (42.9%) |
Stapes:
Stapes showed maximum morphological variations among the middle ear ossicles. The variations of stapes were in the neck, crura and the obturator foramen. The obturator foramen showed a variety of shapes.
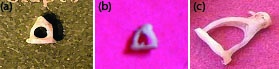
The various shapes observed were: Oval: Right–9, Left–8 and in total 17 (32.7%), Circular: Right-4 and Left-5 and in total 9 (17.3%), Triangular: Right–12 and Left–11 and in total 23 (44.2%), Tunnel Shaped: Right–1 and Left–2 and in total 3 (5.8%) [Table/Fig-8,9]. On doing comparison between right and left sided stapes, no statistical significance was found between foramina of various shapes (Chi-square value=0.547, df=3, p=0.91).
Assessment of morphological parameter of stapes according to shapes of obturator foramen.
| Shape of foramen | Right side | Left side | Total |
|---|
| Oval | 9 (34.6%) | 8 (30.8%) | 17 (32.7%) |
| Circular | 4 (15.4%) | 5 (19.2%) | 9 (17.3%) |
| Triangular | 12 (46.2%) | 11 (42.3%) | 23 (44.2%) |
| Tunnel Shaped | 1 (3.8%) | 2 (7.7%) | 3 (5.8%) |
Stapes with circular (a), triangular (b) and Tunnel-shaped (c) obturator foramen whose posterior crus is more curved than anterior crus.
In only 7 (13.5%) cases (Right–4 and Left–3), the anterior and posterior crura were symmetrical in the sense both the crura were equally curved. In 31 (59.6%) stapes (Right–14 and Left–17), the anterior crus were straight as compared to the posterior crus, which was curved. The rest 14 (26.9%) stapes (Right–8 and Left–6) had a more curved anterior crus than the posterior crus [Table/Fig-10]. Statistical significant difference was not observed when such morphological parameters were compared (Chi-square value=0.165, df=1, p=0.68).
Assessment of morphological parameter of Stapes according to symmetry of crural Curvature.
| Side | Symmetrical crura | Asymmmetrical crura |
|---|
| Anterior straight crus | Anterior curved crus |
|---|
| Right | 4 (15.4%) | 14 (53.8%) | 8 (30.8%) |
| Left | 3 (11.5%) | 17 (65.4%) | 6 (23.1%) |
| Total | 7 (13.5%) | 31 (59.6%) | 14 (26.9%) |
The necks of stapes were well defined in most of the specimens in our study. Some had short neck, while others had long neck. One specimen had no neck and in this case the head seemed to be directly resting on the shoulders.
Discussion
Among the ossicles, stapes is the most variable and incus is the most stable ossicle so far as their morphological variations are concerned [6–10]. Earlier studies revealed that congenital abnormalities of ossicles were accompanied by malformation of facial nerve and its aberrant development in cranium [11]. Recently, a study on human fetal ear ossicles has reported that destitute human fetuses can be used as homografts to replace eroded adults ear ossicles [12]. Due to the present availability of newer surgical techniques and with the advent of powerful operating microscopes, micro instruments and various ossicular prosthesis, reconstruction of the lost ossicular elements are now-a-days new horizons where we may contribute promising results. For middle ear reconstruction with ossicular homografts obtained from cadavers, authors have suggested to follow proper sterilization protocol as a valid and inexpensive approach in order to inactivate any possible chance of transmission of virus or prion [13,14].
In the present study, 55.8% of mallei had a curved free end of its manubrium while 44.2% of them had a straight free end. This goes in conjunction with the previous studies [6,7,10,15]. Crabtree et. al., mentioned findings of underdeveloped malleus and malleus fused with incus [16]. Nomura et al., gave description of peculiar findings such as spindle shaped handle of malleus and malleus bar [17]. Todd and Creighton observed 82 mallei in which one case with absent lateral process and inflected manubrium was mentioned [18]. But, such unusual presentations were not seen in the present study.
Another finding which was observed in other studies was absence of neck of malleus but having large and long lateral processes [6,10]. In the present study, however, all mallei had prominent necks with a groove like impression for the attachment of the tensor tympani muscle but the lateral and anterior processes of mallei showed variations and one malleus had a very short and blunt anterior process unlike that of a bony process projecting from head as mentioned by Mogra et al., [10].
In this present study, the long processes of incus were all similarly and uniformly curved having a lenticular process. Similar data was also obtained from previous studies [6, 7,15,18]. We did not find any variation like absence of long processes of incus with fibrous band replacing it (by connecting the body with the head of stapes) which are mentioned in literatures [6,19].
The only notable morphological variation found was the presence of a notch in the inferior border of short process of incus in 40.4% cases in the present study. It has been reported that early development of the posterior ligament of incus connecting the end of the short process to the fossa incudis in foetus may result growth of the bone around it and produces the notch [20]. Arensburg et al., reported such a finding in 41-42% whereas Unur et al., found it in 42% of cases [6,20]. The course of the notch was found to be either forward (42.9%) or upward (57.1%) in our study. The variations in the course could be caused by the angle between the origin and insertion of the posterior ligament.
Another thing that deserves special mention in the present study is the finding of a peculiar short stubby incus with a small short process and triangular projecting long process. To our knowledge such anomaly has not been previously documented [Table/Fig-6].
The variations of the stapes could be in the neck, crura and foramen obturatum as documented in previous studies [6,7,21]. The presence of an anatomical neck of the stapes remains controversial as stated by Dass et al., [22]. In our study, there were variations in the neck ranging from short neck to long neck. We also noted one stapes without a neck. In such cases, the stapedius tendon was attached to the posterior crus at its upper end.
Variations in the shape of foramen obturatum ranging from circular, oval, triangular and tunnel shaped hole along with non perforated obturator foramen were mentioned in different studies [6,19]. The shape of obturator foramen of stapes widely varied in our study also, but a stapes without a hole was not seen.
The stapes in the present study were found to be having both symmetrical as well as asymmetrical crura. In 13.5% specimens, both the crura were equally curved whereas in 86.5% cases, they were asymmetrically curved with majority (59.6%) having more curved posterior crus and relatively straight anterior crus. Similar morphological variations were found in the study by Unur et al., and Wadhwa et al., [6,21].
Solid aplasia of stapes is very rare but many forms of hypoplasia, like absence of either anterior crus or posterior crus or both have been mentioned in previous studies. Reports of stapes with fused crura and no footplate are also found [8,19]. Farahani and Nooranipour stated straighter anterior crus than posterior one as the most constant finding of stapes in their study [23]. All stapes anomalies combined with incus anomaly were unilateral as mentioned by them. In addition, incudostapedial discontinuity was also reported as a very characteristic form of variation of articulated ossicular chain [24]. But in the present study, we did not come across such major deviations from the normal architecture of stapes. Anatomical variations of stapes may differ in type and extent [22]. Such anomalies have been interpreted to be a developmental aberration involving the second branchial arch (like partial absence of second arch derivative in the case of absent superstructure) from which stapes develops [25]. It is very difficult to appreciate why anomalies were involved more in second arch originated ossicles, restricted only to stapes, and not involving other ossicles developing from the same arch. Thus, we see stapes anomalies were detected with no fixed patterns; therefore, it is expected to detect a large variety of these patterns in future [19].
Limitation
As the sample size in this study depends upon the availability of cadaveric heads in the Department, proper sampling methods could not be employed in the selection of the samples and the maximum number of cadaveric heads that was available in the department during the study period was taken into study, it might so happen that our sample size might not be fulfilled due to scarcity of cadavers. There are certain studies which suggest post natal growth as well as sex related differences of the ossicles. This present study did not have any bias for the age and sex related changes in the ossicles. So, further studies can be done to get a clear idea about such age and sex related changes in the ossicles, if any.
Conclusion
From such analytical study of the ossicles, it could be concluded that the stapes is the most variable and the incus is the most stable ossicle so far as morphological variations are concerned. Occurrence of such variations is thought to have a direct impact in the pre-surgical evaluation, on the course of surgery and is also critical for reconstructing the conduction apparatus. It is expected that this work may also inspire many others to continue temporal bone dissection with a view to gather more ossicles which might be preserved in ossicular banks by following proper preservation and sterilization methods as per protocol for future use as homografts in ossiculoplasty. These harvested ossicles may be used to replace eroded middle ear ossicles as an alternative to manufactured prosthesis.