Supra Hepatic Inferior Vena Cava Thrombosis–Surgical Challenges
Senthil Muthuraman1, Anand Ramamurthy2, Mahesh Gopashetty3, Cuddalore Sadasivam Vijayshankar4, Anand Khakhar5
1 Fellow, Department of Liver Transplant, Apollo Hospital, Chennai, India.
2 Senior Consultant, Department of Liver Transplant, Apollo Hospital, Chennai, India.
3 Senior Consultant, Department of Liver Transplant, Apollo Hospital, Bengaluru, India.
4 Senior Consultant, Department of Cardiothoracis Surgery, Apollo Hospital, Chennai, India.
5 Senior Consultant, Department of Liver Transplant, Apollo Hospital, Chennai, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Senthil Muthuraman, 5634 South Fourth Street, Pudukkottai – 622001, Tamil Nadu, India.
E-mail: drsenthilm@gmail.com
Autosomal Dominant Polycystic Kidney Disease (ADPKD) is a chronic affliction characterized by numerous liver and kidney cysts. There is a gradual but progressive renal and liver impairment which may require combined liver-kidney transplantation. Compression of the retrohepatic Inferior Vena Cava (IVC) by an enlarged polycystic liver may impede clear visualization on pre-operative imaging and miss an underlying thrombosis or obliteration. This may result in an intra-operative surprise. Management can be challenging requiring modification of conventional surgical approach. We present our experience of a 67-year-old patient who underwent combined liver-kidney deceased donor transplantation for decompensated chronic liver disease with chronic kidney disease due to ADPKD. She was diagnosed with ADPKD for 16 year, with progressive deterioration in kidney function over the last 6 year and liver decompensation following knee replacement surgery requiring regular renal replacement therapy. We report this case to highlight the peri-operative challenges and their management along with a review of published literature on this uncommon occurrence.
Chronic kidney disease, Combined liver and kidney transplant, Decompensated chronic liver disease
Case Report
A 67-year-old lady presented with complains of pedal oedema, abdominal distension and jaundice. She was diagnosed to have ADPKD with innumerable cysts in both kidneys and liver for 16 years. She was asymptomatic for 10 years. Subsequently she developed a steady increase in her creatinine but not requiring dialysis. She underwent bilateral total knee replacement, following which she developed urinary tract infection. Since then, she started showing signs of decompensation like jaundice and ascites and diagnosed to have decompensated chronic liver disease with portal hypertension with chronic kidney disease. She developed recurrent urosepsis with multi organ dysfunction five months after the surgery and recovered after a month of hospital stay but since then, requiring thrice weekly renal replacement therapy.
Ultrasonography of the abdomen revealed multiple cysts in liver and kidneys with moderate ascites. Contrast Enhanced Computerized Tomography (CECT) confirmed multiple cysts in kidneys and liver with largest cyst 10cm in size. The supra hepatic Inferior Vena-Cava (IVC) was reported to be compressed with patent hepatic veins [Table/Fig-1,2]. Her cardiac and pulmonary evaluation was normal. She was taken for combined liver and kidney transplant after multi-disciplinary evaluation as per institutional protocol.
Thrombosed Supra-hepatic IVC with narrowed opening into right atrium.
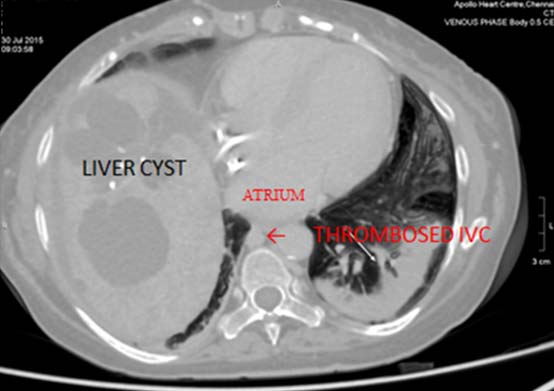
CT image showing polycystic liver and kidney disease.

Intra-operatively dense adhesions of the liver to stomach, greater omentum and colon were found. Some of these larger cyst contain turbid purulent fluid. The adhesiolysis and recipient hepatectomy was performed. At the time of cross clamping, the supra-hepatic IVC was cord like to palpation. The infra-hepatic IVC was normal. The diaphragm and pericardium was opened to expose the IVC opening into the right atrium. The lumen of the IVC was found to be obliterated till its junction with the right atrium. A side biting vascular clamp was applied on the right atrium and the donor supra hepatic portion of IVC was anastomosed with right atrium with 4’0 prolene and the pericardium was closed with a bovine pericardial patch. Donor infra hepatic IVC was anastomosed with recipient IVC with 4’0 prolene. The Portal Vein (PV), Hepatic Artery (HA) and bile duct were anastomosed in standard fashion. Donor kidney was implanted through separate incision in right iliac fossa in a standard fashion [Table/Fig-3,4].
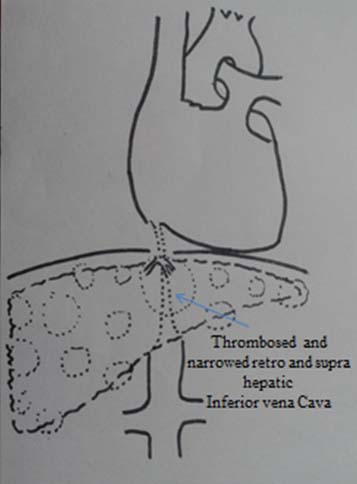
Diagrammatic representation of thrombosed supra and retro hepatic portion IVC with normal infra hepatic IVC.
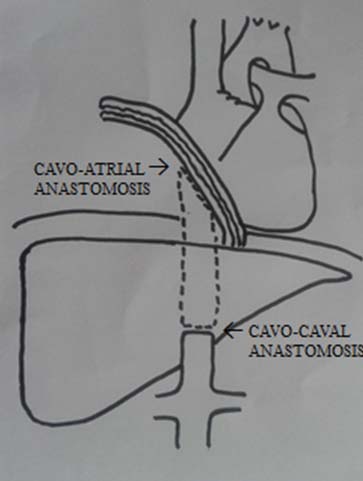
Diagrammatic representation of cava replacement and right atrial anastomosis.
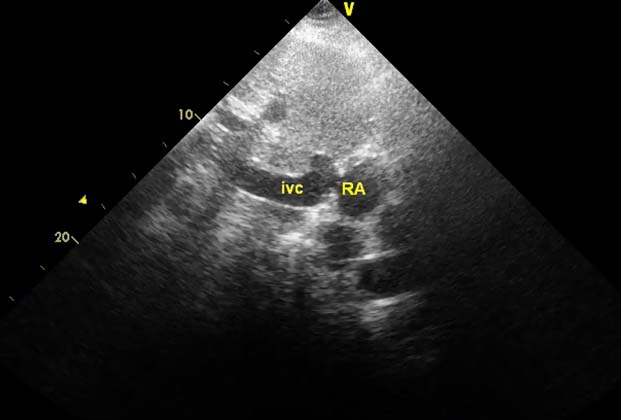
Patient was ventilated electively and extubated on Post-operative Day (POD) one. Post-operative ECHO showed patent cavo-atrial anastomosis [Table/Fig-5]. Post-operatively inotropic supports were discontinued on POD two. She was initially coagulopathic with hemorrhagic drain output which was managed with transfusion of blood products guided by thromboelastography. She developed supra ventricular tachycardia on POD two and atrial fibrillation on POD four which was managed medically. She also had persistent carbon dioxide retention which was managed with non-invasive ventilation and aggressive physiotherapy. As per the Institution protocol patient received immunosuppressants (Triple immunosuppression with Steroid, Tacrolimus and Mycophenolate Mofetil). She improved symptomatically and was discharged on POD 11. She remains well six month following surgery.
Inferior vena caval and right atrial anastomosis – postoperative ECHO.
Discussion
The first case of combined liver and kidney transplantation was reported by Watts RW at Innsbruck University Hospital, in 1984. The patient survived more than nine years [1]. According to Margreiter, the indications for combined liver-kidney transplantation are divided into the following categories [2,3]:
Disease affecting both organs, such as autosomal dominant polycystic disease.
Renal disorders with liver involvement or liver disorders with renal involvement, including primary type I hyperoxaluria, type I glycogen storage disease, cholesterol acyltransferase deficiency, etc.
Evidence of chronic kidney disease in End Stage Liver Disease (ESLD) patients and renal biopsy demonstrating more than 30% of glomeruloesclerosis or 30% of interstitial fibrosis.
Patients with ESLD and Chronic Kidney Disease (CKD) with GFR < 30 mL/min
Patients with acute kidney injury with creatinine >2.0 mg/dL and dialysis requirement > 8 weeks.
ADPKD is characterized by the formation of renal cysts and a variety of extra renal manifestations of which Polycystic Liver Disease (PLD) is the most common. It affects up to 0.2% of the general population, whereas the isolated PLD has a prevalence of less than 0.01% [4]. In rare situation of occlusion of IVC and HV, IVC replacement and liver transplant have been shown to successfully treat the condition [5].
Combined liver-kidney transplantation may be the only surgical option for patients with ADPKD with decompensated liver and chronic kidney disease. Usually in ADPKD there might be a compression of the intra hepatic IVC by larger cyst and enlarged liver [6]. This extrinsic mechanical stress on the IVC has been found to induce thrombosis in the IVC [7]. Cystic liver disease is not commonly recognized as a cause of hepatic vein/ IVC obstruction; although it was listed by Wang et al., as a cause of Budd-Chiari Syndrome (BCS) in one of their 100 patients [8]. For patients with inferior vena cava occlusion, resection of the vein with reconstruction is required to supply a patent venous drainage.
Reconstruction of the resected cava is easy in deceased donor liver transplant due to the presence of long length of suprahepatic vena cava in the liver allograft. In our patient, the IVC lumen was obliterated till the IVC-right atrium junction and a side to end atrio-caval anastomosis was performed (donor supra hepatic IVC to recipient atrium). In case of absence of adequate length of supra caval IVC or in living donor liver transplantation [9] prosthetic graft can be used for reconstruction.
Conclusion
A high index of suspicion is required in patients undergoing liver transplant for ADPKD. When preoperative CT is unable to visualize the IVC satisfactorily or where there is evidence of narrowed / compressed IVC. An extended resection of cava up to the right atrium and advanced vascular reconstruction techniques with grafts or prosthesis may be required.
[1]. Watts RW, Calne RY, Williams R, Manseli M, Veall N, Purkiss P, Primary hyperoxaluria (type I): attempted treatment by combined hepatic and renal transplantationQ J Med 1985 57(222):697-703. [Google Scholar]
[2]. He XS, Huang JF, Chen GH, Zheng KL, Ye XM, A successful case of combined liver and kidney transplantation for autosomal dominant polycystic liver and kidney diseaseWorld J Gastroenterol 1999 5(1):79-80. [Google Scholar]
[3]. Eason JD, Gonwa TA, Davis CL, Sung RS, Gerber D, Bloom RD, Proceedings of consensus conference on simultaneous liver kidney transplantation (SLK)Am J Transplant 2008 8(11):2243-51. [Google Scholar]
[4]. Temmerman F, Missiaen L, Bammens B, Laleman W, Cassiman D, Verslype C, Systematic review: the pathophysiology and management of polycystic liver diseaseAliment Pharmacol Ther 2011 34(7):702-13. [Google Scholar]
[5]. Yaylak F, Ince V, Barut B, Unal B, Kilic M, Yilmaz S, Living related donor liver transplantation with atrio-caval anastomosis of inferior vena cava graft stored in deep-freeze for budd-chiari SyndromeInt J Organ Transplant Med 2015 6(1):41-43. [Google Scholar]
[6]. Torres VE, Rastogi S, King BF, Stanson AW, Gross JB, Nogorney DM, Hepatic venous outflow obstruction in autosomal dominant polycystic kidney diseaseJ Am SocNephrol 1994 5(5):1186-92. [Google Scholar]
[7]. Iguchi S, Kasai A, Kishimoto H, Suzuki K, Ito S, Ogawa Y, Thrombosis in Inferior Vena Cava (IVC) due to intra-cystic hemorrhage into a hepatic local cyst with Autosomal Dominant Polycystic Kidney Disease (ADPKD)Intern Med 2004 43(3):209-12. [Google Scholar]
[8]. Wang Z, Zhu Y, Wang S, Pu LP, Du Y, Zhang H, Recognition and management of Budd-Chiari Syndrome (RBS): Report of one hundred casesJ Vasc Surg 1989 10(2):149-56. [Google Scholar]
[9]. Sakçak I, Eri C, Ölmez A, Kayaalp C, Yılmaz S, Replacement of the vena cava with aortic graft for living donor liver transplantation in Budd-Chiari syndrome associated with hydatid cyst surgery: a case reportTransplant Proc 2012 44(6):1757-58. [Google Scholar]