The restoration of normal jaw function, optimal facial aesthetics and long term stability are the goals of any orthognathic surgical procedures [1]. Superior repositioning of the maxilla is indicated in the treatment of the long face deformities with or without anterior open bite [2]. The maxilla is the focus of surgical treatment in long face patients for two major reasons. First, the maxilla nearly always has excessive vertical development, whereas the mandible may not be involved. Second, moving the maxilla up produces a stable surgical correction [2].
The stability of the orthognathic surgical procedures has been the subject of numerous publications in the recent years. The direction of surgical movement affects the total stability and predictability of any orthognathic surgical procedure [3,4]. According to Proffit WR, in the hierarchy of stability, the most stable orthognathic surgical procedure is the superior repositioning of the maxilla. Following superior repositioning of the maxilla, the postural rest position of the mandible rotates upwards and forwards maintaining the inter occlusal rest space. This physiological adaptation undoubtedly plays a major role in the stability [5].
Though various methods have been used in literature to assess cranio-facial deformities and respective treatment out-come i.e. computed tomograms, cephalograms, Magnetic Resonance Imaging (MRI), lateral cephalogram and panoramic films are still being used widely due to its, low radiation, universal acceptibility, economical factor and easy avaliability [6,7]. During the last two decades, several cephalometric investigations have been reported on the skeletal changes following maxillary surgical procedure with or without orthodontic treatment. Many studies have been conducted in the past highlighting the efficiency and the stability of the orthognathic surgical procedures [8–11].
Stability of any surgical procedure when studied, the maximum changes have been noted in the initial one year hence forth the following observation can be considered as a valuable observation to further our knowledge. Therefore, an attempt was made to study the skeletal and dental stability in patients who underwent superior repositioning of the maxilla via Le Fort I osteotomy by means of downward fracture technique with or without concurrent mandibular procedure after a span of one year following surgery.
Materials and Methods
Subjects: A retrospective cross sectional study had been planned after departmental permission as work of post graduate dissertation. Presurgical, postsurgical and one year postsurgical lateral cephalograms of 10 adult patients who had been treated successfully at the Department of Orthodontics and Dentofacial Orthopedics, Bapuji Dental College and Hospital, Davangere, Karnataka India. from 2006 to 2009 were obtained. The age group of these patients ranged from 17 to 40 years, with a mean age of 22.2 years. All the patients used in the study were treated by a pre-adjusted Edgewise appliance for presurgical orthodontics with or without extractions. Six out of ten patients had undergone upper and lower first premolars extraction, for correction of decompensations and ideal positioning of teeth before surgey to provide stable occlusion postsurgically. Le Fort 1 down-fracture with vertical reduction in the maxilla was carried out in all the subjects.
The primary selection criterions were: (1) Non growing patients diagnosed for vertical maxillary excess with or without an anterior open bite; (2) All the patients were treated by Le Fort I osteotomy, maxillary superior repositioning osteotomy, rigid fixation and with or without concurrent mandibular procedures (BSSO advancement or genioplasty); (3) No concomitant or previous nasal surgery; (4) No history of any congenital deformities and/or a genetic syndrome or whose deformities were related to trauma or disease. Presurgical, Immediate postsurgical and one year postsurgical lateral cephalograms were taken by standardized technique with teeth in occlusion and lips relaxed. The lateral cephalograms of the ten patients considered for the study were grouped into three categories.
T1- Presurgical
T2- Postsurgical
T3- One year postsurgical
Comparisons were made between T1-T2 and T2-T3 to assess the changes following surgery and to evaluate the stability, one year following the surgery using 5 horizontal, 5 vertical linear and 2 angular measurement [Table/Fig-1,2 and 3].
Hard tissue vertical changes.
Hard tissue horizontal changes.
Hard tissue angular changes.
Data Acquisition: Profile cephalograms were taken in occlusion under standardized conditions with a cephalostat. Cephalometric landmarks were traced on 0.003 inch matte acetate paper with a 0.3 mm HB lead pencil.
Measurements: Angular measurements were recorded to a nearest of 0.5 degrees and linear measurements to the nearest 0.5 mm. Linear and angular parameters for hard tissue evaluation were used as illustrated in [Table/Fig-1,3]. The analysis includes certain linear and angular measurements of Burstone’s hard tissue, Steiner’s and Rakosi Jaraback analysis, which were easily applicable for the study. All the measurements were repeated twice with two observer to rule out any intraobserver variability [12,13].
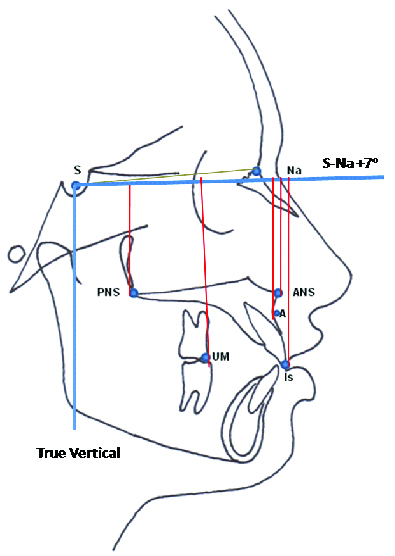
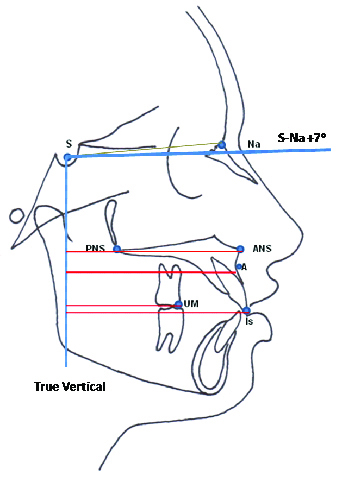
Constructed Reference Lines [Table/Fig-1,2]:
Horizontal Reference Line (HRL): Sella-Nasion + 7o; A horizontal reference line was registered on Sella (S) and oriented 7° inferior to the SN line.
True Vertical Line (TVL): TVL was perpendicular to the horizontal reference plane that passes through Sella (S).
Linear Parameters For Hard Tissue Evaluation [Table/Fig-1,2]:
A point horizontal: the horizontal distance between point A and TVL.
A point vertical: the vertical distance between point A and HRL
ANS horizontal: the horizontal distance between point ANS and TVL.
ANS point vertical: the vertical distance between point ANS and HRL.
PNS point horizontal: the horizontal distance between point PNS and TVL.
PNS point vertical: the vertical distance between point PNS and HRL.
Upper incisor horizontal: the horizontal distance between point Is and TVL.
Upper incisor vertical: the vertical distance between point Is and the HRL.
Upper 1st molar horizontal: the horizontal distance between mesio-buccal cusp of upper 1st molar (Um) and TVL.
Upper 1st molar vertical: the vertical distance between mesio-buccal cusp of upper 1st molar (Um) and the SN+7o line.
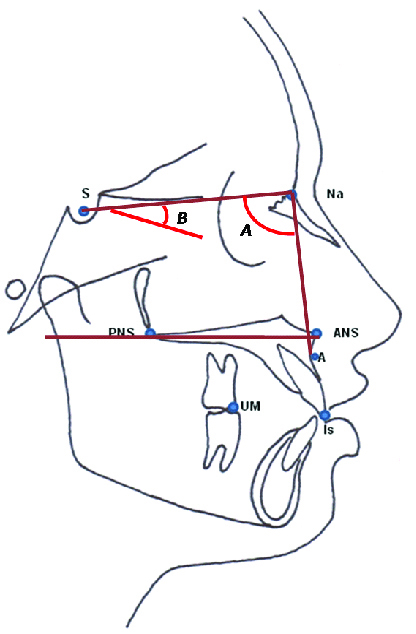
Angular Parameters For Hard Tissue Evaluation [Table/Fig-3]:
SNA Angle: It is the angle formed by the line drawn from sella-nasion to Point A. It relates the anteroposterior position of maxilla relative to anterior cranial base.
Palatal plane to SN: This is the angle formed between S-N Plane and palatal plane (ANS-PNS). It gives inclination of palatal plane to anterior cranial base.
Statistical analysis was done using Statistical Package of Social Science (SPSS Version 20; Chicago Inc., USA). Significance level was fixed at p<0.05. The Student’s t-test was used to analyze the variation in mean between two groups of a variable with a normal distribution [14].
Results
The mean difference in the variables from T1-T2 and T2-T3 were compared to assess the changes brought about by the surgery and its stability one year following the surgery. The inter and intra-observer reliability ranged from 0.75 to 0.90 and 0.84 to 0.99 respectively.
Changes from T1 to T2
The differences between mean presurgical value and mean postsurgical value of HRL to point A, HRL to point ANS, HRL to point PNS, HRL to point Is, HRL to point Um (p<0.001) showed that they were statistically highly significant [Table/Fig-4]
A remarkably significant reduction in the vertical maxillary height was noted. Major movements in the vertical plane occurred at the ANS, point A and upper incisors. The anterior maxilla moved more superiorly than the posterior maxilla. Significant post surgical vertical movements were also seen in the points PNS and upper molar but to a lesser extent when compared to the anterior maxillary points.
Maxillary incisors followed the skeletal landmark with an average superior movement of 7.8 mm postsurgically. The upper molars also moved superiorly by 5.1 mm postsurgically.
The differences between mean presurgical value and mean postsurgical value of TVL to point A, TVL to point PNS, TVL to point Is, TVL to point Um showed that they were statistically significant whereas, TVL to point ANS was not statistically significant. Point A moved anteriorly at an average of 2.7 mm. The posterior maxilla movement also followed the anterior maxilla with a recorded average of 1.9 mm. Maxillary incisors moved anteriorly at an average of 2.8 mm and the upper molars moved at an average of 5.5 mm [Table/Fig-5].
| | T1 | T2 | T3 | T1-T2, p-value*, sig | T2-T3, p-value*, sig |
|---|
| A Point | Mean | 48.8 | 43.0 | 44.1 | 5.8 p<0.001 HS | -1.1, p=0.08 NS |
| SD | 2.5 | 1.8 | 2.3 |
| ANS Point | Mean | 45.1 | 39.7 | 40.6 | 5.4 p<0.001 HS | -0.9, p=0.09 NS |
| SD | 2.1 | 1.3 | 1.8 |
| PNS Point | Mean | 44.1 | 40.9 | 41.4 | 3.2 p=0.001 HS | -0.5, p=0.24 NS |
| SD | 4.1 | 4.7 | 3.8 |
| Upper Incisor | Mean | 79.9 | 72.1 | 73.3 | 7.8 p<0.001 HS | -1.2, p=0.20 NS |
| SD | 5.0 | 4.4 | 4.5 |
| Upper 1st Molar | Mean | 71.9 | 66.8 | 67.0 | 5.1 p=0.001 HS | -0.2, p=0.75 NS |
| SD | 5.3 | 3.3 | 4.5 |
*Student’s paired t test
| | T1 | T2 | T3 | T1-T2, p-value*, sig | T2-T3, p-value*, sig |
|---|
| A Point | Mean | 67.8 | 70.5 | 69.2 | -2.7, p=0.008 S | 1.3, p=0.19 NS |
| SD | 4.1 | 4.4 | 4.4 |
| ANS Point | Mean | 70.6 | 72.5 | 71.3 | -1.9, p=0.1 NS | 1.2, p=0.2 NS |
| SD | 3.6 | 3.9 | 3.7 |
| PNS Point | Mean | 18.6 | 21.2 | 19.7 | -2.6, p=0.02 S | 1.5, p=0.07 NS |
| SD | 3.5 | 3.3 | 3.3 |
| Upper Incisor | Mean | 74.8 | 77.6 | 74.6 | -2.8, p=0.003 S | 0.32, p=0.02 S |
| SD | 7.2 | 6.0 | 6.3 |
| Upper 1st Molar | Mean | 45.5 | 51.0 | 49.2 | -5.5, p=0.002 S | 1.8, p=0.07 NS |
| SD | 6.2 | 7.1 | 5.7 |
*Student’s paired t test
The differences between mean presurgical value and mean postsurgical value of SNA, SN to PP showed they were statistically significant [Table/Fig-6]. Post surgically the SNA increased to an average of 2.1 mm and the angle SN to PP reduced by an average of 2.5 mm.
| | T1 | T2 | T3 | T1-T2, p-value*, sig | T2-T3, p-value*, sig |
|---|
| SNA | Mean | 80.6 | 82.7 | 82.3 | -2.1, p=0.01 S | 0.4, p=0.74 NS |
| SD | 3.3 | 3.7 | 4.4 |
| SN to PP | Mean | 8.1 | 5.6 | 6.1 | 2.5, p=0.004 S | -0.5, p=0.49 NS |
| SD | 3.2 | 4.4 | 3.3 |
*Student’s paired t test
Changes from T2 and T3
The mean differences between Postsurgical mean value and One year post surgical mean value of HRL to point A, HRL to point ANS, HRL to point PNS, HRL to point Is, HRLto point Um showed that they were statistically non significant. There was a minimal postoperative movement of the maxilla, all the values changed in a range of 1 to 1.5 mm. The incisors extrusion was limited to an average of 1.2 mm and the molars showed a 0.2 mm movement.
The mean differences between Postsurgical mean value and one year post surgical mean value of TVL to point A, TVL to point ANS, TVL to point PNS, TVL to point Um showed that they were statistically not significant whereas, TVL to point Is was statistically significant approximately. 1 to 1.5 mm of posterior skeletal movement was seen at the anterior and posterior skeletal landmarks which was statistically insignificant. The upper incisor showed a significant posterior movement. The upper molar also showed a posterior movement but to a lesser extent when compared to the incisors.
The mean differences between Postsurgical mean value and One year postsurgical mean value of SNA, SN to PP showed that they were statistically not significant [Table/Fig-3].
Discussion
The stability of orthognathic surgical procedures has been the subject of numerous publications in the recent years. Literatures have shown that the direction of movement, type of fixation used and the surgical technique that was employed affects stability after surgical repositioning of the jaws [15].
This study was aimed at determining the surgical changes brought about by superior repositioning of the maxilla by Le Fort I osteotomy and evaluate the stability of the surgical procedure one year following surgery to assist the Orthodontist in determining of the efficacy of this treatment procedures.
The difference in the age group of the subjects and difference in the sexes were not considered relevant in this study. This was supported by the study conducted by Bishara, Chu and Jackobson wherein they have mentioned that the amount of surgical corrections is not necessarily related to difference in sample size between the sexes and the difference between younger (less than 20 years of age) and older patients were also not significant [16].
When the vertical maxillary proportions were compared from Pre surgical (T1) to Postsurgical (T2), a remarkably significant reduction in the vertical maxillary height was noted. Major movements in the vertical plane occurred at the ANS, point A and upper incisors. The anterior maxilla moved more superiorly than the posterior maxilla. These findings were supported by the findings of Schendel SA, Hiranaka DK, and Proffit WR et al., [1,2,5]. ANS and point A demonstrated the greatest amount of postoperative changes; the remodeling of the ANS made identification of A point difficult. Similar findings were noted by Schendel SA [1]. Significant post surgical vertical movements were also seen in the points PNS and upper molar but to a lesser extent when compared to the anterior maxillary points. The reason would have been the way the surgery was planned and executed.
Maxillary incisors followed the skeletal landmark with an average superior movement of 7.8 mm postsurgically. The upper molars also moved superiorly by 5.1 mm postsurgically. These findings were similar to the findings of Bishara SE, Chu JW and Jacobson JR [16]. They gave a possible explanation to the increased dental changes to be related to the forces acting on the teeth during fixation and tightening of the suspension wires attached to the orthodontic arch wires which may exert greater force on the dentition and may cause localized dental intrusion and therefore care should be taken to avoid “burying” the incisors beneath the lips as it moves superiorly after the surgical procedure.
The vertical maxillary proportions were compared between T2 and T3 found that there was a minimal postoperative movement of the maxilla which was statistically insignificant. These findings were generally consistent with the observations of previous investigators i.e. Hiranaka DK and Kelly JP [2]. Only 0.5 to 1.2 mm of relapse was noted through the posterior and anterior maxilla which was insignificant showing the excellent stability of the surgical procedure in the vertical plane.
The mean horizontal skeletal and dental dimensions of the maxilla from presurgical to postsurgical showed significant anterior movement of the maxilla. Similar findings were also observed by Bishara SE, Chu JW and Jacobson JR [16]. Such an anterior movement of the maxilla is often seen in maxillary impaction surgeries. This can be because of posterior surface of the maxilla is angulated superiorly and anteriorly. On superior repositioning, the maxilla follows the same anterior and superior angulated path, thus showing an anterosuperior movement. Many of the classical landmarks may be altered during and after surgical procedure. Bone remodeling during the initial healing may change their configuration even further giving the result of an anterior movement [17].
The postsurgical and One year postsurgical horizontal maxillary changes had shown a relapse ranging from 1.2 to 3 mm. Significant relapse values were noted only at the incisors. This can be because due to finishing orthodontic treatment presumably accounts for much of the post fixation dental changes. The incisors usually are retracted. This probably reflects the need to close some residual extraction spaces which are usually present in the maxilla. A similar insignificant posterior movement was noted by Schendel SA, Proffit WR and Bishara SE and associates [1,5,16].
Maxillary incisors moved anteriorly at an average of 2.8 mm and the upper molars moved at an average of 5.5 mm from T1 to T2. These findings again were similar to the finding of Bishara JE, Chu JW and Jacobson JR [16].
The T2 and T3 horizontal dental changes found that the upper incisor showed a significant posterior movement. The upper molar also showed a posterior movement but to a lesser extent when compared to the incisors but the changes in the molar position was insignificant. Similar findings were noted by Proffit WR and associates, which they explained by saying that, during finishing orthodontic treatment which presumably accounts for much of the post fixation dental changes, the incisors usually are retracted but the molars are less likely to move forward [5]. This probably reflects the need to close some residual extraction spaces which are usually present in the maxilla.
Postsurgically (T2), the SNA increased to an average of 2.1 mm and the angle SN to PP reduced by an average of 2.4 mm. These findings were similar to the findings noted by Ayoub AF et al., [18]. From T2 to T3, very minimal i.e. 0.4o to 0.5o decrease in the respective angles was recorded, which was statistically not significant thus justifying good stability of the angular changes brought about by the surgery.
Even though no mandibular changes were exclusively studied in this study, the observations made by Proffit WR et al., stated that no difference in the stability of the maxillary surgery was noted at any postsurgical time in patients who underwent genioplasty [5]. In the study done by Turvey TA et al., and Kai Forssel K et al., on maxillary superior repositioning and mandibular advancement stated that there was no effect on the stability of the superior repositioning of the maxilla, instead the stability of the mandibular advancement procedure improved following superior maxillary repositioning [15,19].
With the advent of better surgical devices and rigid fixation options such as mini plates, biodegradable fixation, osteosynthesis screw fixation and also the newer bone grafting techniques, stability following Le Fort I osteotomy and superior repositioning of the maxilla can be definitely graded as excellent in all the three dimensions. As with any study, there were limitations that must be discussed. Firstly, the parameters could be better identified and the changes be recorded more accurately in a three dimensional representation like Cone Beam Computed Tomography (CBCT). Some of the skeletal landmarks such as ANS and PNS undergo considerable changes in their morphology and remodeling during and following surgery and the orthodontic tooth initiated post surgically may have influenced the results to some extent [20].
Though the various authors have documented littile or no effect [5,15,19], further limitations of these kind of studies were to rule out effect of concomitant mandibular advancement and genioplasty on Lefort 1 disimpaction stability in long term follow up. Secondly, a higher sample size would yield more significant results.
Conclusion
The major highlights of this study was the results showing the excellent postsurgical changes and stability one year following the superior repositioning of maxilla by Le fort I osteotomy thus encouraging the judicious use of this surgical procedure. There was a significant reduction in the facial height and significant anterior movement of maxilla after surgery was observed. Even one year following surgery, negligible amount of relapse was recorded except at the incisors.
*Student’s paired t test
*Student’s paired t test
*Student’s paired t test