Solid-Cystic Hypoglossal Nerve Schwannoma with Fluid-Fluid Level: A Rare Case Report
Kulamani Sahoo1, Pramod Ramchand Shaha2, Rahul Khetawat3, Mohd. Abbas Ilyas4, Gaurav Rajendra Khairnar5
1 Head of Department, Department of Radiology, Krishna Hospital and Medical Research Center, Karad, Maharashtra, India.
2 Professor, Department of Radiology, Krishna Hospital and Medical Research Center, Karad, Maharashtra, India.
3 Resident, Department of Radiology, Krishna Hospital and Medical Research Center, Karad, Maharashtra, India.
4 Resident, Department of Radiology, Krishna Hospital and Medical Research Center, Karad, Maharashtra, India.
5 Resident, Department of Radiology, Krishna Hospital and Medical Research Center, Karad, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rahul Khetawat, Resident, Department of Radiology, Krishna Hospital and Medical Research Center, Karad-415110, Maharashtra, India.
E-mail: rahul.med11@gmail.com
Schwannomas (neurinoma, neurilemmoma) are benign slow-growing encapsulated tumours originating from well-differentiated myelin-producing Schwann cells or nerve fiber sheet cells at the glial-Schwann cell junction. Hypoglossal nerve schwannoma mostly develops in the intracranial and extra-cranial segment or in both intracranial and extra-cranial segment forming a dumbbell shape tumour. The peripheral hypoglossal schwannomas are very rare. We present a case of right hypoglossal nerve schwannoma in a 46-year-old female who presented with headache and neck pain since 2 weeks with deviation of tongue to right side since 1 week. Patient was investigated with Computed Tomography (CT) scan of head and Magnetic Resonance Imaging (MRI) of brain, which showed a dumb-bell shaped solid-cystic mass lesion with fluid-fluid level in right cerebello-pontine angle cistern.
Cranial nerves, Cystic, Nerve sheath, Tumour
Case Report
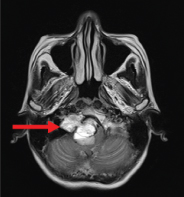
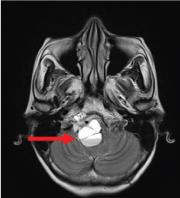
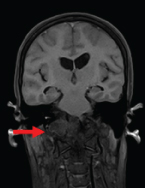
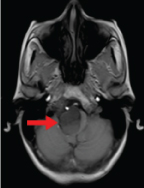
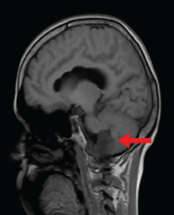
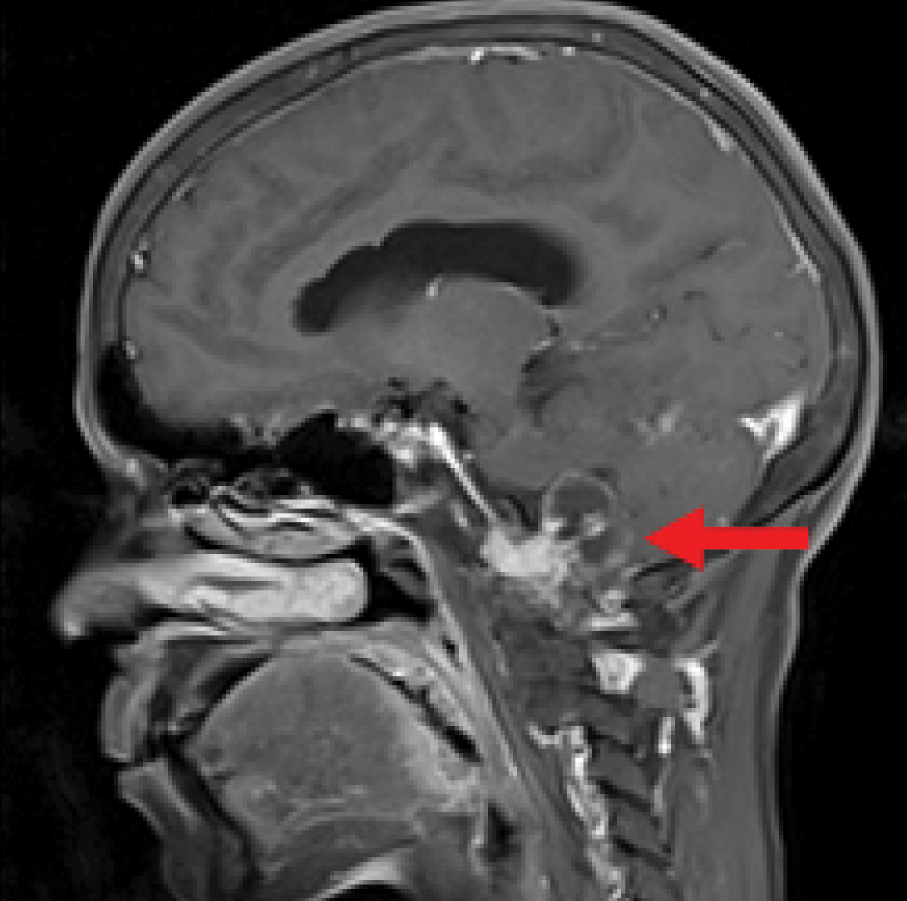
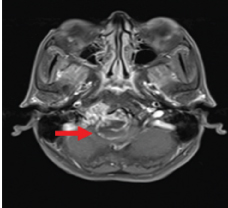
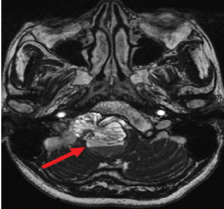
A 46-year-old female complaining of headache and neck pain since 2 weeks with deviation of tongue to right since 1 week with no significant past and family history. On clinical examination, patient has reduced gag reflex. Patient was investigated with Computed Tomography (CT) scan of head and Magnetic Resonance Imaging (MRI) of brain. MRI findings include well-defined, heterogeneously enhancing lobulated, dumb-bell shaped solid-cystic lesion measuring ~ 3.28x2.79x2.29cm with fluid-fluid level (supernatant part was more hyperintense on T2WI than dependent part) [Table/Fig-1,2], noted in right cerebello-pontine angle cistern (lateral medullary cistern) seen extending into right hypoglossal canal. The lesion was markedly compressing medulla and fourth (4th) ventricle. Lesion was heterogeneously hyperintense on T2WI/FLAIR [Table/Fig-1,2], hypo- to iso- intense on T1WI [Table/Fig-3,4 and 5], with multiple areas of blooming on Haemo/SWI [Table/Fig-6,7] indicating haemorrhage within and in the periphery of lesion. The lesion showed heterogeneous enhancement of solid component with peripheral (rim) enhancement of cystic component [Table/Fig-8,9 and 10]. Lesion was obliterating ponto-cerebellar sulcus on right side. Right-sided cisternal segments of Glassopharyngeal (IXth) nerve, Vagus (Xth) nerve and hypoglossal (XIIth) nerve are not seen separately from the lesion in the cerebello-pontine angle cistern (lateral medullary cistern) [Table/Fig-11].
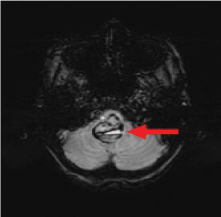
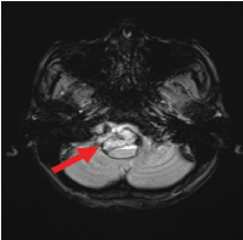
T2WI Axial; shows a dumb-bell shaped solid-cystic lesion in right cerebello-pontine angle cistern (lateral medullary cistern) seen extending into right hypoglossal canal.
T2WI Axial; shows a dumb-bell shaped solid-cystic lesion with fluid-fluid level (supernatant part is more hyperintense on T2WI than dependent part), noted in right cerebello-pontine angle cistern (lateral medullary cistern).
T1WI Coronal; hypo- to iso- intense lesion in right cerebello-pontine angle cistern (lateral medullary cistern) seen extending into right hypoglossal canal.
T1WI Axial; hypo- to iso- intense lesion in right cerebello-pontine angle cistern (lateral medullary cistern) seen extending into right hypoglossal canal.
T1WI Sagittal; hypo- to iso- intense lesion in right cerebello-pontine angle cistern (lateral medullary cistern).
Haemo Axial; shows multiple areas of blooming predominantly in the periphery of the lesion.
SWI Axial; shows multiple areas of blooming predominantly in the periphery of the lesion.
T1FS C+ Coronal:- shows well defined heterogeneously enhancing lesion in right cerebello-pontine angle cistern.
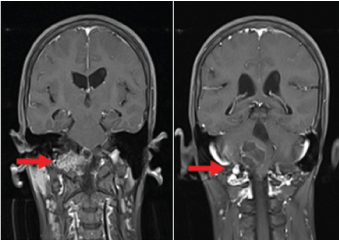
T1FS Sagittal–Post-contrast- shows well defined heterogeneously enhancing lesion compressing medulla.
T1FS Axial –Post-contrast- shows well defined heterogeneously enhancing lesion in right cerebello-pontine angle cistern.
Axial CISS sequence- shows right sided Cranial nerves IX, X, XII not delineated separately from lesion (arrow).
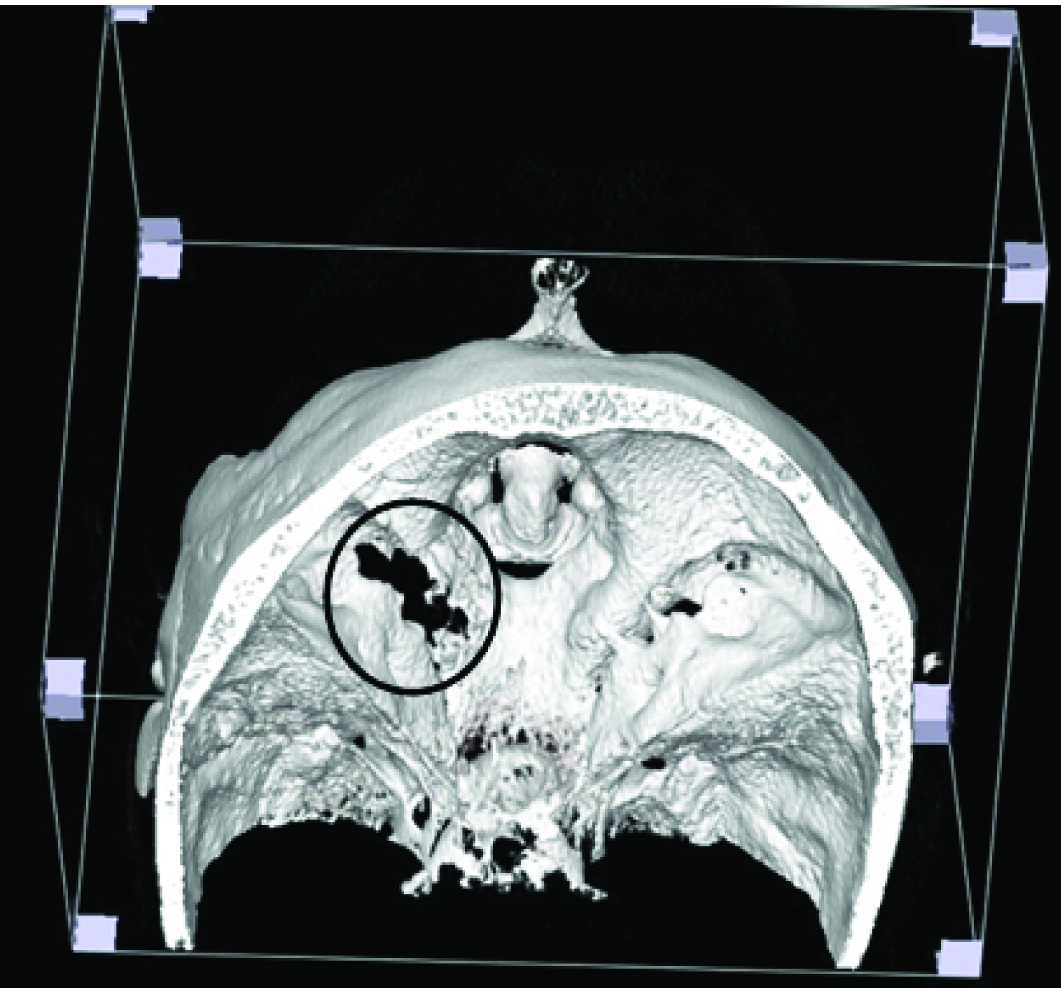
CT scan demonstrated the lesion entering the right hypoglossal canal and has eroded the occipital bone and jugular bulb [Table/Fig-12,13].
CT scan bone window – demonstrated the lesion entering the right hypoglossal canal and has eroded the occipital bone and jugular bulb.
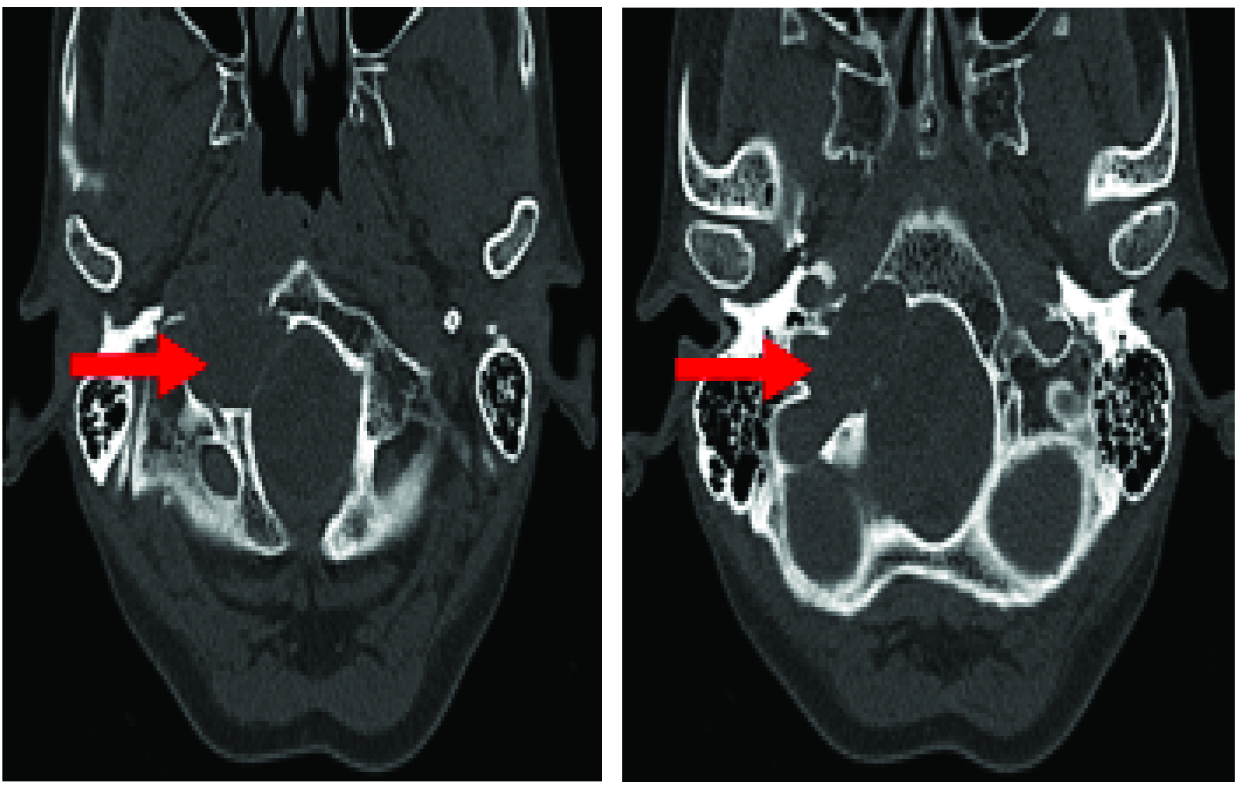
CT VRT image - demonstrated the lesion entering the right hypoglossal canal and has eroded the occipital bone and jugular bulb.
The bulk of the lesion was removed by suboccipital craniotomy through subtonsillar approach. Sample sent for histopathology. Histopathology showed typical features of schwannomas - spindle cells arranged in bundles and fascicles. Cellular areas showing spindle cells arranged in palasading fashion and having organoid arrangement forming Verocay bodies (Antoni type A areas). The cells in Antoni type B areas have round condensed nuclei and indistinct cytoplasm. In other areas, tumour cells were separated by abundant edematous stroma and at places cystic areas. The intervening stroma was fibrocollagenous and shows foci of haemorrhages.
Discussion
Schawannomas (less commonly known as neurinoma, neurilemmoma) are benign slow-growing encapsulated tumours originating from well-differentiated myelin-producing schwann cells or nerve fiber sheet cells at the glial-Schwann cell junction [1]. According to Kaye et al., classification of the jugular foramen schwannomas (neurinoma, neurilemmoma), the hypoglossal schwannomas documented in the literature are divided into three types: Type A, intracranial in 31.5%; type B, dumbbell shaped or extra- and intracranial in 50%; type C, extracranial in 18.5% [2].
Over 90% of cases are presented as acoustic schawannomas. Schwannomas arise very rarely from primarily motor nerves. The purely motor hypoglossal nerve emerges from the medulla oblongata between the pyramid and the olivary bodies, passes extra-cranially through the hypoglossal canal [3].
Fluid levels in solid-cystic schwannomas may be due to collection of liquefactive necrotic materials or by haemorrhage from hypervascular schwannomas [4]. Usually, this blood does not clot, so that some part of the fluid is unclotted blood, which may create a level against serous (interstitial) fluid [4]. Takahashi et al., reported that a hypervascular hypoglossal schwannoma with hyaline degeneration of vessels had extensive intra-tumoural haemorrhage [5].
Hypoglossal schwannomas usually cause ipsilateral hypoglossal nerve palsy. Hypoglossal nerve palsy has particular diagnostic value, as 85.7% of patients with hypoglossal schwannomas present with this symptom [4].
Lesion in our patient showed T1 low signal, T2 high signal, and heterogenous post-contrast enhancement. Such contrast enhancement pattern is also seen in meningiomas, though meningiomas usually have lower T2 signal intensity and higher pre-contrast attenuation in CT as compared to schwannomas. In addition, they may show calcification with hyperostosis; furthermore, growth within the jugular foramen and/or below the skull base is unusual for meningiomas. Another important differential diagnosis is glomus jugulare tumour. This is a highly vascular tumour, which shows intense post-contrast enhancement and, most importantly, multiple small flow voids (“salt and pepper” appearance on MR images) is pathognomic for glomus jugulare. Schwannomas do not show internal flow voids, in some relatively vascular vestibular schwannomas flow voids at the periphery can be seen [6].
Conclusion
Dumbbell-shaped solid-cystic hypoglossal nerve schwannomas are extremely rare skull base tumours. Patients usually present with symptoms due to increased intracranial tension and hypoglossal nerve palsy, though symptoms due to 10th or 11th nerve are less commonly encountered. Both imaging (MRI and CT scan) and clinical presentation plays very important role in interpretation of lesion and narrowing differential diagnosis.
[1]. Osborn AG, Brain – Imaging, pathology, and anatomy; Amirsys Jan 2013 1st edition – 2nd:626-38. [Google Scholar]
[2]. Kaye AH, Hahn JF, Kinney SE, Hardy RW Jr, Bay JW, Jugular foramen schwannomasJ Neurosurg 1984 60:1045-53. [Google Scholar]
[3]. Masoud N, Mohammad F, Kamandi S, Hypoglossal schowannoma: A case report and review of literatureIranian Journal of Otorhinolaryngology 2011 23(1):45-50. [Google Scholar]
[4]. Li WC, Hong XY, Wang LP, Ge PF, Fu SL, Luo YN, Large cystic hypoglossal schwannoma with fluid-fluid level: A case reportSkull Base 2010 20:193-97. [Google Scholar]
[5]. Takahashi T, Tominaga T, Sato Y, Watanabe M, Yoshimoto T, Hypoglossal neurinoma presenting with intratumoural haemorrhageJ Clin Neurosci 2002 9:716-19. [Google Scholar]
[6]. Petter EO, Gabrielsen TO, Jacobsen EA, Imaging findings in schwannomas of the jugular foramenAJNR Am J Neuroradiol 2000 21:1139-44. [Google Scholar]