Inguinal hernia is one of the most common surgeries performed in the general surgery practice as nearly 20 million hernia surgeries are performed annually worldwide [1]. Inguinal hernia constitutes about 75% of all abdominal wall hernias with lifetime risk of 27% in males and 3% in adult females respectively [1,2]. The inguinal canal is mainly formed by the external, internal and transverse abdominal muscles. The posterior wall of the inguinal canal is mainly formed by the fusion of aponeurosis of internal oblique and transverse oblique along with fascia transversalis which forms the main support and helps in hernia prevention in normal individuals [3]. Hence, all the hernia surgeries are mandated to strengthen the posterior inguinal canal.
Most inguinal hernias result from a weakness in the abdominal wall that develops by any increase in pressure in the abdomen during coughing, straining, heavy lifting or pregnancy. It is more common after 40 years of age since abdominal muscles weaken with age [4]. However, to the best of our knowledge, there are no previous studies done to objectively assess the abdominal muscle strength in inguinal hernia subjects to confirm it as a causative factor for hernia. The treatment options will change depending on the cause of the hernia with or without mesh repair. Also, subjects with hernia on one side are more prone to develop hernia on the other side. However, there is paucity of literature on the comparison of abdominal muscle strength of unilaterally affected hernia patients with their apparently normal contralateral side. If the other side proven to have decreased muscle strength, prophylactic hernia surgery can be done on the other side. Therefore, the present study was conceived to assess the abdominal muscle strength in healthy subjects and compare it with inguinal hernia patients and to compare the muscle strength of the affected side to the apparently normal side in the inguinal hernia subjects.
Materials and Methods
Sample and Recruitment
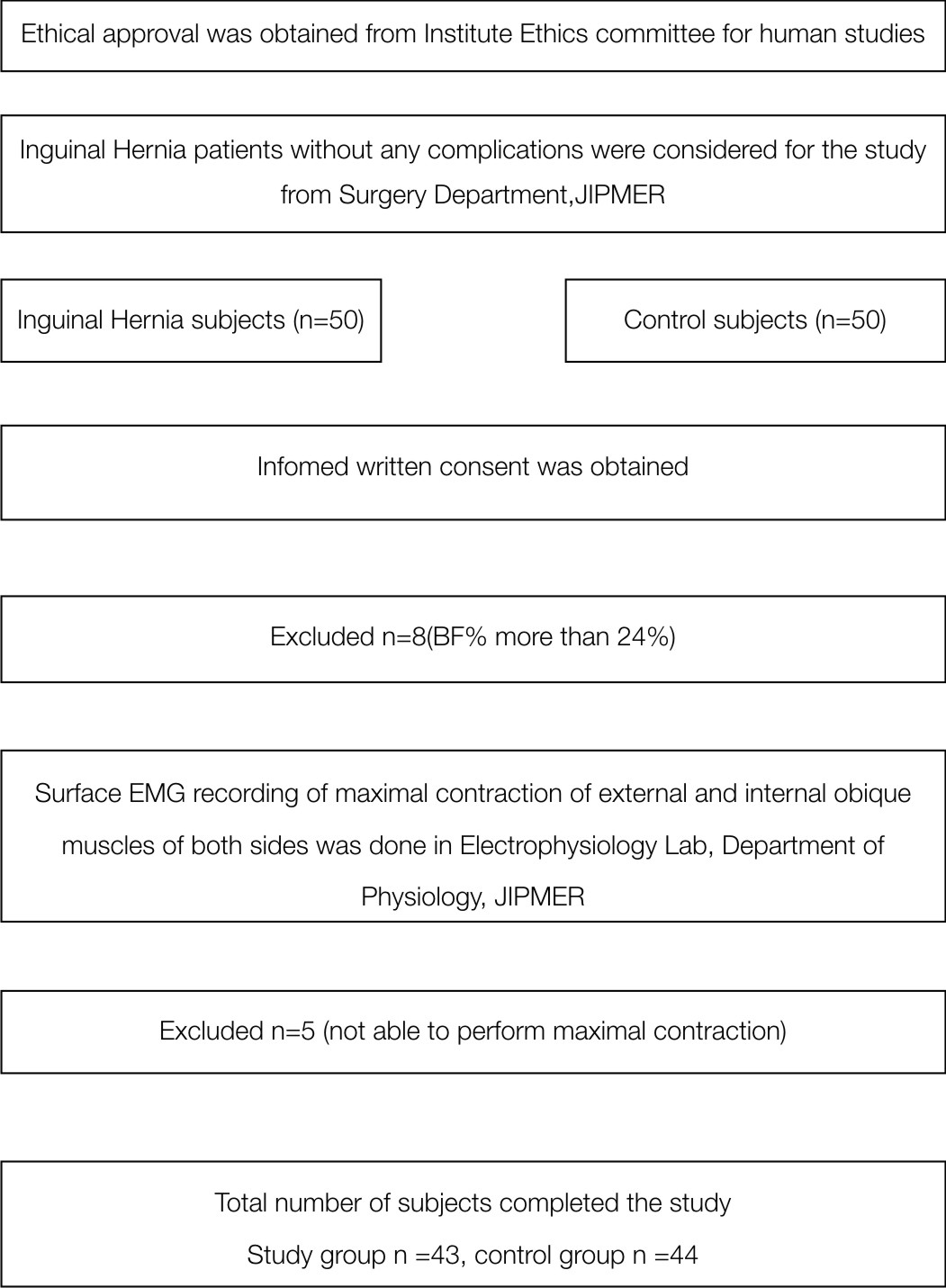
This cross-sectional study was conducted in Electrophysiology Lab, Department of Physiology, JIPMER (Jawaharlal Institute of Postgraduate Medical Education and Research) in collaboration with Surgery department, JIPMER during June 2012 to March 2013. Study was commenced after getting approval from JIPMER, Ethics committee for human studies. Male subjects of 18-70years’ age, diagnosed with inguinal hernia without any known complications were recruited from Surgery department, JIPMER (Study group, n=50). Controls were age matched healthy volunteers who attended the outpatient department along with the patients (n=50). All the participants signed a written informed consent before participating in the study. Only male subjects were taken because it is common in males [1] and to avoid gender difference if any [5]. Subjects with hypothyroidism, collagen diseases of the skin, or any ailment that can interfere with the maximal abdominal muscle contraction were excluded. None of the participants had any previous abdominal muscle strengthening training.
Surface Electromyography (EMG) was done in Electrophysiology Lab, Department of Physiology, JIPMER. Body fat percentage (BF%) was calculated using skin fold thickness measurement [6] and Siri equation (BF% = (495/body density) – 450). Only subjects with BF% less than 24% were considered for the study as the surface EMG can be greatly affected by BF% [7]. (Total= 92, Study=44, control = 48). Flow of the study is given in [Table/Fig-1].
Instrumentation
Neuropack MEB-9200J/K EP/EMG Measuring System (Nihon- Kohden) was used to record the surface EMG. Silver chloride electrodes of 1 cm diameter were used for recording, with an inter-electrode distance of 2 cm. Following setting was used: band with = 10-500Hz, input impedance = 2MΩ (differential), maximum input voltage = ±10 V. sampling rate = 1200 Hz, gain = 1000.
Electromyography Procedure
Surface EMG recordings were done on internal oblique and external oblique muscles of either side. Subjects were instructed about the procedure and at least 5 minutes were given for them to practice. If the subject experiences pain and/or not able to perform the procedure to the maximum contraction, they were excluded from the study (n=5). (Total=87, Study=43, Control = 44) [Table/Fig-1].
The maximum voluntary contractions were performed in lying supine in a bed with the hips and knees flexed to 60o. Head was held in mid-line supported by pillows, with the arms crossed over the chest and hands reaching to the opposite shoulders. The following physiological movements were performed:
1. Targeting right external oblique - trunk flexion consisting of raising the head and thorax until the inferior angles of the scapulae lifted off the bed and adding trunk rotation to the left, once the inferior angle of the left scapula was off the bed.
2. Targeting the right internal oblique - repeating the movement as for trunk flexion but adding right trunk rotation and focusing on pushing the right scapula to the floor once the right inferior angle of the scapula had lifted off the bed [8].
All the contractions were performed for 3 seconds, and repeated three times, with a 30-seconds rest between repetitions. A 1-min rest was given between each muscle contraction. Motor unit potentials were recorded using surface Electromyography (EMG) for individual muscles on both side during maximal contraction. The maximum amplitude of the motor unit potentials out of the three recordings obtained was considered as the strength of the respective muscle.
Electrode Position
The skin was prepared by rubbing with spirit and shaving the area when necessary. Surface electrodes were positioned parallel to the muscle fibres of respective muscles [9]. Conductive gel was applied and the electrodes were taped to the skin and secured using micropore tape. The following anatomic locations were used for electrode placement: Active electrode for External oblique was placed 13 cm lateral to the umbilicus, for internal oblique 3 cm medial and inferior to the right Anterior Superior Iliac Spine (ASIS). A reference electrode was placed over the opposite ASIS [8,10,11].
Statistical Analysis
The magnitude of the force of contraction in EMG recording is given in μV. Data is given in mean and standard deviation, median and range and quartiles for easy of reference with other studies. Comparison between right and left side is done using paired students t-test. Comparison between control and Hernia group is done using unpaired students t-test.
Results
The control and hernia groups were comparable based on age (control group -39.45±16.51; Hernia group-40.12±15.43; p = 0.847) and body fat percentage (control group-15.02±1.90; hernia group – 15.74±1.92; p = .081). [Table/Fig-2] shows the normative data for the maximal force of contraction in four muscles (External Oblique right and left, Internal Oblique right and left) in control subjects. There was no difference in maximal force of contraction between left and right sided muscles.
EMG data for control group (n=44).
| Parameters | EO Right (μV) | EO Left (μV) | IO Right (μV) | IO Left (μV) | Left vs right EO | Left vs right IO |
|---|
| Mean | 1423.32 | 1396.32 | 781.95 | 792.11 | .103 | .125 |
| Std. Deviation | 378.20 | 337.12 | 136.61 | 123.22 | | |
| Median | 1390.00 | 1387.50 | 780.00 | 799.00 | | |
| Range | 1316.70 | 1400.00 | 575.00 | 554.00 | | |
| Minimum | 870.00 | 800.00 | 550.00 | 530.00 | | |
| Maximum | 2186.70 | 2200.00 | 1125.00 | 1084.00 | | |
| Percentiles | 25 | 1029.25 | 1079.25 | 687.50 | 701.250 | | |
| 50 | 1390.00 | 1387.50 | 780.00 | 799.000 | | |
| 75 | 1699.50 | 1599.75 | 855.50 | 853.500 | | |
EO- External oblique muscle; IO- Internal oblique muscle: Std.-Standard; Comparison between sides were done using paired Student t-test.
[Table/Fig-3] shows the maximal force of contraction in four muscles in right side hernia subjects. [Table/Fig-4] shows the maximal force of contraction in left side hernia subjects. The maximal force of contraction was significantly less in the herniated side than the apparently normal side in both right and left side hernia subjects.
EMG data for Right side hernia subjects (n=26).
| Parameters | EO Right (μV) | EO Left (μV) | IO Right (μV) | IO Left (μV) | Left vs right EO | Left vs right IO |
|---|
| Mean | 738.18 | 876.44 | 569.94 | 675.87 | .009 | <.001 |
| Std. Deviation | 330.00 | 407.10 | 265.40 | 297.74 | | |
| Median | 702.00 | 905.00 | 598.50 | 684.35 | | |
| Range | 1149.00 | 1255.00 | 865.50 | 976.00 | | |
| Minimum | 178.00 | 294.00 | 150.00 | 224.00 | | |
| Maximum | 1327.00 | 1549.00 | 1015.50 | 1200.00 | | |
| Percentiles | 25 | 447.00 | 460.75 | 314.75 | 376.750 | | |
| 50 | 702.00 | 905.00 | 598.50 | 684.348 | | |
| 75 | 1005.70 | 1225.25 | 830.00 | 909.500 | | |
EO- External oblique muscle; IO- Internal oblique muscle; Std.-Standard; Comparison between sides were done using paired Student t-test.
EMG data for left side hernia subjects (n=17).
| Parameters | EO Right (μV) | EO Left (μV) | IO Right (μV) | IO Left (μV) | Left vs right EO | Left vs right IO |
|---|
| Mean | 1176.09 | 1079.73 | 863.67 | 697.53 | .008 | .003 |
| Std. Deviation | 384.72 | 335.36 | 248.80 | 235.18 | | |
| Median | 1206.40 | 1149.53 | 975.07 | 790.62 | | |
| Range | 1468.00 | 1440.00 | 885.60 | 857.00 | | |
| Minimum | 357.00 | 160.00 | 367.00 | 186.00 | | |
| Maximum | 1825.00 | 1600.00 | 1252.60 | 1043.00 | | |
| Percentiles | 25 | 1047.40 | 974.00 | 640.83 | 572.000 | | |
| 50 | 1206.40 | 1149.53 | 975.07 | 790.618 | | |
| 75 | 1367.18 | 1231.18 | 1038.39 | 859.514 | | |
EO- External oblique muscle; IO- Internal oblique muscle; Std.- Standard; Comparison between sides were done using paired Student t-test.
[Table/Fig-5] shows that there was significant difference in magnitude of maximal force of contraction between hernia (n=43) and control subjects (n=44) in all the four muscles irrespective of the side of the hernia manifested.
Comparison of control and hernia group (including both right and left hernia subjects).
| Parameters | Control (n=44) | Hernia (n=43) | p-value |
|---|
| Mean | SD | Mean | SD | |
|---|
| EO Right(μV) | 1423.32 | 378.20 | 911.31 | 410.05 | <.001 |
| EO Left(μV) | 1396.32 | 337.12 | 956.81 | 389.37 | <.001 |
| IO Right(μV) | 781.95 | 136.61 | 686.07 | 294.32 | .054 |
| IO Left(μV) | 792.11 | 123.22 | 684.43 | 271.94 | .019 |
| BF% | 15.02 | 1.90 | 15.74 | 1.92 | .081 |
EO- External oblique muscle; IO- Internal oblique muscle; BF%- Body fat percentage; SD- Standard Deviation; Comparison between the groups were done using unpaired Student t-test.
[Table/Fig-6] shows comparison of right side hernia subjects with control subjects. [Table/Fig-7] shows comparison of left side hernia subjects with control subjects. The magnitude of maximal force of contraction was less in all the four muscles as compared to control irrespective of which side the subjects had hernia at the time of recording.
Comparison of control and right hernia subjects.
| Parameters | Control (n=44) | Hernia (n=26) | p-Value |
|---|
| Mean | SD | Mean | SD | |
|---|
| EO Right(μV) | 1423.32 | 378.20 | 738.18 | 330.00 | <.001 |
| EO Left(μV) | 1396.32 | 337.12 | 876.44 | 407.10 | <.001 |
| IO Right(μV) | 781.95 | 136.61 | 569.94 | 265.40 | <.001 |
| IO Left(μV) | 792.11 | 123.22 | 675.87 | 297.74 | .025 |
| BF% | 15.02 | 1.90 | 16.12 | 1.87 | .022 |
EO- External oblique muscle; IO- Internal oblique muscle; BF%- Body fat percentage; SD- Standard Deviation; Comparison between the groups were done using unpaired Student t-test.
Comparison of control and left hernia subjects.
| Parameters | Control (n=44) | Hernia (n=17) | p-Value |
|---|
| Mean | SD | Mean | SD | |
|---|
| EO Right(μV) | 1423.32 | 378.20 | 1176.09 | 384.72 | .026 |
| EO Left(μV) | 1396.32 | 337.12 | 1079.73 | 335.36 | .002 |
| IO Right(μV) | 781.95 | 136.61 | 863.67 | 248.80 | .106 |
| IO Left(μV) | 792.11 | 123.22 | 697.53 | 235.18 | .045 |
| BF% | 15.02 | 1.90 | 15.18 | 1.90 | .778 |
EO- External oblique muscle; IO- Internal oblique muscle; BF%- Body fat percentage; SD- Standard Deviation; Comparison between the groups were done using unpaired Student t-test.
Discussion
Inguinal hernia is one of the most common cases in the Surgical department [12]. Classical text book teaching is to do herniorrhaphy in adults and hernioplasty in old age [12]. There are so many techniques described to do herniorapphy like Bassinies repair, modified Basinie repair, Shouldies technique, Anderson’s technique, Darning technique etc. In hernioplasty, various techniques described are Linchestine technique [13,14], internal ring plugging with mesh placement [15].
All the techniques described above are based on the assumption that abdominal muscle is reduced in the hernia subjects. However, abdominal muscle strength/ power of the muscle of the hernia subjects are not routinely assessed. Review of literature showed that there is no normative data for the magnitude of force of contraction for abdominal muscles. Further, there was no documented recording of reduced abdominal muscle strength in the hernia subjects. If a subject develops hernia on one side, there is 10% chance that he will develop hernia on the other side [16]. Further in patients operated for unilateral inguinal hernia, intraoperatively a contralateral hernia was found in 11-50% of the time [17]. This mandates the assessment of the abdominal muscle strength of either side irrespective on which side, the subject presents with hernia. Hence, the objective of the present study was to assess the maximal force of contraction of the hernia subjects and compare it with age matched control subjects with the secondary objective of comparing the right and left side musclis’ maximal force of contraction.
Only external and internal oblique muscles were chosen for recording EMG in this study for ease of the subject as they have to do maximal contraction of these muscle three times and on either side. Only male subjects were chosen to avoid the difference due to gender if any in the strength of contraction. Since it was surface EMG only motor unit potentials of maximal contraction was recorded as the lesser level of contraction will be difficult to gauge and the recording would have been distorted by the subcutaneous body fat [7]. Further there was no difference in the body fat percentage between controls and hernia subjects [Table/Fig-5].
The major finding in our study is that the maximal force of contraction in external and internal oblique muscle of the side of the hernia in hernia subjects was significantly less as compared to the age and gender matched control subjects. Hence, placing a mesh would be a better technique than other techniques in inguinal hernia repair as it reinforces the abdominal wall bridging the defect [18]. Further, the maximal force of contraction of the non-hernia side of the hernia subjects were also significantly less as compared to control subjects. This justifies the prophylactic repair of the non-hernia side even though the subject presents with unilateral hernia. Before suggesting such recommendations, the logical extension of our study is to have an invasive EMG assessment of all muscles involved in forming the inguinal canal in a larger sample size to have an overall idea about the pathogenesis of the inguinal hernia.
Limitation
Invasive EMG was not done, which could have provided more accurate results as it will not be influenced by body fat percentage and/or subcutaneous fat.
Conclusion
The maximal force of contraction is reduced in external and internal oblique muscles of both side in unilateral inguinal hernia subjects (left/right) as compared to age matched control subjects. Hence, we suggests that reduced abdominal muscle strength has to be considered while performing corrective surgeries in inguinal hernia subjects.
EO- External oblique muscle; IO- Internal oblique muscle: Std.-Standard; Comparison between sides were done using paired Student t-test.
EO- External oblique muscle; IO- Internal oblique muscle; Std.-Standard; Comparison between sides were done using paired Student t-test.
EO- External oblique muscle; IO- Internal oblique muscle; Std.- Standard; Comparison between sides were done using paired Student t-test.
EO- External oblique muscle; IO- Internal oblique muscle; BF%- Body fat percentage; SD- Standard Deviation; Comparison between the groups were done using unpaired Student t-test.
EO- External oblique muscle; IO- Internal oblique muscle; BF%- Body fat percentage; SD- Standard Deviation; Comparison between the groups were done using unpaired Student t-test.
EO- External oblique muscle; IO- Internal oblique muscle; BF%- Body fat percentage; SD- Standard Deviation; Comparison between the groups were done using unpaired Student t-test.