A Study of Medication Compliance in Geriatric Patients with Chronic Illnesses at a Tertiary Care Hospital
R. Shruthi1, R. Jyothi2, H.P. Pundarikaksha3, G.N. Nagesh4, T.J. Tushar5
1 Tutor, Department of Pharmacology, Kempegowda Institute of Medical Sciences, BSK-II Stage, Bangalore, Karnataka, India.
2 Associate Professor, Department of Pharmacology, Kempegowda Institute of Medical Sciences, BSK-II Stage, Bangalore, Karnataka, India.
3 Professor and Head, Department of Pharmacology, Kempegowda Institute of Medical Sciences, BSK-II Stage, Bangalore, Karnataka, India.
4 Professor, Department of Medicine, Kempegowda Institute of Medical Sciences, BSK-II Stage, Bangalore, Karnataka, India.
5 Tutor, Department of Pharmacology, Kempegowda Institute of Medical Sciences, BSK-II Stage, Bangalore, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. R. Jyothi, Associate Professor, Pharmacology, No-301, Sri Sai Ram Enclave, Uttarahalli Main Road, Uttarahalli, Bangalore-61, Karnataka, India.
E-mail: sanjyothi03@gmail.com
Introduction
Geriatric population is more prone for various chronic and recurrent illnesses like diabetes mellitus, hypertension, IHD, arthritic, neurodegenerative, gastrointestinal, ocular, genitourinary, respiratory disorders etc., which may require chronic medication with multiple drugs. Poor compliance in this age group accounts for medication wastage with increased cost of healthcare and substantial worsening of the disease with disability or death. Most of the human and economic costs associated with non adherence can be avoided by improving medication adherence.
Aim
To assess the level of medication compliance in elderly patients with chronic illnesses and to analyse the factors influencing medication compliance.
Materials and Methods
The study subjects were assessed by using twenty item structured questionnaires as per modified Morisky Medication Adherence Scale (MMAS).
Results
A total of 251 subjects of geriatric age group with chronic illnesses were assessed for the level of compliance for long term medications. The average number of medications 2.96±1.42 per subject and most of the subjects were receiving FDCs. The compliance level was assessed by way of interview using a twenty item structured pretested questionnaire as per modified MMAS. The level of compliance was good in 45.41%, moderate in 35.45% and poor in 19.12% of the study subjects.
Conclusion
The level of compliance positively correlated with the educational status of the study subjects and their awareness about the diseases and prescribed medications. The overall level of compliance was higher in subjects living with spouse or families, subjects without any functional impairment, subjects who were regular for the follow-up visits and also in subjects who did not experience any adverse events.
Elderly, Medication adherence, Poor compliance
Introduction
The process of aging involves progressive and irreversible decline in organ function that occurs over time even in the absence of injury, illness, or poor lifestyle like unhealthy diet, lack of exercise, substance abuse, etc., [1]. Currently the aging population is rapidly increasing, particularly in developing regions of the world, due to longer expectancy of life, better healthcare facilities and greater awareness about healthy lifestyle [2]. Because of the progressively increasing geriatric population requiring special care, there is a growing global concern to improve the health care delivery systems, particularly against chronic and recurrent illnesses that occur more commonly during later life such as: diabetes mellitus, hypertension, IHD, arthritic disorders, neurodegenerative disorders, psychiatric illnesses, gastrointestinal disorders, ocular disorders, genitourinary disorders, respiratory disorders etc., which may require chronic medication with multiple drugs. Because of the chronic nature of the disease, the need for multiple drug therapy with complex medication regime, increasing cost of therapy, adverse effects, drug interactions, forgetfulness, lack of familial and social support and care, elderly patients may not be fully compliant to long term medications. In general only 50% of general population has been estimated to adhere to their medications, and this may range from 47 to 100% in elderly [3]. Poor compliance among older persons is a public health concern, as it accounts for adverse outcomes, medication wastage with increased cost of healthcare, and substantial worsening of the disease with increased disability or death [4]. This poses a greater responsibility on the health services especially in developing countries like India; where there is a greater strain on available health infrastructure and delivery systems. Numerous studies have been done in many developed countries to assess the problem and prevalence of poor compliance in geriatric patients [5]. However, few studies have been done in Indian population to assess the problem and the extent of medication compliance in geriatric patients and to analyse the various factors contributing the human and economic costs associated with nonadherence and hence the present study was taken up, to assess the level of medication compliance in elderly patients with chronic illnesses and to analyse the factors influencing medication compliance.
Materials and Methods
This prospective observational study was done to assess the level of medication compliance in elderly subjects with chronic illnesses requiring long term medication. After approval and clearance from the Institutional Ethics Committee, 251 consecutive subjects with chronic illnesses and receiving long term medications visiting the outpatient department of Medicine at Kempegowda Institute of Medical sciences, Hospital and Research Centre, Bangalore were included into the study by the investigator after coordinating and confirming the diagnosis with physician. Study subjects were recruited by purposive sampling method from January 2013 – June 2014 (18 months). Written informed consent was obtained from all the study subjects after fully explaining the study procedure to their satisfaction, in both English and vernacular language. Subjects fulfilling the inclusion criteria were included into the study; Elderly patients of either gender aged >60 years with chronic illnesses receiving long term medications for more than 6 months and willingness to give written informed consent and available for regular follow up visits. Patients with the following conditions were excluded from the study; Newly diagnosed patients with recently started drug treatment, Patients receiving intermittent short course therapy or treatment for recurrent acute illnesses, Infectious diseases such as TB, Leprosy, HIV (supervised treatment procedures covered under national programmes) and patients with malignancies or terminal illnesses.
The compliance to the prescribed medications was assessed by the patients answering the twenty item pretested structured questionnaire as per modified MMAS [6,7], regarding the nature and duration of illnesses, the impact of the diseases on their personal, family and social life, the pattern of therapeutic interventions and the medication history. The patients’ awareness about their illness, the prescribed medications, and their expectations from the drug therapy were recorded. The tolerability to the medications and ongoing therapy and adverse events were also documented. The available medical records of the patients were thoroughly scrutinized to obtain the relevant information about the ongoing drug therapy including the number of drugs used, the name of drugs, the dose, frequency and duration of administration and the cost of medication. The demographic data collected was analysed by using descriptive statistics, namely mean, standard deviation. Significance of the associations of different parameters was evaluated by using Chi-Square test and multinomial logistic regression.
Results
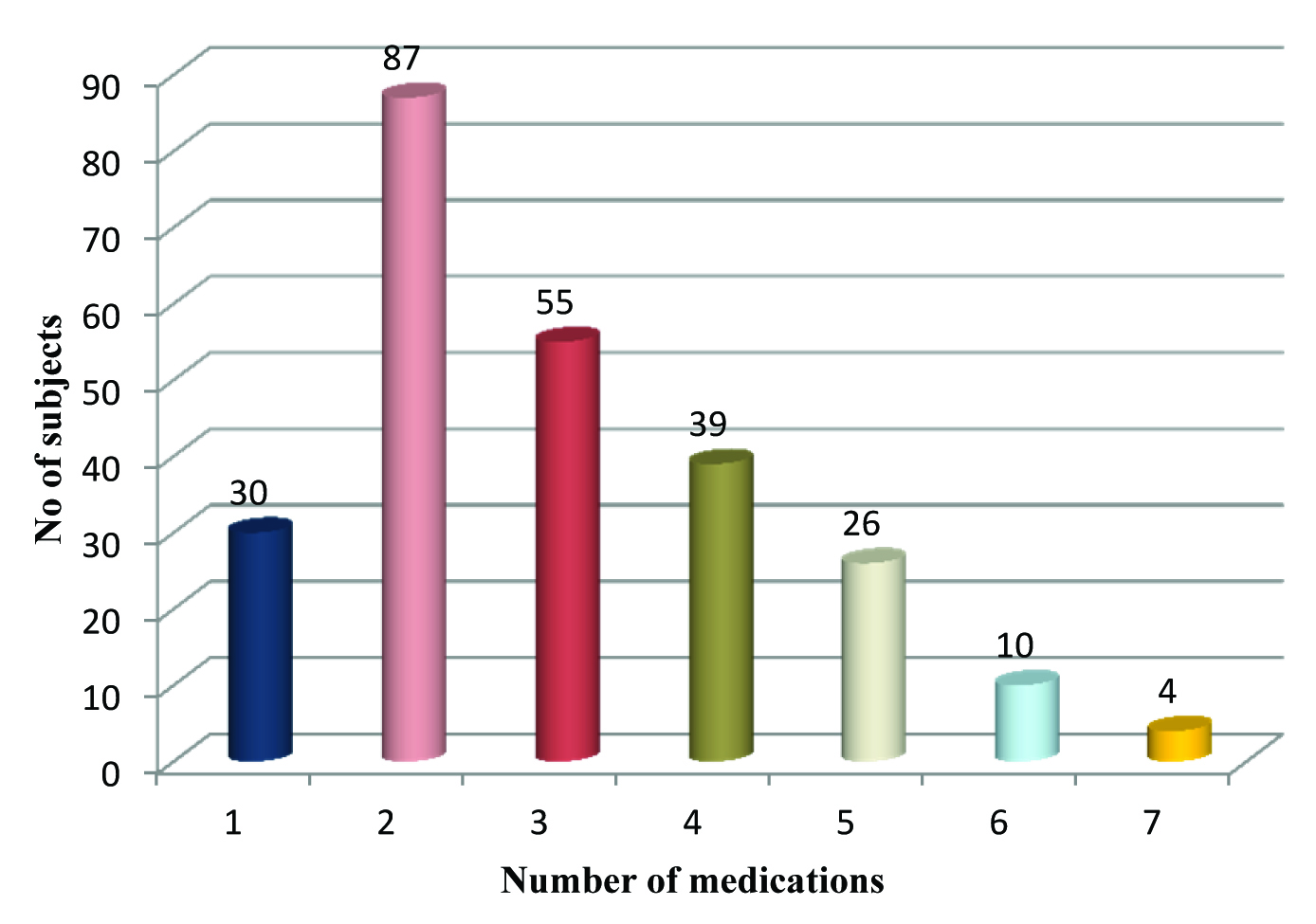
The age and gender distribution in the study subjects is shown in [Table/Fig-1]. The mean age was 66.93±6.55 years. 60.15% of the subjects were male and 39.84% female. [Table/Fig-2] summarizes the chronic illnesses/disease states in the study subjects. The prescribed medications for various illnesses are summarized in [Table/Fig-3]. Since majority of the patients had multiple medical illnesses, different classes of drugs were prescribed either as monotherapy or in combination. Except insulin and inhalational antiasthmatic drugs, all others were oral medications. [Table/Fig-4] shows the number of medications per subject. The Fixed Dose Combinations (FDCs) were considered as single medications. Except 30 subjects, all others were prescribed two or more medications, and the average number of medications per subject was 2.96±1.42. The most commonly prescribed FDCs were glimepride + metformin (n=96), glibenclamide + metformin (n=19), telmisartan + hydrochlorthiazide (n=20) and atenolol + amlodipine (n=12) and aspirin+ atorvastatin (n=16). All the FDCs prescribed are approved and rational. The functional status in the study subjects based on objective assessment has been shown that; majority of the subjects (79.28%) had no functional impairment, 38 had impairment of vision, 6 subjects with hearing impairment, age related memory impairment in 4 subjects, physical disability in 4 subjects and none of the subjects had impairment in speech. The level of compliance to the prescribed medications as assessed by pretested structured questionnaire as per modified MMAS is summarized in [Table/Fig-5]. The factors affecting medication compliance like age, gender, educational status, family income, occupational status, marital status, physical disability, memory, disease states, number of medications and other factors are presented in [Table/Fig-6]. The various reasons for missing the medications are summarized in [Table/Fig-7].
Age & gender distribution.
| Age(years) | Malen (%) | Femalen (%) | Totaln (%) |
|---|
| 60-70 | 103(41.03) | 74(29.48) | 177(70.51) |
| 71-80 | 42(16.73) | 20(7.96) | 62(24.70) |
| >81 | 06(2.39) | 06(2.39) | 12(4.78) |
| Total | 151(60.15) | 100(39.84) | 251(100) |
| Mean±SD | 66.90±6.57 | 66.03±6.61 | 66.93±6.55 |
(n=251)
Disease states/ illnesses.
| Disease states/Illnesses* | Number of subjects |
|---|
| Hypertension | 199 |
| Diabetes Mellitus | 187 |
| Ischemic heart disease† | 39 |
| Cerebrovascular disease ‡ | 05 |
| Obstructive airway diseases§ | 22 |
| Chronic renal disease|| | 06 |
| Epilepsy** | 04 |
| Thyroid disorders†† | 10 |
| Psychiatric disorders | 01 |
| Arthritic disorders | 01 |
| Gastrointestinal disorders | 01 |
| Parkinsonism | 01 |
| Anaemia | 01 |
| Peripheral vascular disorders | 02 |
*181 subjects had multiple (two or more) diseases
† 3 subjects also had cardiac failure
‡With history of stroke
§Bronchial asthma (n=15); COPD (n=7)
||2 subjects maintained on dialysis
** Tonic clonic epilepsy
†† hypothyroidism (n=9), Harshimoto’s disease (n=1)
Prescribed medications/ongoing therapy.
| Therapeutic class | Drugs prescribed* | No. of subjects |
|---|
| Anti diabetic drugs | Insulin | 20 |
| Oral antidiabetics | 139 |
| Insulin + oral antidiabetic drugs | 30 |
| Antihypertensives | Calcium channel blockers | 68 |
| ACE inhibitors | 11 |
| Angiotensin receptor blockers | 40 |
| Beta blockers | 22 |
| Alpha blockers | 06 |
| Combinations | 51 |
| Drugs used in IHD | Nitrates | 8 |
| Metoprolol and carvediolol | 10 |
| ACEIs | 20 |
| Statins | 50 |
| Antiplatelet drugs | 55 |
| Digoxin | 03 |
| Bronchodilators | Salbutamol (inhalation) | 10 |
| Tiotropium and ipratropium (inhalation) | 03 |
| Theophylline | 07 |
| Inhalational corticosteroids | 06 |
| Thyroid hormones | Levothyroxine | 10 |
| Diuretics | Furosemide | 08 |
| Antiepileptics | Phenytoin | 01 |
| Phenobarbitone | 02 |
| Clobazam | 01 |
| NSAIDs & DMARDs | Diclofenac, aceclofenac & HCQS | 04 |
| Antipsychotics | Olanzapine + trihexyphenydil+clonazepam | 01 |
| Antiparkinsonism drugs | Levodopa+carbidopa | 01 |
(n=251)
*Except insulin & inhalational antiasthmatic drugs, all were oral medications
Number of medications per subject
| Level of Compliance* | n (%) |
|---|
| Good | 114(45.41) |
| Moderate | 89 (35.45) |
| Poor | 48 (19.12) |
(n=251)
*Assessed by pretested structured questionnaire as per modified Morisky Adherence Scale: 0 - 5 (very poor); 6-10 (poor); 11-15 (moderate); 16-20 (good)
Factors affecting medication compliance.
| Factor/variable | Compliance level | p-value* |
|---|
| Poor | Moderate | Good |
|---|
| Age | 60-70 | 23(12.99) | 56(31.63) | 98(55.36) | <0.05 |
| 71-80 | 21(33.87) | 25(40.32) | 16(25.80) |
| >81 | 4(33.33) | 8(66.66) | 0(0.00) |
| Gender | Male | 25(16.55) | 50(33.11) | 76(50.33) | 0.141 |
| Female | 23(23.00) | 39(39.00) | 38(38.00) |
| Educational status | Illiterate | 21(33.33) | 22(34.92) | 20(31.74) | 0.002 |
| Pre/Middle/High school | 26(15.75) | 56(33.93) | 83(50.30) |
| Diploma/Graduate/PG | 01(4.54) | 11(50) | 10(45.45) |
| Professional/Honors | 0(0.0) | 0(0.0) | 1(100) |
| Family income | 1000-10000 | 20(18.18) | 36(32.72) | 54(49.09) | 0.737 |
| >10000 | 28(19.85) | 53(37.58) | 60(42.55) |
| Family status | Living alone | 20(52.63) | 11(28.94) | 7(18.42) | 0.001 |
| With spouse | 17(13.93) | 36(29.50) | 69(56.55) |
| With family | 11(12.08) | 42(46.15) | 38(41.75) |
| Functional status | No impairment | 24(12.06) | 69(34.67) | 106(53.26) | 0.001 |
| Impairment of vision | 17(44.73) | 14(36.84) | 7(18.42) |
| Hearing impairment | 2(33.33) | 2(33.33) | 2(33.33) |
| Memory impairment | 2(50.00) | 2(50.00) | 0(0.00) |
| Physical disabilty | 1(25) | 3(75.00) | 0(0.00) |
| No of illnesses | Single | 2(2.85) | 20(28.57) | 48(68.57) | 0.001 |
| Multiple | 46(25.41) | 69(38.12) | 66(36.46) |
| No of medications | Upto 3 | 16(9.30) | 58(33.72) | 98(56.97) | 0.001 |
| >3 | 32(40.50) | 31(39.24) | 16(20.25) |
| Awareness about the diseases | Yes | 38(15.96) | 86(36.13) | 114(47.89) | 0.001 |
| No | 10(76.93) | 3(23.07) | 0(0.00) |
| Side effects | Yes | 17(36.95) | 18(39.13) | 11(23.91) | <0.005 |
| No | 31(15.12) | 71(34.63) | 103(50.24) |
*Evaluated by Chi -square test and multinomial logistic regression.
Reasons for missing the medications.
| Reasons | Number of subjects |
|---|
| Forgetfulness | 14 |
| Polypharmacy | 9 |
| Complexity of regime | 6 |
| Lack of time | 4 |
| Side effects/Adverse events | 3 |
| Dependency on caretaker | 1 |
| Financial constraints | 3 |
| Non availability of medications | 7 |
| Negligence | 2 |
Discussion
In the present study 251 subjects of geriatric age group with chronic illnesses were assessed for the level of compliance for long term medications and the various factors influencing medication compliance were analysed. The level of compliance was good in 45.41%, moderate in 35.45% and poor in 19.12% of the subjects. The level of compliance observed in the present study was in accordance with the observations made in some of the other studies [8,9]. Good compliance was observed in 55.36% of the subjects in the age group of 60-70 years, 25.80% in the age between 71-80 years and none of the subjects above 81 years. The level of compliance was poor in 12.99% of the subjects of 60-70 years age group and 33.87% in the age above 71 years. These observations suggest that the compliance level has decreased progressively with increasing age, with statistically significant difference (p<0.05). Thus, it appears that age may be an important factor which may affect the medication compliance, probably because of the age related functional decline. Similar observations were made in other studies [10,11], however some studies have suggested that age as such may not be an important contributing factor [12]. There was a positive correlation between educational status and compliance level, and the difference was statistically significant (p=0.002). However the difference in the poor and moderate level of compliance between the groups was not statistically significant. Other studies have also shown a positive correlation between educational status and compliance level [13–15]. Hence it can be presumed that the education may play a definite role in improving medication compliance by making the subjects to understand better regarding the nature of their disease, the importance of treatment, physician’s instructions and advice. One of the factors which may determine the affordability for the healthcare services and medication adherence is the financial status of the study subjects or their family, health insurance coverage and facilities for reimbursement. However in the present study the family income had not influenced the medication compliance in the study subjects and there was no statistically significant difference in the different levels of compliance (p=0.737). But most of the subjects (23 out of 25) who had insurance coverage showed good compliance. Some studies have shown increased compliance in subjects with good family income [10,16]. The compliance level was much higher in those subjects living with spouse or with family compared to those living alone. The difference in the level of compliance was statistically significant (p=0.001). Similar observation was made in one of the previous study [17]. However, other studies have not found any positive correlation between family status and compliance [5,18].
Regarding the functional status and compliance, difference in the level of compliance in different groups was highly significant (p=0.001). Other studies have reported higher occurrence of poor compliance or non compliance in subjects with functional impairment particularly related to vision [15]. Probably because of inability to read medication related written instructions in the prescription and the package inserts of the formulations. Good compliance was seen in subjects with single illness compared to multiple illnesses, and the difference was highly significant (p=0.001). Similar observations were made in previous study [19,20]. The number of illnesses has a direct correlation with medication adherence as the subjects with multiple illnesses obviously require a higher number of medications with complex dosing regime and increased medication costs. As against this subjects with a single illness are more likely to be compliant because of simpler dosing regime requiring less number of medications. In our study, we also noticed that, the compliance level was low in subjects with multiple illnesses of longer duration, receiving multiple medications, more frequent administration and also with increasing cost of medications. Subjects with good ability to recall medications showed a high level of compliance. The awareness among the study subjects about their illnesses and prescribed medications showed a positive correlation with the level of compliance. The subjects who were regular for the follow-up visits generally showed better medication compliance and also the compliance was better in those who did not experience any side effects or adverse events. In general the low level of compliance was generally related to advancing age, lack of family and social support, functional impairment, multiple illnesses of long duration, multiple medications with complex regime, poor ability to recall, lack of proper awareness about their illnesses and medications and occurrence of adverse effects. The missing of the medications was mainly attributed to polypharmacy, complexity of regime, forgetfulness, financial constraints and nonavailability of the medications.
A detailed analysis of the different factors which may influence the medication compliance in elderly subjects can help to address the specific problems and issues responsible for poor compliance, particularly when such patients are left for self administration. Since the optimum therapeutic outcome involves a good patient compliance to the prescribed medications, effective measures to ensure a high level of compliance are to be implemented. The patient compliance can be improved by reducing the number of medications, simplifying the regime, less frequent dosing, use of long acting formulations, FDCs, cost-effective medications, avoiding the troublesome side effects/adverse events, proper motivation of the patients and their caregivers for regular follow-up and also by effective patient education and counseling to create a proper awareness about their disease states and medications. Use of special methods, techniques and devices (like pill count method, medication calendar, special medication containers, drug reminder packaging, such as weekly pillboxes or multidrug punch cards etc.,), involving the active role of patients, healthcare providers, healthcare system, the family and community may also contribute to significantly improve the compliance.
Limitation
As it is a hospital based study extrapolation is not possible and the study may not be representative of patients from all socioeconomic backgrounds.
Conclusion
This study confirms the existence of poor compliance to the prescribed medication among geriatric subjects with chronic diseases. However, there was variation in the reported rates of level of compliance (poor/moderate/good compliance), probably due to differences in the study methods. Overall only few studies have been conducted in developing countries on medication compliance, factors influencing the medication compliance and the magnitude of the impact of non-compliance and hence there is a need for more systematic studies.
(n=251)
*181 subjects had multiple (two or more) diseases
† 3 subjects also had cardiac failure
‡With history of stroke
§Bronchial asthma (n=15); COPD (n=7)
||2 subjects maintained on dialysis
** Tonic clonic epilepsy
†† hypothyroidism (n=9), Harshimoto’s disease (n=1)
(n=251)
*Except insulin & inhalational antiasthmatic drugs, all were oral medications
(n=251)
*Assessed by pretested structured questionnaire as per modified Morisky Adherence Scale: 0 - 5 (very poor); 6-10 (poor); 11-15 (moderate); 16-20 (good)
*Evaluated by Chi -square test and multinomial logistic regression.
[1]. Besdine RW, Approach to Geriatric Patient Quality of life & Therapeutic Objectives. In: Porter SR, editorThe Merck Manual of Diagnosis & Therapy 2011 19th editionNew JerseyMerck & Co:3262-80.[cited 2014 Jul 25]. Available from: URL http://www.merckmanuals.com/professional/geriatrics/approach_to_the_geriatric_patienu7t/introduction_to_geriatrics.html [Google Scholar]
[2]. United Nations, Department of Economic and Social Affairs, Population Division (2015)World Population Ageing 2015 (ST/ESA/SER.A/390) [Google Scholar]
[3]. Tsai K, Chen J, Wen C, Medication adherence among geriatric outpatients prescribed multiple medicationsThe American Journal of Geriatric Pharmacotherapy 2012 10(1):61-68. [Google Scholar]
[4]. Osterberg L, Blaschke T, Adherence to medicationNew England Journal of Medicine 2005 353:487-97. [Google Scholar]
[5]. Jin J, Sklar G, Oh V, Li SH, Factors affecting therapeutic compliance: A review from the patient’s perspectiveTherapeutics and Clinical Risk Management 2008 4(1):269-86. [Google Scholar]
[6]. Morisky DE, Ang A, Krousel-Wood M, Ward JH, Predictive validity of a medication adherence measure in an outpatient settingJ Clin Hypertens 2008 10(5):348-54. [Google Scholar]
[7]. Lam WY, Fresco P, Medication Adherence Measures: An OverviewBio Med Research International 2015 2015:21704712 pages, 2015 [Google Scholar]
[8]. Blenkiron P, The elderly and medication: understanding and compliance in a family practicePostgrad Medical Journal 1996 72:671-76. [Google Scholar]
[9]. Tiv M, Viel JF, Mauny F, Eschwège E, Weill A, Fournier C, Medication adherence in Type 2 Diabetes: The ENTRED study 2007, a French population based studyPLoS One. [serial online] 2012 [cited 2014 Jul 15] 7(3)Available from: URL: http://www.plosone.org/article/fetchObject.action?uri=info%3Adoi%2F10.1371%2Fjournal.pone.0032412&representation=PDF [Google Scholar]
[10]. Benner JS, Glynn RJ, Mogun H, Neumann PJ, Weinstein MC, Avorn J, Long-term persistence in use of statin therapy in elderly patientsJAMA 2002 288(4):455-61. [Google Scholar]
[11]. Okuno J, Yanagi H, Tomura S, Oka M, Hara S, Hirano C, Compliance and medication knowledge among elderly Japanese home-care recipientsEuropean Journal of Clinical Pharmacology 1999 55(2):145-49. [Google Scholar]
[12]. Lorenc L, Branthwaite A, Are older adults less compliant with prescribed medication than younger adults?Br J Clin Psychol 1993 32(4):485-92. [Google Scholar]
[13]. Nichols G, Poirier S, Optimizing adherence to pharmaceutical care plansJournal of American Pharmaceutical Association 2000 40(4):475-85. [Google Scholar]
[14]. Ho PM, Bryson C, Rumsfeld JS, Medication adherence: its importance in cardiovascular outcomesCirculation Journal of the American Heart Association 2009 119:3028-35. [Google Scholar]
[15]. Maclaughlin EJ, Raehl CL, Treadway AK, Sterling TL, Zoller DP, Bond CA, Assessing medication adherence in the elderly: Which tools to use in Clinical practice?Drugs aging 2005 22(3):231-55. [Google Scholar]
[16]. Breissacher BA, Gurwitz JH, Soumeral SB, Patient at risk for cost related med nonadherence: A Review of the literatureJ Gen Intern Med 2007 22:864-71. [Google Scholar]
[17]. Shams MEE, Barakat EAM, Measuring the rate of therapeutic adherence among outpatients with T2DM in EgyptSaudi Pharm J 2010 18(4):225-32. [Google Scholar]
[18]. Spikmans FJ, Brug J, Doven MM, Kruizenga HM, Hoafsteenge GH, Van Bokhorst-vander Schueren MA, Why do diabetic patients not attend appointments with their dietitian?J Hum Nutr Diet 2003 16:151-58. [Google Scholar]
[19]. Ibrahim OH, Jirjees FJ, Mahdi HJ, Barriers affecting compliance of patients with chronic diseases: a preliminary study in United Arab Emirates (UAE) populationAsian Journal of Pharmaceutical and Clinical Research 2011 4(Suppl 2):42-45. [Google Scholar]
[20]. Ioana Dana A, Simona S, Paula B, Laura O, Radu Ionut R, Gabriel U, Non compliance in a large population of elderly patients with cardiovascular diseaseA Journal of Clinical Medicine 2006 1(3):14-18. [Google Scholar]