To Operate or not to Operate the Mid-Shaft Fractures of the Clavicle: A Comparative Study of Functional Outcomes of the Two Methods of Management
Sanath Kumar Shetty1, Ragesh Chandran2, Arjun Ballal3, Lawrence John Mathias4, Anoop Hegde5, Ashwin Shetty6
1 Assistant Professor, Department of Orthopaedic Surgery, K.S. Hegde Medical Academy, Deralakatte, Mangalore, Karnataka, India.
2 Registrar, Department of Orthopaedic Surgery, ARS Hospital, Tirupur, Tamil Nadu, India.
3 Consultant Orthopaedic Surgeon, Ballal Healthcare, Udupi, Karnataka, India.
4 Professor, Department of Orthopaedic Surgery, K.S. Hegde Medical Academy, Deralakatte, Mangalore, Karnataka, India.
5 Registrar, Department of Orthopaedic Surgery, ARS Hospital, Tirupur, Tamil Nadu, India.
6 Professor, Department of Orthopaedic Surgery, K.S. Hegde Medical Academy, Deralakatte, Mangalore, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Arjun Ballal, Consultant Orthopaedic Surgeon, Ballal Healthcare, Sweeny Complex, Santhekatte, Udupi-76103, Karnataka, India.
E-mail: 5arjunballal@gmail.com
Introduction
Fractures of the clavicle are some of the most common fractures which are seen in the adult population. Mid-shaft fractures of the clavicle are considered the most common form of clavicle fractures and about half of them are displaced fractures. They have been managed non-operatively over the years. However, severe displacement and comminution of these fractures have warranted the requirement of operative intervention, due to increased incidence of mal-union, worsening of shoulder functions etc., after conservative management. The introduction of locking compression plates, have increased the incidence of operative intervention in the management of these injuries.
Aim
To study and compare the functional outcome of the shoulder after open reduction and internal fixation versus non-operative management of mid-shaft clavicle fractures.
Materials and Methods
A prospective study was conducted from June 2013-October 2015 in the Department of Orthopaedic Surgery, K.S. Hegde Medical Academy, Mangalore. A total of 30 skeletally mature patients between the age groups of 20-50 years with diagnosed fresh mid-shaft clavicle fractures, AO type A and B mild to moderate displacement, were enrolled into the study with. They were divided into two groups randomly. Group 1 consisted 16 patients who underwent open reduction and locking compression plate fixation and Group 2 consisted of 14 patients who were managed with application of a clavicle brace and arm pouch for three weeks. Reviews were done at three, six and 24 weeks postoperatively. The patients were assessed clinically and radiographs were taken during all the reviews. Scoring of shoulder function was done using the Disabilities of the Arm, Shoulder and Hand (DASH) score during all the reviews. The results were tabulated compared and analyzed statistically using the ‘Independent t-test’ and Chi-square test.
Results
The DASH scores at the end of 24 weeks were noted to be 8.57±6.073 points for the 14 patients in the conservative management group and 7.74±16.422 points for the 16 patients in the open reduction and internal fixation group. This indicated that there was no significant difference noted in terms of shoulder function between the two groups. Six of the 14 patients in the conservative management group were noted to have mal-union of the fracture. No non-unions were noted in the conservative or operative groups. No mal-union was noted in the open reduction and internal fixation group.
Conclusion
Though open reduction and internal fixation of mid-shaft clavicle fractures reduced the incidence of mal-union, no significant difference was noted in the functional outcome of shoulder function as compared to when the fracture was managed conservatively.
Comminuted fractures, Conservative management, DASH score, Internal fixation, Locking compression plating, Open reduction
Introduction
Fractures of the clavicle, especially those of the mid-shaft, contribute to about 2.6-5% of all fractures in adults [1]. The mid-shaft area is the thinnest zone along the shaft of the clavicle, as well as the clavicle is not protected by any tissue, hence, more prone for fractures [2]. Literature states a 69-82% incidence of mid-shaft localization of clavicle fractures [1]. The mid-shaft fractures of the clavicle primarily occur lateral to the sternocleidomastoid muscle and medial to the coracoclavicular ligaments [2]. Due to such an anatomical presentation of the clavicle, the medial fragment rotates superiorly and posteriorly due to the sternocleidomastoid and the lateral fragment rotates inferiorly due to the pull of the pectoral muscles and the body weight [3]. Older studies and reports claimed a non-union rate of 1% after conservative management [4,5]. Recent studies reported a rate of non-union to be upto 15-20% with loss of shoulder strength and poor early functioning of the shoulder with sequelae even upto six months after injury [6–11]. Reports have stated a shortening of clavicle after conservative management post-trauma to be upto a mean of 1.2 cm [12]. Recent reports have shown that a shortened clavicle predisposes to symptoms of rapid loss of strength, fatigue and even hyperaesthesia of the upper limb [13].
As these injuries primarily occur in the young active, age groups for the avoidance of these complications, surgical treatment is gaining importance [2]. Several operative fixation techniques have developed over the years such as locking plates, Kirschner wires etc., [9,14–17].
The aim of the study was to study and compare the outcomes of shoulder function after open reduction and internal fixation of mid-shaft clavicle fractures versus conservative management of mid-shaft clavicle fractures and to study the complications occurring in both techniques.
Materials and Methods
A prospective study was conducted in the Department of Orthopaedic Surgery of Justice K.S. Hegde Charitable Hospital, Mangalore, Karnataka, India. A total of 30 diagnosed patients with fresh closed AO type A and B mid-shaft clavicle fractures with mild to moderate displacement [Table/Fig-1] between the age group of 20-50 years were enrolled into the study after obtaining the clearance from the ethical committee and informed consent from all the patients.
Right midshaft clavicle fracture. AO type A3.

Patients with diagnosed medical conditions such as diabetes mellitus, hypertension, associated ipsilateral upper limb injuries, solid organ injuries, head injuries, neurovascular injuries, osteoporosis, pathological fractures, AO type C fractures, undisplaced and severely displaced fractures, skeletally immature patients and patient refusal were criteria of exclusion from the study. The patients were divided into two groups after explaining the patients about both the methods of management and obtaining consent from them to be a part of either of the groups in the study.
Group 1 consisted of 14 patients who were managed conservatively by means of clavicle brace application and arm pouch application and immobilization for a total period of three weeks. The second group consisted of 16 patients who underwent operative fixation of the fracture by means of open reduction and internal locking compression plate fixation.
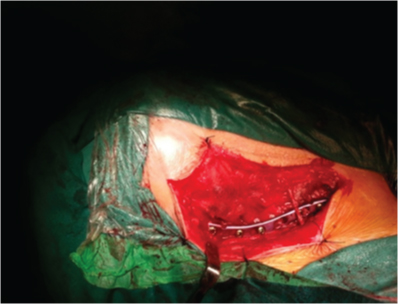
The surgical technique we employed included administration of intravenous antibiotics one hour before the scheduled time of surgery. The surgical technique involved positioning the patient in a beach chair position with placing a large bump between the two scapulae. The skin incision was centred over the fracture extending from the sternal notch to the acromion. The platysma was dissected and clavipectoral facia was incised along its attachment. Dissection was performed along the fragment and the fracture site was exposed. The reduction was performed and held with bone clamps. A seven hole or an eight hole clavicle locking compression plate was selected and fixed with screws inserted on either sides of the fracture engaging a minimum of six cortices. Skin was sutured in layers [18,19] [Table/Fig-2].
Intraoperative image showing locking compression plate fixation after open reduction of a midshaft clavicle fracture.
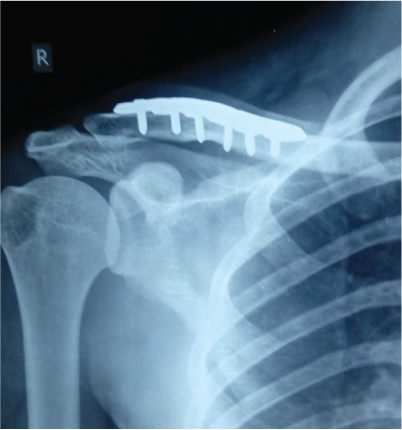
The postoperative protocol included immobilization of the patient on an arm pouch for a period of three weeks. Suture removal and discharge was started on postoperative day 10. Shoulder mobilization and rehabilitation exercises were begun during the review at postoperative week three for patients of either groups. Regular reviews were done at postoperative week three, six and 24. Review radiographs [Table/Fig-3,4] and assessment of shoulder function and scored with DASH scoring system [20] for both the groups. Complications noted during the reviews were documented. During the final review the final DASH scores and radiographs were analyzed and compared. All the results were tabulated, compared and analyzed statistically using the ‘Independent t-test’ and Chi-square test.
During the final review at 24 weeks after conservative management. A mild degree of mal-union is noted.

Right midshaft clavicle fracture during the final review at 24 weeks showing complete union of the fracture after locking compression plate fixation.
Results
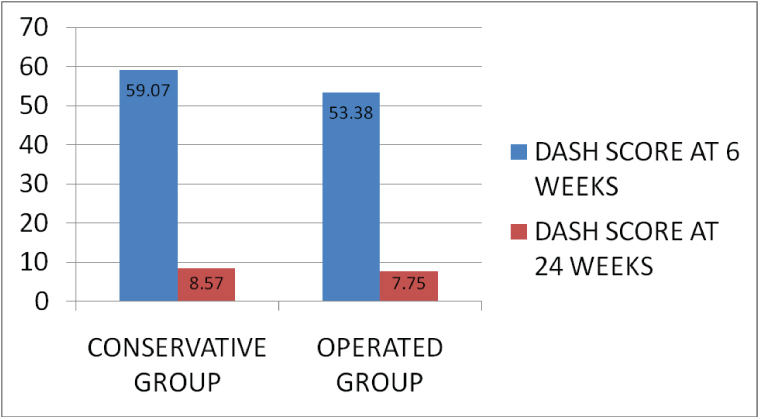
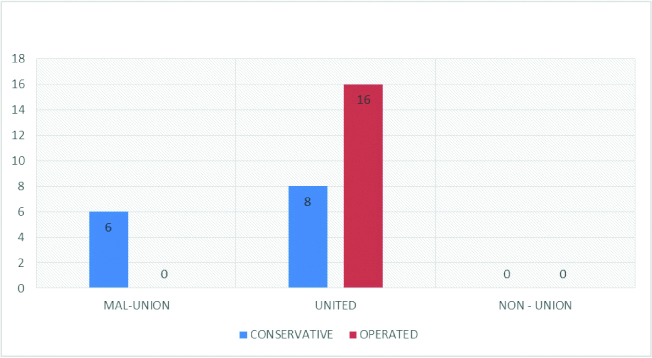
Road traffic accidents and fall were the main aetiologies of clavicle fractures in our patients. Between 25-35 years was the interval of age group that included majority of the patients with clavicle fractures. Twenty five of the 30 patients were males. Hence, there was more of a male predisposition of these injuries. At six weeks the DASH score was noted to be 59.07+11.99 points for the conservative group and 53.38+14.435 points for the operated group, with a significant p-value (0.254). During the final review at 24 weeks, the DASH score was noted to be 8.57+/-6.073 points for the conservative group and 7.75+16.422 points for the operated group, with a significant p-value (0.861) [Table/Fig-5]. Six of the 14 patients of the conservative management group were noted to have mal-union of the fracture at 24 weeks; none of the patients in the operated group had mal-union as a complication. None of the patients had non-union as a complication [Table/Fig-6]. No other complications were noted.
Bar graph showing the DASH score of the patient’s shoulder function in the conservative and operative group during the review at six weeks and 24 weeks.
Bar graphs representing the complication rate at 24 weeks post-op.
Discussion
The studies of Neer CS and Rowe CR in the 1960s suggested that conservative management of mid-shaft clavicle fractures to be included under the spectrum of non-operative management [4,5]. The functional outcome was defined to be complete regardless of the fracture pattern and displacement [4,5]. They considered conservative management to be satisfactory as their study population included a large number of adolescents. Also, in this population, the remodelling of clavicle can occur due to late closure of diaphysis. Mal-union can be one of the causes for reduction in shoulder movement [2]. Robinson CM noted four risk factors for mal-union and non-unions to occur: age, female gender, displacement more than one clavicular shaft width, comminution [1]. Results of Pandya MK and colleagues stressed on maintanance of clavicular length. Higher incidence of pain was reported in cases with shortening more than 15 mm [21]. Mal-unions and non-unions predispose to several static changes which can be noted such as decreased strength, elevated sternocostal angle, opening of glenohumeral joint which can worsen the shearing forces on the anterior glenoid and labrum and eventual shortening of lever arm and muscles of the shoulder girdle [3].
Majority of the patients in our series were males (83.3%) and rest were females (16.7%). The age group which was affected maximum was between 25-35 years. These results were comparable to the results of Bostman O et al., where average age under study was 33.4 years and 73.9% were male and 26.21% were females [22]. On comparison of the DASH scores during the final review no significant difference in the DASH scores was noted between the two groups. This inferred that there was no significant difference in the outcome of shoulder function between the two techniques. These results were comparable to those of Virtanen KJ et al., who reported no significant difference between the functional outcome of the conservative and operative group in their series [10]. Six of the 14 patients reported mal-union as a complication during the final review in the conservative group, no mal-union was noted in the operated group. No non-unions were noted in either of the groups. These results were comparable to those of Robinson CM who reported a displaced mal-union and non-union in 19-33% of his cases [1]. Robinson CM also reported saying an escalation in the rate of mal-unions and non-unions to 33-47% in case of a comminuted fracture [1].
Virtanen KJ et al., in their series of 60 patients of whom 32 patients were managed conservatively and 28 patients underwent open reduction and plate fixation, they concluded that the rate of non-union was higher with the conservative group but the outcome of shoulder function was same as the operated group [10].
Brin and colleagues reported that operative fixation was preferred over non-operative management for clavicular fractures, mainly open reduction and locking plate fixation by majority of the trauma surgeons [2].
McKee RC and colleagues reported significantly lower rates of mal-union and non-union in the patients who were operated as compared to the patients who underwent conservative management [23].
Limitation
The sample size of the study was small. Most of our cases were from distant places and hence, did not appear for the first follow up and hence, had to be excluded from the study. The follow up was done only till 24 weeks, as many patients could not be followed up beyond 24 weeks.
Conclusion
The outcome of shoulder function after management by conservative technique of mid-shaft fractures of clavicle do not show significant difference from the outcomes after operative intervention of open reduction and locking plate fixation. However, the incidence of mal-union and non-union of clavicle fractures is noted to have diminished after operative intervention.
[1]. Robinson CM, Fractures of the clavicle in the adult. Epidemiology and classificationJ Bone Joint Surg Br 1998 80:476-84. [Google Scholar]
[2]. Brin YS, Palmanovich E, Dolev E, Nyska M, Kish BJ, Displaced mid-shaft clavicular fractures: Is conservative treatment still preferred?Isr Med Assoc J 2014 16(12):748-52. [Google Scholar]
[3]. Ledger M, Leeks N, Ackland T, Wang A, Short mal-unions of the clavicle: An anatomic and functional studyJ Shoulder Elbow Surg 2005 14(4):349-54. [Google Scholar]
[4]. Neer CS, Nonunion of the clavicleJAMA 1960 172:1006-11. [Google Scholar]
[5]. Rowe CR, An atlas of anatomy and treatment of midclavicular fracturesClin Orthop Relat Res 1968 58:29-42. [Google Scholar]
[6]. McKee MD, Pedersen EM, Jones C, Stephen DJ, Kreder HJ, Schemitsch EH, Deficits following nonoperative treatment of displaced midshaft clavicular fracturesJ Bone Joint Surg Am 2006 88(1):35-40. [Google Scholar]
[7]. Nowak J, Holgersson M, Larsson S, Sequelae from clavicular fractures are common: A prospective study of 222 patientsActa Orthop 2005 76:496-502. [Google Scholar]
[8]. Rehn CH, Kirkegaard M, Viberg B, Larsen MS, Operative versus nonoperative treatment of displaced midshaft clavicle fractures in adults: A systematic reviewEur J Orthop Surg Traumatol 2014 24(7):1047-53. [Google Scholar]
[9]. Robinson CM, Goudie EB, Murray IR, Jenkins PJ, Ahktar MA, Read EO, Open reduction and plate fixation versus nonoperative treatment for displaced midshaft clavicular fractures: A multicenter, randomized, controlled trialJ Bone Joint Surg Am 2013 95(17):1576-84. [Google Scholar]
[10]. Virtanen KJ, Remes V, Pajarinen J, Savolaines V, Bjokenheim MJ, Paavola M, Sling compared with plate osteosynthesis for treatment of displaced midshaft clavicular fractures: a randomized clinical trialJ Bone Joint Surg Am 2012 94(17):1546-53. [Google Scholar]
[11]. Xu CP, Li X, Cui Z, Diao XC, Yu B, Should displaced midshaft clavicular fractures be treated surgically? A meta-analysis based on current evidenceEur J Orthop Surg Traumatol 2013 23(6):621-29. [Google Scholar]
[12]. Inman VT, Saunders JB, Observations on the function of the clavicleCalif Med 1946 65(4):158-66. [Google Scholar]
[13]. Hill JM, Mcguire MH, Closed treatment of displaced middle-third fractures of the clavicle gives poor resultsJ Bone Joint Surg Br 1997 79:537-39. [Google Scholar]
[14]. Wenninger JJ, Dannenbaum JH, Branstetter JG, Arrington ED, Comparison of complication rates of intramedullary pin fixation versus plating of midshaft clavicle fractures in an active duty military populationJ Surg Orthop Adv 2013 22(1):77-81. [Google Scholar]
[15]. Poigenfurst J, Rappold G, Fischer W, Plating of fresh clavicular fractures: Results of 122 operationsInjury 1992 23:237-41. [Google Scholar]
[16]. McKee MD, Seiler JG, Jupiter JB, The application of the limited contact dynamic compression plate in the upper extremity: An analysis of 114 consecutive casesInjury 1995 26:661-66. [Google Scholar]
[17]. Mueller M, Burger C, Florczyk A, Elastic stable intramedullary nailing of midclavicular fractures in adults: 32 patients followed for 1-5 yearsActa Orthop 2007 78:421-23. [Google Scholar]
[18]. Perez AE, Fractures of the shoulder, arm and forearmCampbell’s Operative OrthopaedicsVol IIIEd 12:2832 [Google Scholar]
[19]. Semkal V, Oberladstaetter J, Sturve P, Krappinger D, Shaft fractures of the clavicle: current conceptsArch Orthop Trauma Surg 2009 129:807-15. [Google Scholar]
[20]. Hudak PL, Amadio PC, Bombardier C, Development of an upper extremity outcome measure: The DASH (disabilities of the arm, shoulder and hand)Am J Ind Med 1996 29(6):602-08.Erratum in: Am J Ind Med 1996:30;3-372 [Google Scholar]
[21]. Pandya NK, Namdari S, Hosalkar HS, Displaced clavicle fractures in adolescents: Facts, controversies, and current trendsJ Am Acad Orthop Surg 2012 20(8):498-505. [Google Scholar]
[22]. Bostman O, Manninen M, Pihlajamaki H, Complications of plate fixation in fresh displaced mid clavicular fracturesJ Trauma 1997 43:778-83. [Google Scholar]
[23]. McKee RC, Whelan DB, Schemitsch EH, McKee MD, Operative versus nonoperative care of displaced midshaft clavicular fractures: A meta-analysis of randomized clinical trialsJ Bone Joint Surg Am 2012 94(8):675-84. [Google Scholar]