Female Genital Tract Involvement in Acute Lymphoblastic Leukemia: A Rare Case Report
Vikram Narang1, Amit Dhiman2, Bhavna Garg3, Neena Sood4
1 Assistant Professor, Department of Pathology, Dayanand Medical College and Hospital, Ludhiana, Punjab, India.
2 Assistant Professor, Department of Medical Oncology, Dayanand Medical College and Hospital, Ludhiana, Punjab, India.
3 Professor, Department of Pathology, Dayanand Medical College and Hospital, Ludhiana, Punjab, India.
4 Professor and Head, Department of Pathology, Dayanand Medical College and Hospital, Ludhiana, Punjab, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Vikram Narang, Assistant Professor, Department of Pathology, Dayanand Medical College and Hospital, Ludhiana-141001, Punjab, India.
E-mail: drvikramnarang@yahoo.com
Female Genital Tract (FGT) involvement with hematologic neoplasms is uncommon and the hematologic malignancies which involve the female genital organs are usually non-Hodgkin’s lymphoma. Involvement of the uterus and cervix with Acute Lymphoblastic Leukaemia (ALL) is extremely rare, and ovarian involvement is even rarer. We report the case of a young lady who presented with tubo-ovarian mass, excessive post-operative bleeding (post-total abdominal hystrerctomy and bilateral salpingo-oophorectomy) and was diagnosed to have ALL with blood and tissue involvement by histopathology and flow cytometry.
Diagnosis, Flow cytometry, Haematolymphoid malignancy, Ovary
Case Report
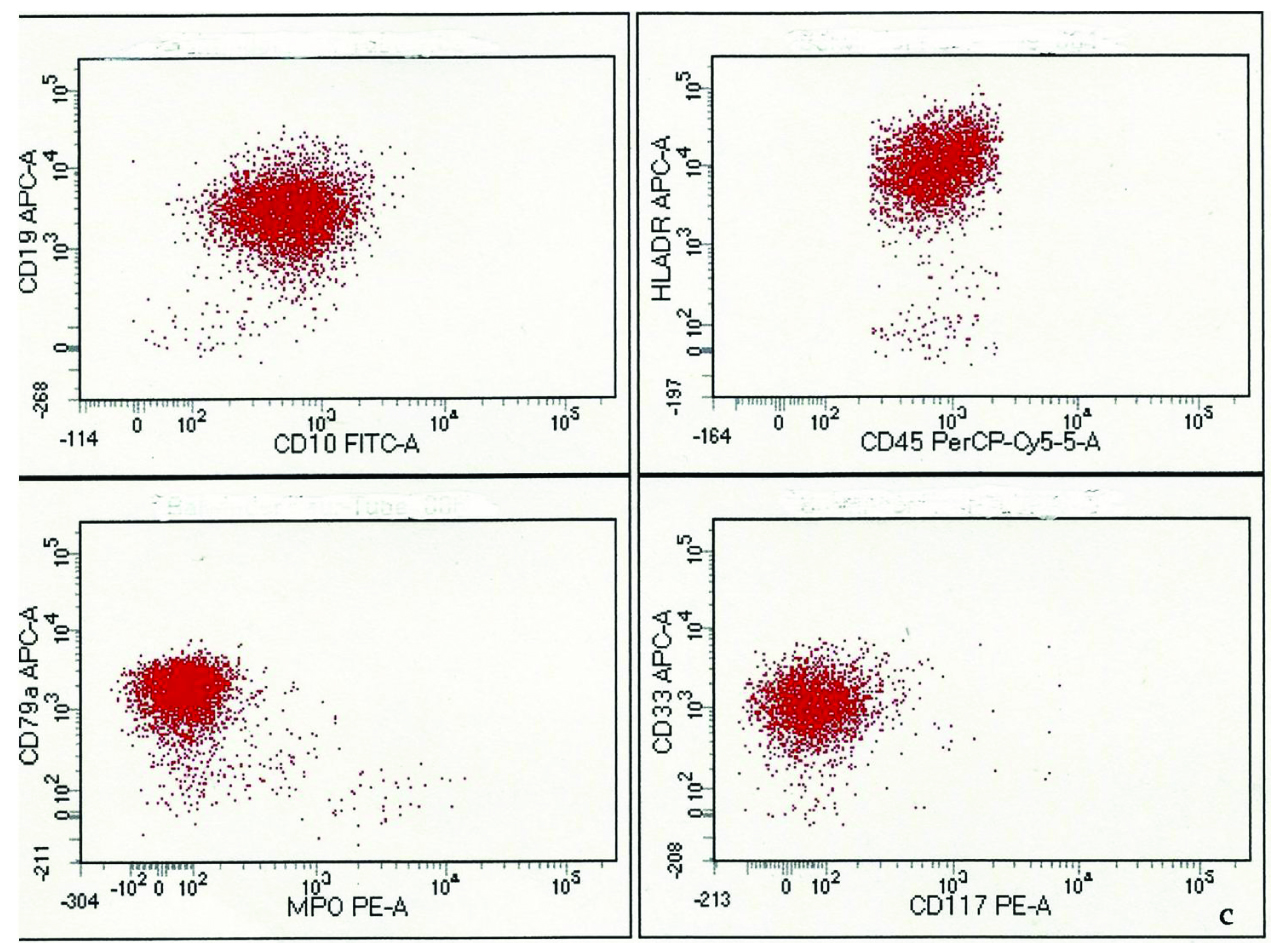
A 20-year-old female was referred from a peripheral hospital with clinical history of tubo-ovarian mass, bleeding per vagina and thrombocytopenia (platelets-32000/cumm). She underwent total abdominal hysterectomy and bilateral salpingo-oophorectomy with clinical suspicion of ruptured ectopic and impending sepsis. Post-operatively, her leucocyte count showed sudden increase (TLC- 95000/cumm) and platelets decreased to 29000/cumm. Thus, she was sent to us for a detailed examination and further management. Peripheral blood smear examination was done which revealed 90 percent blasts. Immuno-phenotyping was done on peripheral blood using BD FACS Canto II flow cytometer and cells were processed with stain-lyse-wash technique. SSC low and CD45 dim intensity gated events constituted 50% and these events were positive for HLA-DR, CD10, CD19, CD79a, CD33 [Table/Fig-1].
Scattergrams showing SSC-A low and CD45 dim events to be positive for HLA-DR, CD10, CD19, CD79a and CD33 (aberrant)
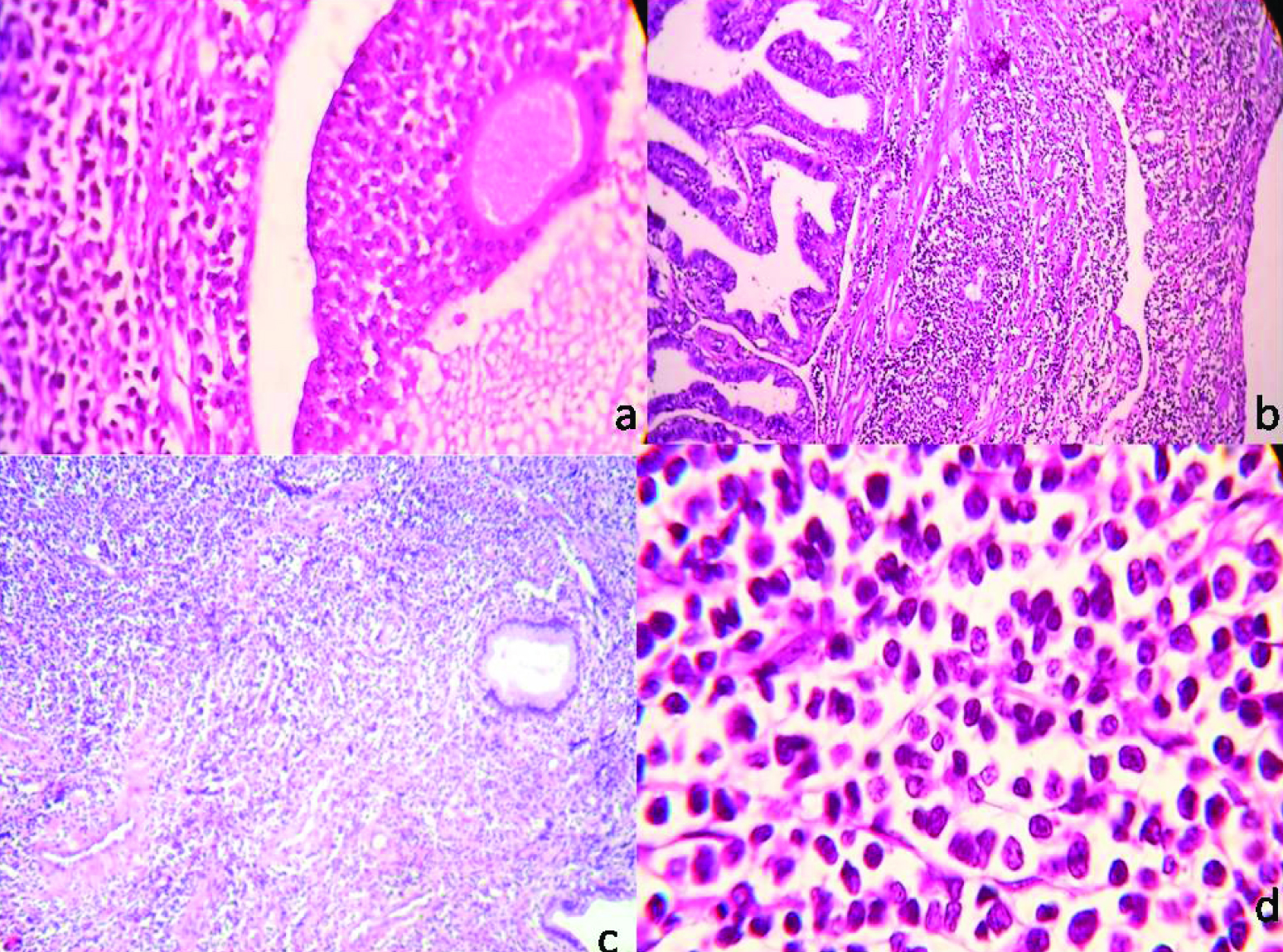
Simultaneously, gross specimen of hysterectomy with bilateral salpingoophercetomy showed bilateral bulky ovaries which on cut section were solid and haemorrhagic. Uterus, cervix and bilateral fallopian tubes showed no gross pathology. Microscopic examination revealed diffuse infiltration of uterus, cervix, bilateral tubes and ovaries by leukaemic cells having hyperchromatic nuclei, irregular nuclear margins and scant amount of cytoplasm [Table/Fig-2a-d]. The diagnosis of Precursor B lymphoblastic leukaemia infiltrating the female genital tract was rendered.
(a) Microphotograph showing ovarian follicle surrounded by leukaemic cells. (H&E, 40X); (b) Sections from the fallopian tube show infiltration by blast cells. (H&E, 4X); (c) Microphotograph exhibiting endocervical glands and diffuse infiltration by leukaemia. (H&E, 4X); (d) High power view of leukaemic cells exhibiting large size, high nucleo cytoplasmic ratio and scant cytoplasm. (H&E, 40X)
The patient died on the third hospital day due to extensive haemorrhage and sepsis.
Discussion
Female Genital Tract (FGT) involvement by hematologic neoplasms is uncommon. The non-Hodgkin lymphomas like diffuse large-cell, Burkitt and follicular lymphomas are common as compared to precursor B-cell lymphoblastic lymphomas/leukaemia. The primary sites of extramedullary disease in Acute Lymphocytic Leukaemia (ALL) are central nervous system and testes. Though uterine and cervix involvement is frequently described but primary ovarian involvement is rarely observed [1–3].
Leukaemic involvement of ovary has been found in up to 30% of patients with ALL at autopsy or relapsed cases. The present case did not have any past history of treatment of leukaemia therefore, primary tissue involvement was the only possible diagnosis. Moreover, the peripheral blood immunophenotyping confirmed the diagnosis of acute lymphoblastic leukaemia.
Radiological investigations can be used in evaluating the ovary either prior to cessation of chemotherapy or on subsequent follow-up. However, histopathological examination is key to diagnose and distinguish such lesions from other round-cell tumours like dysgerminoma, primary small-cell carcinoma and adult granulosa cell tumour [4–6].
Dysgerminoma usually has sheets and nests of tumour cells with nuclei having fine nuclear chromatin and abundant clear cytoplasm. Periodic Acid-Schiff (PAS) positivity of the cytoplasm is also a differentiating feature with immunohistochemical studies like Placental alkaline phosphatase (PLAP) positivity, Oct 4 positivity and Leucocyte common antigen (LCA) negativity assist in establishing the diagnosis. The primary small cell carcinoma exhibits cohesive cell growth with nuclear moulding along with Cytokeratin positivity. The adult granulose cell tumour has characteristic trabecular, insular, micro or macro follicular pattern and tumour cells have grooved nuclei. The Call Exner bodies and Inhibin and Calretinin positivity make the diagnosis almost certain.
As in the present case there was extensive involvement of the FGT, the differential diagnosis include lymphoma like lesions, endometrial stromal sarcoma, embryonal rhabdomyosarcoma. The lymphoma like lesions usually shows superficial mixed infiltrate as compared to monomorphic cells infiltrating deep tissues and presenting as mass lesions in lymphomas. The endometrial stromal sarcoma usually has tongue like growth pattern and evenly distributed cells moreover, theses cells are CD45 negative as compared to lymphomas. The embryonal rhabdomyosarcomas are common in pediatric patients and positivity of immunohistochemical markers like desmin and myogenin assist in diagnosis.
In the present case immunophenotyping confirmed the diagnosis of precursor B- Lymphoblastic leukaemia with aberrant CD-33 expression. The presence of aberrant myeloid antigen in ALL portends a poor prognosis compared to ALL cases without myeloid antigens, and a poor response to drug therapies targeting conventional ALL. The present case also had a fatal outcome before the treatment could be initiated due to extensive tissue involvement. More studies with follow up are required to ascertain the correlation of these markers with prognosis and therapeutic response, as well as whether, drug therapies targeting myeloid antigens could be of use in treatment [7,8].
The patients with acute leukaemia have thrombocytopenia in majority of patients thus females may present with abnormal uterine bleeding as a feature of leukaemia. Apart from thrombocytopenia, increased menstrual losses could be due to diffuse infiltration of leukaemia in the female genital tract leading to tissue destruction thus, predisposing to abnormal uterine bleeding [9,10]. Thus, emphasing the thorough radiological and histopathological evaluation of leukaemic patients both at presentation and at follow up to prevent the adverse outcomes.
Conclusion
Menorrhagia is common in females with acute leukaemia and is usually overlooked. The female genital tract involvement is rare and ovary involvement is even rarer. Though radiological features do help in recognising these lesions but definitive diagnosis can be made only by histological analysis, and immunophenotyping. The case is presented due to its rarity.
[1]. Geetha N, Lali VS, Mathews A, Prakash NP, Acute lymphoblastic leukaemia presenting with a uterine cervical massClin Cancer Investig J 2015 4:280-81. [Google Scholar]
[2]. Oliva E, Ferry JA, Young RH, Prat J, Srigley JR, Scully RE, Granulocytic sarcoma of the female genital tract: A clinicopathologic study of 11 casesAm J Surg Pathol 1997 21:1156-65. [Google Scholar]
[3]. Rajnics P, Demeter J, Csomor J, Krenács L, Pajor L, Kollár B, Rare primary extranodal lymphomas: Diffuse large B-cell lymphomas of the genital tractAnn Hematol 2009 88:1223-28. [Google Scholar]
[4]. Tan S, Peng X, Cao Y, Primary precursor B cell lymphoblastic lymphoma of uterine corpus: case report and review of the literatureArchives of Gynecology and Obstetrics 2011 1:1289-92. [Google Scholar]
[5]. Lane DM, Birdwell RL, Ovarian leukaemia detected by pelvic sonography. A case reportCancer 1986 58:2338-42. [Google Scholar]
[6]. Crasta JA, Vallikad E, Ovarian lymphomaIndian J Med Paediatr Oncol 2009 30(1):28-30. [Google Scholar]
[7]. Slasky BS, Straub WH, Deutsch M, Acute lymphocytic leukaemia of the ovary: the value of sonographyJ Comput Tomogr 1982 6(2):161-65. [Google Scholar]
[8]. Suggs JL, Cruse JM, Lewis RE, Aberrant myeloid marker expression in precursor B-cell and T-cell leukaemiasExp Mol Pathol 2007 83(3):471-73. [Google Scholar]
[9]. Tsuruchi N, Okamura J, Childhood acute lymphoblastic leukaemia relapse in the uterine cervixJ Pediatr Hematol Oncol 1996 18:311-13. [Google Scholar]
[10]. Kazi S, Szporn AH, Strauchen JA, Chen H, Kalir T, Recurrent precursor-B acute lymphoblastic leukaemia presenting as a cervical malignancyInt J Gynecol Pathol 2013 32:234-37. [Google Scholar]