Post-Caesarean Drain Placement - Minor Procedure Leading to Major Complication
Richa Sharma1, Kiran Guleria2, Amita Suneja3, Vishnu Bhartiya4
1 Assistant Professor, Department of Obstetrics and Gynaecology, University College of Medical Sciences and Guru Teg Bahadur Hospital, Delhi, India.
2 Director and Professor, Department of Obstetrics and Gynaecology, University College of Medical Sciences and Guru Teg Bahadur Hospital, Delhi, India.
3 Director and Professor, Department of Obstetrics and Gynaecology, University College of Medical Sciences and Guru Teg Bahadur Hospital, Delhi, India.
4 Assistant Professor, Department of Obstetrics and Gynaecology, University College of Medical Sciences and Guru Teg Bahadur Hospital, Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Vishnu Bhartiya, Assistant Professor, Department of Obstetrics and Gynecology, University College of Medical Sciences and Guru Teg Bahadur Hospital, Dilshad Garden, Delhi, India.
E-mail: vishnubhartiya99@gmail.com
Intra abdominal drain insertion in doubtful cases has been practised since many years. It may be associated with certain minor as well as major complications like drain site haemorrhage, infection, intestinal perforation and even visceral herniation from the site.
Herein, we report a case of 28-year-old unbooked G2P1L1 at 33 weeks gestation with previous caesarean, who underwent Lower Segment Caesarean Section (LSCS) in view of breech presentation in labour. On sixth postoperative day, tubular structure herniation through the drain site was observed. She was undertaken for laparotomy and fallopian tube herniation through the drain site was confirmed. Ipsilateral salpingectomy was done. Thus, drain placement lead to prolonged hospital stay and maternal morbidity.
Postpartum morbidity, Prophylactic drain, Tubal herniation
Case Report
A 28-year-old unbooked G2P1L1 at 33 weeks gestation, presented to the gynaecology casualty of our institution with complaints of leaking per vaginum for eight hours. Previous caesarean was done three years back at 30 weeks gestation for breech presentation in active labour. Two years back she was diagnosed having hypertension and now with superimposed pre-eclampsia, which was controlled on Tablet Methyldopa 250 mg QID since one month.
On examination her pulse was 90/min, BP 142/88 mmHg and live foetus in transverse lie position not in labour. Patient was taken up for caesarean section in view of previous LSCS with transverse lie position, after steroid coverage. A live male baby of weight 2 kg was born with Apgar score 7/10 and 9/10 and was shifted to NICU in view of prematurity. Intraoperatively, lot of adhesions were present and dissections were done between rectus muscles, parietal peritoneum and anterior abdominal wall, which kept on oozing despite haemostat application. Penrose drain no 32FG was inserted from a separate incision in left iliac fossa and placed intraperitoneally in pouch of douglas.
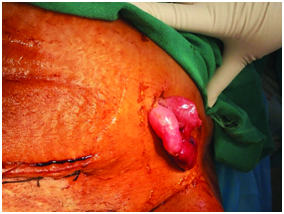
Drain was removed on day 3 and she developed mild cough on postoperative day 4. On day 6, bleeding at the drain site along with 3 cm of reddish-pink coloured oedematous, swollen and tip necrosed tubular structure was observed coming out through the drain site [Table/Fig-1]. It was strangulated and non-reducible. Her bowel and bladder habits were normal.
Tubular structure herniating from drain site.
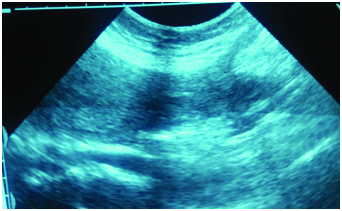
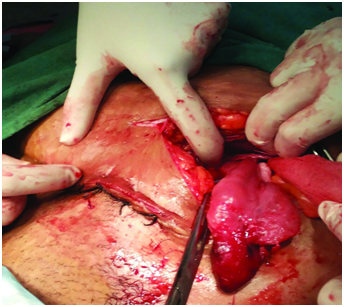
Transabdominal ultrasonogram was suggestive of fallopian tube herniation [Table/Fig-2]. Patient was taken up for emergency laprotomy, incision of 4 cm was made at the drain site, structures were explored and the fallopian tube herniation was observed [Table/Fig-3]. Left sided salpingectomy was done and the histopathological examination also confirmed the diagnosis.
Transabdominal ultrasonogram shows fallopian tube herniation.
Intraoperative picture showing left side tube and ovary.
She was discharged on fifth postoperative day following laparotomy with a healthy baby. Her duration of hospital stay was 11 days. Both were followed up after one month and found to be healthy.
Discussion
Prophylactic drainage following routine abdominal surgery continues to be a controversial subject. The dictum when in doubt put the drain is well known to most surgeons. Drain insertion may be associated with haemorrhage from abdominal wall vessels, sepsis, kinking and knotting of drains requiring operative removal, fistulae formation, intestinal obstruction or erosion into adjacent structures with peritonitis, incisional hernia [1]. But very few cases regarding postcaesarean fallopian tube herniation through the drain site have been reported [2,3]. Review of literature has documented fallopian tube as a content of hernia sac (inguinal and femoral hernia) [4] and post hysterectomy herniation of fallopian tube (abdominal and vaginal) [5]. There are also reports of herniation of intestine [6], appendix [7], omentum [8], gall bladder [9] and ovary [10] from surgical drain site. Hernias through drain site usually occur 3–8 hour after drain removal. Predisposing factors include general debility, poor nutritional status, obesity, increased intra-abdominal pressure (constipation, cough, vomiting), co-morbidities (e.g., diabetes mellitus), steroid therapy that further delays wound healing and fibrosis, and the stab incisions for drains which had external diameters of more than 1 cm [11]. In the present case, it occurred after 72 hours of drain removal and the risk factors could have been upper respiratory tract infection and betamethasone therapy which was given for the foetal lung maturity.
The risk of this complication could be minimized by the use of smaller bore drainage systems measuring less than 10 mm in diameter, a ‘Z’ (nonsymmetric) insertion method, a purse string suture for closure of the site after removal and a gradual removal of the drain [11]. If a stab incision is to be made, it should be made obliquely and not reach the peritoneum so that the latter is stretched as the drain is inserted. In present case 32FG drain was used, which was available in our hospital. Though drain removal was gradual and tincture iodine was applied after it, patient developed tubal evisceration leading to unnecessary maternal morbidity.
Conclusion
Complications are known to occur with the use of drains, no drainage at all is better than the ignorant employment of it. Proper selection of size, technique of intraperitoneal drain insertion and gradual removal of the drain followed by purse string suture for closure of the site could greatly avoid untoward morbidity.
[1]. Mosley JG, Jantet G, Herniation at the site of an abdominal drainBr J Clin Pract 1978 32(2):56-58. [Google Scholar]
[2]. Sharma L, Singh A, Bhaskaran S, Radhika AG, Radhakrishnan G, Fallopian tube herniation: An unusual complication of surgical drainCase Rep Obstet Gynecol 2012 2012:194350 [Google Scholar]
[3]. Saini P, Faridi MS, Agarwal N, Gupta A, Kaur N, Drain site evisceration of fallopian tube, another reason to discourage abdominal drain: Report of a case and brief review of literatureTrop Doct 2012 42:122-24. [Google Scholar]
[4]. Ozkan OV, Semerci E, Aslan E, Ozkan S, Dolapcioglu K, Besirov E, A right sliding indirect inguinal hernia containing paraovarian cyst, fallopian tube, and ovary: A case reportArch Gynecol Obstet 2009 279(6):897-99. [Google Scholar]
[5]. Candiani GB, Candiani M, Posthysterectomy fallopian tube herniation. A report of two casesJ Reprod Med 1996 41(12):915-20. [Google Scholar]
[6]. Kulkarni S, Krijgsman B, Sharma D, Kaisary AV, Incarcerated small bowel hernia through drain siteAnn R Coll Surg Engl 2004 86(6):W24-25. [Google Scholar]
[7]. Gass M, Zynamon A, von Flüe M, Peterli R, Drain-site hernia containing the vermiform appendix: Report of a caseCase Rep Surg 2013 2013:19 [Google Scholar]
[8]. Howard FM, Sweeney TR, Omental herniation after operative laparoscopy. A case reportJ Reprod Med 1994 39(5):415-16. [Google Scholar]
[9]. Vedat B, Aziz S, Cetin K, Evisceration of gallbladder at the site of a Pezzer drain: A case reportCases J 2009 2:8601 [Google Scholar]
[10]. Pianon P, Lise M, Exteriorization of an ovary: An unusual complication of abdominal drainageBr J Surg 1992 79(9):963 [Google Scholar]
[11]. Falidas E, Mathioulakis S, Vlachos K, Pavlakis E, Villias C, Strangulated intestinal hernia through a drain siteInt J Surg Case Rep 2012 3(1):1-2. [Google Scholar]