Triple Synchronous Malignancies in Genital Tract; Primary Endometrial, Ovarian and Fallopian Tube Carcinoma: A Case Report
Ozgur Kan1, Aysegul Alkilic2, Batuhan Turgay3, Ali Gemici4, Cem Somer Atabekoglu5
1 Specialist, Department of Obstetrics and Gynaecology, Etlik Zubeyde Hanim Women’s Health Hospital, Ankara, Turkey.
2 Specialist, Diyadin State Hospital, Agri, Turkey.
3 Resident, Department of Obstetrics and Gynaecology, Ankara University School of Medicine, Ankara, Turkey.
4 Specialist, Department of Obstetrics and Gynaecology, Etlik Zubeyde Hanim Women’s Health Hospital, Ankara, Turkey.
5 Professor, Department of Obstetrics and Gynaecology, Ankara University School of Medicine, Ankara, Turkey.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ozgur Kan, Etlik Zubeyde Hanim Women’s Health Hospital, Etlik, Yeni Etlik Caddesi No:55, 06010, Ankara, TR.
E-mail: drozgurkan@gmail.com
Synchronous malignancies, including three or more tumours, are extremely rare. Herein, we present a case of a woman with a concurrent simultaneous endometrial, ovarian and fallopian tubal carcinoma with different histopathological characteristics. A 55-year-old postmenopausal woman with a diagnosis of endometrial adenocarcinoma by pipelle biopsy, underwent surgical staging. Final pathology result was reported as synchronous stage IA grade 2 endometrioid adenocarcinoma of the uterus, stage IA grade 2 mucinous adenocarcinoma of the right ovary and in situ serous cystadenocarcinoma of the right fallopian tube. In the postoperative period, patient followed without adjuvant therapy. To our knowledge, this a very rare case report in the literature of sychronous triple gynaecologic cancers including fallopian tube cancer and with the longest disease free survival time with over 39 months due to better prognosis than metastatic or advanced primitive diseases.
Different primaries, Synchronous tumours, Triple cancers
Case Report
A 55-year-old, G3P3, postmenopausal woman was presented to her primary care provider with a complaint of postmenopausal haemorrhage. Her body mass index was 27.3 kg/m2. Her personal and family history was unremarkable. Initial pelvic ultrasonography examination had revealed 13 mm endometrial thickness and a 45x41 mm measured adnexal mass in the right side and endometrial biopsy was planned in the primary clinic. The histopathological diagnosis of the endometrial biopsy was reported as adenocarcinoma of endometrium. After this result, patient was referred to our tertiary clinic for detailed examination and further treatment.
Her physical examination and vital findings were normal. Pelvic examination was normal and no palpable masses were noticed. Transvaginal Ultrasonogram (TVUSG) showed slight thickening of the endometrium and heterogeneous mass located in the right adnexal area (53x42 mm) containing multiple foci of calcification and thin septas. Computerized Tomography (CT) scan revealed a 57x48 mm right adnexial mass [Table/Fig-1] and neither adenopathies nor other significant findings were found in the remainder of the abdomen. Tumour markers were within the normal range (CA-125: 18.3 IU/ml).
CT image of the right adnexal mass.

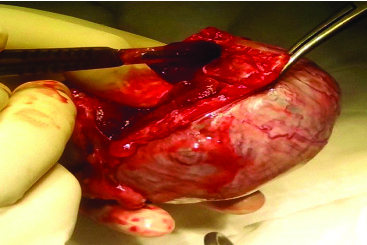
Under a diagnosis of endometrial adenocarcinoma, debulking surgery was planned. Following peritoneal washing sampling, indeterminate right adnexal mass was visualized and unilateral salpingo-oophorectomy performed and specimen sent to frozen section examination [Table/Fig-2]. Intraoperative pathological findings resulted as mucinous adenocarcinoma of the ovary. Then, total abdominal hysterectomy, contralateral salpingo-oophorectomy, bilateral pelvic and para-aortic lymph node dissection, total omentectomy and appendectomy were performed.
Macroscopic view of the right oophorectomy specimen.
Final pathology result was reported as synchronous stage IA grade 2 endometrioid adenocarcinoma of the uterus, stage IA grade 2 mucinous adenocarcinoma of the right ovary and in situ serous cystadenocarcinoma of the right fallopian tube. Uterine corpus specimen was reported with minimal myometrial invasion and neither squamous differentiation nor lymphovascular invasion was seen. There was no tumour on the surface of the right oophorectomy specimen and also peritoneal washing sample, appendix and omental biopsies were negative. A total of 33 lymph nodes were evaluated and all were reported as negative. All of the three tumours were accepted as different primaries due to final pathologic evaluation.
In the postoperative period, patient was discharged and referred to the medical oncology council and they did not suggest any adjuvant therapy. In the follow up stage, CT scans and gynaecologic exams showed no evidence of disease and routine mammographies excluded breast diseases.
Discussion
Synchronous malignancies in female genital tract are rare. Previous authors have reported synchronous malignancy incidence among gynaecologic neoplasms between 0.8% and 1.7% [1,2]. The most common malignancies in genital tract that coexist together are ovary and endometrium. A 5% of the endometrial carcinomas and 10% of the ovarian cancers are concurrent with each other [3]. The aetiology of this coexistence is still unclear, but, it has been postulated that tissues of a common embryologic origin may develop synchronous neoplasms when simultaneously exposed to certain carcinogens [4,5].
Surgical staging is the fundamental of treatment of the patients with synchronous malignancies. It must be proved whether a primary or a metastatic tumour with the pathological examination criteria described by Ulbright T and Roth L at the first place [6]. According to these, the tumours must have different histopathology or fulfill all the minor criteria. The minor criteria are: all the tumours must be restricted, no distant metastasis, no connection between the tumours, no lenfovascular tumour embolus and no myometrial invasion. In this case, a surgical staging was performed and eventually the diagnosis was synchronous malignancy due to the different histopathology of all the tumours.
Patients with synchronous malignancies have a better outcome than the patients who have metastatic diseases in the same organs [7,8]. Owing to early detection, opportunity in combination with endometrial carcinomas have better survival rates than the patients with malignancies of ovaries [9]. In this case, postmenopausal haemorrhage complaint of the patient generated a chance to early diagnosis. Because of this fact, severe invasion and metastasis risk excluded and no postoperative therapy suggested for the patient. There was no recurrence observed after 39 months from operation.
There is no high-quality evidence that any specific post-treatment surveillance strategy is associated with improved outcomes for synchronous tumours in genital tract. In the absence of data, we agree with the consensus-based guidelines from the United States National Comprehensive Cancer Network (NCCN) for both ovarian and endometrial cancers [10,11]. According to these guidelines, follow up visits (including history, general physical and pelvic examinations) were performed every three months up to five years after surgery. Despite there is no clear impact of serial Ca-125 measurements on overall survival, tumour marker measurements were taken every three months.
Primary fallopian tube carcinomas are rare malignancies of the genital tract and the incidence was reported 0.41 in 100000 women [12]. There are reported four cases with multiple coexisting malignancies include fallopian tube carcinomas in the literature and this case is the fifth one to our knowledge. The characteristics of the all five cases are given in [Table/Fig-3] [13–16].
Features of multiple synchronous gynaecologic malignancies including fallopian tubal carcinoma reports in the literature [13–16].
| Reference | Age | Anatomic Site | Tumour histology | Outcome follow-up |
|---|
| Saglam Aet al., [13] | 63 | SalpinxOvaryEndometriumCervix | Papillary Adenoca.Mucinous Adenoca.Adenoca.Endocervical Adenoca. | NED 12 months |
| Atasever Met al., [14] | 50 | SalpinxOvaryEndometriumCervix | Microinvasive carcinoma in situPapillary Serous Adenoca.Intraepithelial Adenoca.Endocervical carcinoma in situ | DOD29 months |
| Kambi DPet al., [15] | 55 | SalpinxOvaryCervix | Papillary Cystadenoca.Papillary Cystadenoca.Adenosquamous carcinoma | N/A |
| Gutierrez-Palomino Let al., [16] | 49 | SalpinxOvaryEndometrium | Endometrioid Adenoca.Endometrioid Adenoca.Adenoca. | Adjuvant therapy, survival N/A |
| Present study | 55 | SalpinxOvaryEndometrium | Serous Cystadenoca. in situMucinous Adenoca.Adenoca | DFS39 months |
Adenoca.: adenocarcinoma, DOD: died of disease, NED: no evidence of disease DFS: disease free
Genetic transition must be considered in synchronous malignancies. Especially women with mutation of the BRCA-1 and BRCA-2 have improved risk for malignancies of fallopian tubes and ovaries [17]. Lynch syndrome is other condition has to be taken into account because of the risk for the ovarian malignancy development due to the mutation of the mismatch-repair genes [18]. Synchronous tumours are associated with these genetic mutations.
Conclusion
Triple synchronous malignancies in genital tract are extremely rare and distinct from the most of the previous cases, one of the primaries are originated from fallopian tubes, the different histopathology of all the tumours and 39 months of disease free survival in the follow up period is the value of this case report.
Adenoca.: adenocarcinoma, DOD: died of disease, NED: no evidence of disease DFS: disease free
[1]. Ayhan A, Yalcin OT, Tuncer ZS, Gurgan T, Kucukali T, Synchronous primary malignancies of the female genital tractEur J Obset Gynaecol Reprod Biol 1992 45:63-66. [Google Scholar]
[2]. Tong SY, Lee YS, Park JS, Bae SN, Lee JM, Namkoong SE, Clinical analysis of synchronous primary neoplasms of the female reproductive tractEur J Obstet Gynaecol Reprod Biol 2008 136:78-82. [Google Scholar]
[3]. Zaino R, Whitney C, Brady MF, DeGeest K, Burger RA, Buller RE, Simultaneously detected endometrial and ovarian carcinomas–A prospective clinicopathologic study of 74 cases: A gynaecologic oncology group studyGynaecol Oncol 2001 83:355-62. [Google Scholar]
[4]. Woodruff JD, Solomon D, Sullivant H, Multifocal disease in the upper genital canalObstet Gynaecol 1985 65:695-98. [Google Scholar]
[5]. Takatori E, Shoji T, Miura Y, Takeuchi S, Uesugi N, Sugiyama T, Triple simultaneous primary invasive gynaecological malignancies: A case reportJ Obstet Gynaecol Res 2014 40:627-31. [Google Scholar]
[6]. Ulbright T, Roth L, Metastatic and independent cancers of the endometrium and ovary: A clinicopathologic study of 34 casesHum Pathol 1985 16:28-34. [Google Scholar]
[7]. Williams MG, Bandera EV, Demissie K, Rodríguez-Rodríguez L, Synchronous primary ovarian and endometrial cancers: A population-based assessment of survivalObstet Gynaecol 2009 113(4):783-89. [Google Scholar]
[8]. Chiang YC, Chen CA, Huang CY, Hsieh CY, Cheng WF, Synchronous primary cancers of the endometrium and ovaryInt J Gynaecol Cancer 2008 18:159-64. [Google Scholar]
[9]. Chiofalo B, Di Giuseppe J, Alessandrini L, Perin T, Giorda G, Canzonieri V, Triple synchronous invasive malignancies of the female genital tract in a patient with a history of leukemia: A case report and review of the literaturePathol Res Practice 2016 212:573-77. [Google Scholar]
[10]. Phippen NT, Barnett JC, Lowery WJ, Miller CR, Surgical outcomes and national comprehensive cancer network compliance in advanced ovarian cancer surgery in a low volume military treatment facilityGynaecol Oncol 2013 131(1):158-62. [Google Scholar]
[11]. Morgan RJ, Ovarian Cancer, Version 1.2016, NCCN Clinical Practice Guidelines in OncologyJ Natl Compr Canc Netw 2016 14(9):1134-63. [Google Scholar]
[12]. Stewart SL, Wike JM, Foster SL, Michaud F, The incidence of primary fallopian tube cancer in the United StatesGynaecol Oncol 2007 107(3):392-97. [Google Scholar]
[13]. Saglam A, Bozdag G, Kuzey GM, Kuçukali T, Ayhan A, Four synchronous female genital malignancies: The ovary, cervix, endometrium and fallopian tubeArch Gynaecol Obstet 2008 277:557-62. [Google Scholar]
[14]. Atasever M, Yilmaz B, Dilek G, Akcay EY, Kelekci S, Synchronous primary carcinoma in 5 different organs of a female genital tract: an unusual case and review of the literatureInt J Gynaecol Cancer 2009 19:802-07. [Google Scholar]
[15]. Kambi DP, Mallikarjuna M, Santosh C, Abhishek V, Synchronous malignancies of ovary, fallopian tube and cervix: A rare caseInternational Journal of Biochemical and Advance Research 2013 4(9):676-79. [Google Scholar]
[16]. Gutiérrez-Palomino L, Reyes JMR, Pareja-Megía MJ, García-Mejido JA, Triple synchronous primary gynaecological tumours. A case reportCirugía y Cirujanos (English Edition) 2016 84(1):69-72. [Google Scholar]
[17]. Chen S, Parmigiani G, Meta-analysis of BRCA1 and BRCA2 penetranceJ Clin Oncol 2007 25(11):1329-33. [Google Scholar]
[18]. Dunlop MG, Farrington SM, Carothers AD, Wyllie AH, Sharp L, Burn J, Cancer risk associated with germline DNA mismatch repair gene mutationsHum Mol Genet 1997 10:105-10. [Google Scholar]