Balanced Autosomal Translocations in Two Women Reporting Recurrent Miscarriage
Brindha Arumugam1, Chandra R Samuel2, Santhiya Sathiyavedu Thyagarajan3
1 Research Scholar, Department of Genetics, Dr. ALM PG IBMS, University of Madras, Chennai, Tamilnadu, India.
2 Associate Professor, Department of Genetics, Dr. ALM PG IBMS, University of Madras, Chennai, Tamilnadu, India.
3 Professor (Retd.), Department of Genetics, Dr. ALM PG IBMS, University of Madras, Chennai, Tamilnadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Santhiya Sathiyavedu Thyagarajan, Department of Genetics, Dr. ALM PG IBMS, University of Madras, Taramani, Chennai-600113, Tamilnadu, India.
E-mail: v_santhiya63@hotmail.com
Spontaneous abortion or loss of fetus prior to 20 weeks of gestation is observed in 15-20% of clinically recognized pregnancies. Recurrent Miscarriage (RM) is defined as three or more consecutive pregnancy losses and it affects 1-2% of women. Parental chromosomal rearrangements account for 2-5% of RM. This report describes two couples with a clinical history of RM who were subjected to conventional cytogenetic analysis to ascertain the chromosomal aetiology. Analysis of GTG-banded metaphases obtained from cultured lymphocytes at approximately 500-band resolution revealed balanced translocation in the female spouses as 46,XX,t(8;11)(p11.2;q23.3) in BR27W and 46,XX,t(5;7)(p15.1;q32) pat in BR49W. Both the male partners exhibited 46,XY karyotype. Fluorescent In Situ Hybridization (FISH) analysis was subsequently carried out to confirm the balanced translocation using suitable whole chromosome paint probes. These balanced chromosomal abnormalities in the parents could be responsible for the repeated fetal losses. Hence, karyotype analysis should be a mandatory etiological investigation for couples with RM towards genetic counselling. Disruption of critical genes through these rearrangements could also underlie the pregnancy outcome.
Chromosomal rearrangement, Fluorescent in situ hybridization, Genetic counseling
Case Report 1 - BR27W
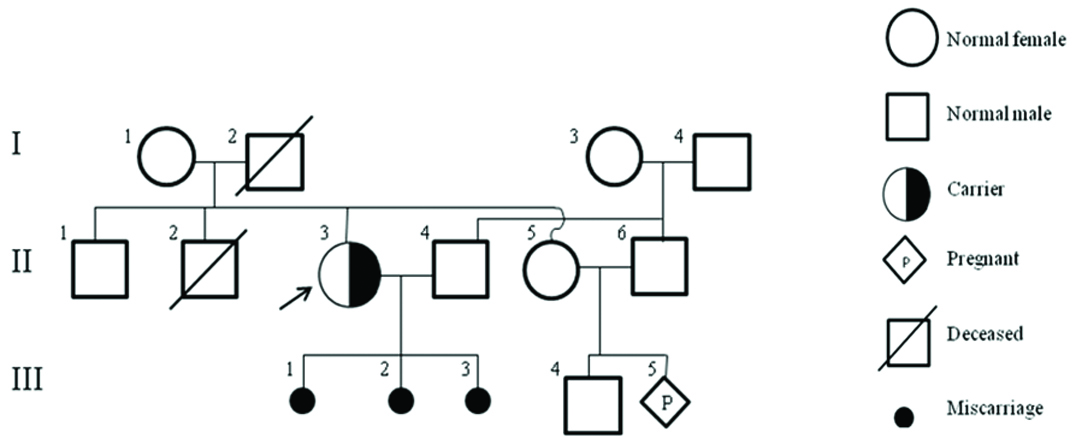
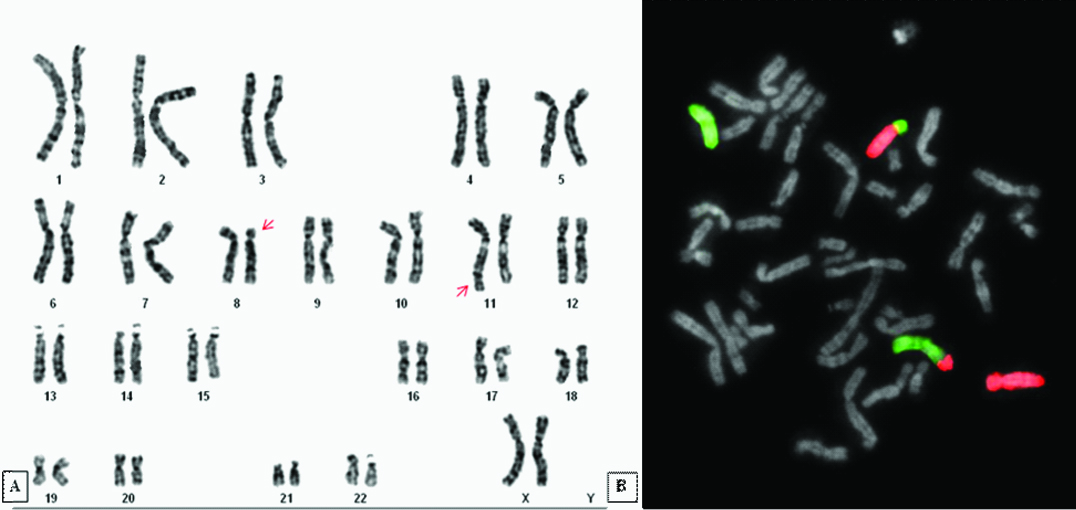
A 29-year-old female (proband) was referred from the Institute of Obstetrics and Gynecology, Chennai with a history of three first trimester miscarriages. She presented no family history of either miscarriages or genetic disorders [Table/Fig-1]. Her age at menarche was 15 years and had regular menstrual cycles. Ultrasound imaging revealed bilateral polycystic ovaries (RO: 4.3 x 2.3cm; LO: 4.4 x 2.2cm) and normal uterus (7.4 x 4.1 x 4cm). Hormonal profiles were normal (FSH 7.93mIU/ml; LH 3.97mIU/ml; Estradiol 77.9pg/ml). Laboratory investigations were carried out to exclude TORCH infection and anti-phospolipid syndrome. The study was approved by the Institutional Human Ethical Committee (UM/IHEC/06-2014-II). After obtaining written informed consent from the couple, cytogenetic analysis was performed on GTG-banded metaphases at 400-500 band level resolution using Applied Spectral Imaging Systems karyotyping software (BandView version 6.0) as per standard protocols. The abnormalities were designated following ISCN 2013 [1] guidelines. The husband exhibited a normal 46,XY karyotype while the female partner (BR27W) showed a balanced translocation as 46,XX,t(8;11)(p11.2;q23.3) [Table/Fig-2a]. Fluorescence In Situ Hybridization (FISH) analysis using Whole Chromosome Paint (WCP) probes for chromosomes 8 and 11 with Applied Spectral Imaging Systems FISH software (FISH View version 6.0) confirmed the chromosomal re-arrangement [Table/Fig-2b]. The proband’s family denied consent for further study aimed to resolve the origin of the translocation.
Pedigree of Case Report 1 (BR27W).
a) GTG-banded karyogram showing the translocation t(8;11) (indicated by arrows) in the wife BR27W; b) FISH using WCP8 (red) and WCP11 (green) probes confirmed the translocation.
Case Report 2 - BR49W
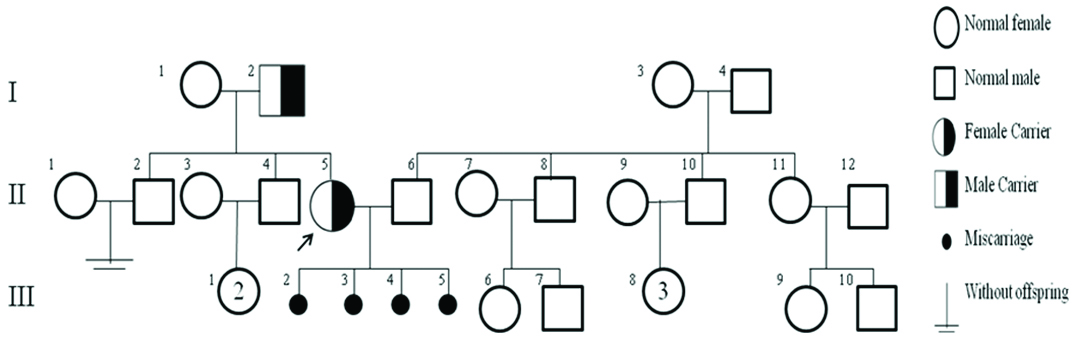
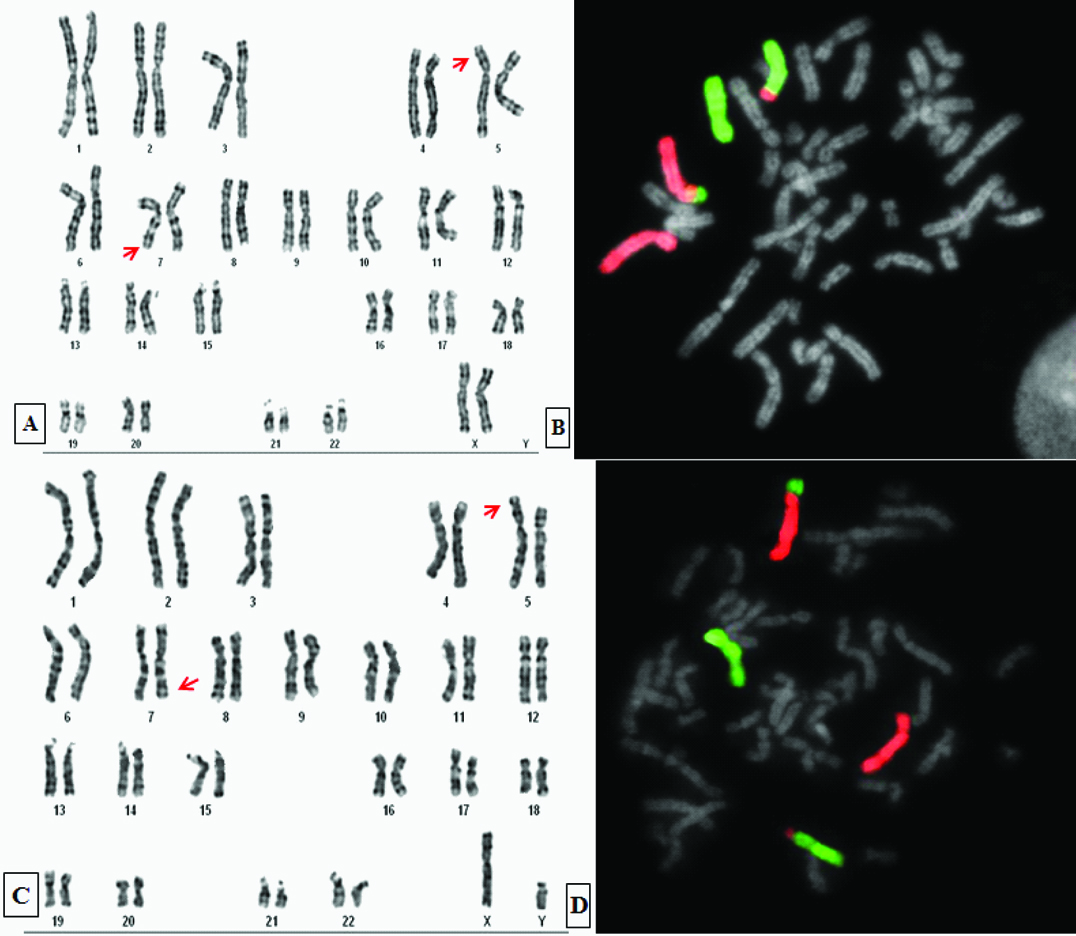
A 26-year-old female gave a history of four miscarriages, all in second trimester, although there was no family history of abortions [Table/Fig-3]. She experienced regular menstrual cycles since, the age of 16 years. Endocrine profiling revealed slightly elevated level of TSH (7.12μIU/ml) and normal total T3 (201ng/dl) and total T4 (12.66ug/dl). Investigations ruled out TORCH infection and anti-phospholipid syndrome. Written informed consent was obtained from the couple. A balanced translocation 46,XX,t(5;7)(p15.1;q32) observed in the wife (BR49W) [Table/Fig-4a] was confirmed through FISH employing WCP probes for chromosomes 5 and 7 [Table/Fig-4b]. Extended chromosomal analysis of her parents established her father also to be a carrier of the denoted translocation [Table/Fig-4c,d]. Of her two brothers, one was infertile (II-2) and the other has two daughters (II-4) but they did not cooperate for this study. Her husband and mother had normal karyotype.
Pedigree of Case Report 2 (BR49W).
GTG-banded karyogram showing the translocation t(5;7) (arrows) (a) in the patient BR49W which was confirmed by FISH using WCP5 (red) and WCP7 (green) probes (b); GTG-banded karyogram (c) and metaphase FISH using WCP probes (d) from her father exhibiting the same translocation.
Discussion
Recurrent Miscarriage (RM) is defined as three or more consecutive pregnancy losses prior to 20 weeks of conception and is observed in 1-2% of women [2]. However, two pregnancy losses also prompt the diagnosis of RM as recurrence rates and risk factors are fairly similar [3,4]. Several etiologies besides age such as genetic, anatomical, endocrine, immunologic, environmental and life-style risk factors contribute to ~50% of the cases [4]. Fetal chromosomal abnormalities cause about 70% of sporadic miscarriages while they lead to only a relatively smaller fraction of pregnancy losses in RM couples [3].
Parental structural chromosomal rearrangements have been reported in 2-5% couples with RM [2,4]. These anomalies include reciprocal and Robertsonian translocations, inversions, insertions and mosaicism [2]. Robertsonian translocations account for 35% of the cases carrying a translocation, while 65% are of reciprocal type [5]. Reciprocal translocations, found in one out of 500 people, do not produce any phenotypic effects but usually result in RM, offspring with chromosomal abnormalities or infertility in the carriers [6]. When a parent carries a balanced translocation, there is a 4% risk of unbalanced translocation in the fetus [5]. The chromosome arms 2q, 5q, 7p, 7q, 12q, 13q, 17q, 18q and 22q were preferentially involved in RM [6]. In addition to size of the chromosomal segment, the position and frequency of the break points also play a critical role [7]. The risk of RM doubles when one partner is a carrier [8]. Low maternal age, history of RM and family history of RM increase the probability of carrier status [9].
Karyotypic analysis forms a part of diagnostic work-up of couples with RM [4]. Chromosomal anomalies including polymorphic variants have been recorded in 2-12.5% of couples with RM [10,11]. These anomalies trigger meiotic unequal crossing over leading to formation of genetically imbalanced gametes that is lethal to the embryo, causing miscarriage [11]. At meiosis, chromosomes involved in reciprocal translocations form quadrivalent complexes that segregate by alternate, adjacent-1, adjacent-2, 3:1 or 4:0 modes to form gametes with either balanced or imbalanced chromosome complements. Eventually of the 32 possible zygotes only two are genetically normal or balanced [6]. Parents as carriers have 2.9% chance of their offspring born with an imbalanced karyotype and congenital anomalies [10]. There also occurs a gender influence over clinical pathology as inherited balanced chromosomal rearrangements in males cause sterility [7]. The woman BR49W reporting RM in this paper had inherited the translocation from her father.
Varied translocation break points involving the same chromosomes as observed in our probands have been described in couples with RM earlier [Table/Fig-5] [12–16]. Further, chromosomal rearrangements depicting identical loci have also been implicated in RM [Table/Fig-6] [6,13,16–19]. Molecular characterization of these break points would elucidate not only the critical genes responsible for the clinical condition but also unravel the mechanism of inactivation through interruption or by position effect [19]. List of genes located at the translocation breakpoints and their likely role are given in [Table/Fig-7] [20]. Some of them regulate basic cellular processes like response to DNA damage, microtubule assembly, chromosome segregation (CEP164), cell differentiation (PAX4), cell-cell interaction, sperm–egg interaction (ADAM2), cell adhesion (C1QTNF5 and PVRL1), cell senescence (ETS1) and apoptosis [20]. Genes encoding transcription factors (PAX4, ETS), if disrupted could manifest a cascade effect affecting a specific pathway involving an array of genes [Table/Fig-7]. Future efforts integrating studies on skewed X-chromosome inactivation, copy number variations, parental- and tissue- specific imprinted genes and microRNA expression profiling for RM-related tissues would aid in the identification of biomolecular risk factors for RM [3]. It could be speculated that disruption of critical genes through chromosomal rearrangements and their consequent functional impairment possibly results in RM. Therefore, molecular characterization of the breakpoints in future might reveal the candidate genes underlying RM.
Published cases of t(5;7) and t(8;11) associated with Recurrent Miscarriage [12–16]
| Karyotype | Reference |
|---|
| 46,XX,t(5;7)(p15.1;q32) | Present study |
| 46,XY, t(5;7)(p13;p15) | Stephenson and Sierra, [12] |
| 46,XY,t(5;7)(p13;p15) | Chaithra et al., [13] |
| 46,XY,t(5;7)(q13;q22) | Sheth et al., [14] |
| 46,XX,t(5;7)(q13;q32)* | Sheth et al., [15] |
| 46,XX,t(8;11)(p11.2;q23.3) | Present study |
| 46,XX, t(8;11)(q11.23;q24.2) | Stephenson and Sierra, [12] |
| 46,XX,t(8;11)(q11.23;q24.2) | Chaithra et al., [13] |
| 46,XX,t(8;11)(q21;q13) | Sugiura-Ogasawara et al., [16] |
* Single cell abnormality.
Phenotypes reported in cases with identical breakpoints [6,13,16,17,18,19].
| Band | Karyotype | Phenotype | Reference |
|---|
| 5p15 | 46,XX,inv(5)(p15.3q15) | RM | Ghazaey et al., [17] |
| 46,XY,inv(5)(p15.3q35) | RM | Goddijn et al., [18] |
| 46,XY,inv(5)(p15.2p13) | Male infertility | Bugge et al., [19] |
| 46,XY,t(5;12)(p15.1;p12.2) | RM | Chaithra et al., [13] |
| 46,XX,t(5;12)(p15.1;q22) | RM | Goddijn et al., [18] |
| 46,XX,t(X;5)(q22;p15.2) | Female infertility | Bugge et al., [19] |
| 46,XY,t(4;5)(q25;p15.2) | RM | Ghazaey et al., [17] |
| 7q32 | 46,XX,t(1;7)(q32.1;q32) | RM | Chaithra et al., [13] |
| 46,XX,t(2;7)(q37.1;q32) | RM | Ghazaey et al., [17] |
| 46,XX,t(3;7)(q22;q32) | RM | Ghazaey et al., [17] |
| 8p11 | 46,XX,inv(8)(p11.22q13.1) | RM | Goddijn et al., [18] |
| 46,XY,t(8;15)(p11.2;q25) | RM | Sugiura-Ogasawara et al., [16] |
| 11q23 | 46,XX,inv(11)(q21q23) | RM | Goddijn et al., [18] |
| 46,XX,t(11;22)(q23.3;q11.2) | RM | Ogilvie and Scriven [6] |
| 46,XY,t(11;22)(q23.3;q11.2) | RM | Ogilvie and Scriven [6] |
| 46,XX,t(11;22)(q23.3;q11.2) | RM | Ghazaey et al., [17] |
| 46,XX,t(11;22)(q23;q11) | RM | Sugiura-Ogasawara et al., [16] |
| 46,XY,t(11;22)(q23;q11) | RM | Ghazaey et al., [17] |
List of genes at the translocation breakpoints reported in this study [20].
| Gene | Band | Role | Phenotype |
|---|
| ANKH | 5p15.1 | Multipass transmembrane Protein | Craniometaphyseal dysplasia - AD |
| PAX4 | 7q32 | Transcription Factors
Critical role in fetal development and cancer growth Differentiation of insulin producing beta cells
| |
| STAR | 8p11.2 | Acute regulation of steroid hormone synthesis | Congenital adrenal hyperplasia |
| ERlIN2 | 8p11.2 | SPFH domain-containing family of lipid raft-associated proteins | Spastic paraplegia-18 |
| ADAM2 | 8p11.2 | Cell-cell interaction & cell-cell matrix interaction
Fertilization, muscle development and neurogenesis Sperm-egg interaction
| |
| CBL | 11q23.3 | Proto-oncogene | Noonan syndrome-like disorder |
| APOC 3 | 11q23.3 | Apolipoprotein C III | Hypertriglyceridemia due to increased expression |
| ETS1 | 11q23.3 | ETS family of transcription factors (activator/repressor)
Stem cell development Cell senescence and death Tumorigenesis
| |
| HMBS | 11q23.3 | Hydroxymethlylibane super family | Acute intermittent porphyria – AD |
| PVRL1 | 11q23.3 | Adhesion protein | Cleft lip and palate/ ectodermal dysplasia 1 syndrome |
| TMPRSS4 | 11q23.3 | Serine protease family | Multiple human diseases and disorders due to malfunction |
| C1QTNF5 | 11q23.3 | Cell adhesion | Late onset retinal degeneration |
| DPAGT1 | 11q23.3 | Catalytic enzyme | Congenital disorder of glycosylation type Ij |
| CEP164 | 11q23.3 | Centrosomal protein
Microtubule organization DNA damage response Chromosome segregation
| |
| ARCN1 | 11q23.3 | Intra-cellular protein | Multiple disease-associated chromosome translocations |
Conclusion
Karyotype analysis is mandatory for couples with RM to ascertain the chromosomal etiology towards genetic counseling. Further, prenatal diagnosis in every subsequent pregnancy and oocyte or sperm donation followed by preimplantation genetic diagnosis are recommended when a parent proves to be a carrier of chromosomal rearrangement. Alteration of expression of critical genes through these rearrangements could also underlie the pregnancy outcome.
* Single cell abnormality.
[1]. Shaffer LG, McGowan-Jordan J, Schmid M, ISCN (2013) An International System for Human Cytogenetic Nomenclature (2013) - Recommendations of the International Standing Committee on Human Cytogenetic Nomenclature, S. Karger Basel [Google Scholar]
[2]. Ford HB, Schust DJ, Recurrent pregnancy loss: etiology, diagnosis, and therapyRev Obstet Gynecol 2009 2:76-83. [Google Scholar]
[3]. Rull K, Nagirnaja L, Laan M, Genetics of recurrent miscarriage: Challenges, current knowledge, future directionsFront Genet 2012 3:1-13. [Google Scholar]
[4]. Practice Committee of the American Society for Reproductive MedicineEvaluation and treatment of recurrent pregnancy loss: A committee opinionFertil Steril 2012 98:1103-11. [Google Scholar]
[5]. Kiwi R, Recurrent pregnancy loss: Evaluation and discussion of the causes and their managementCleve Clin J Med 2006 73:913-21. [Google Scholar]
[6]. Ogilvie MC, Scriven PN, Meiotic outcomes in reciprocal translocation carriers ascertained in 3-day human embryosEur J Hum Genet 2002 10:801-06. [Google Scholar]
[7]. Sayee R, Preetha T, Aruna N, Rema D, Karyotyping and counseling in bad obstetric history and infertilityIran J Reprod Med 2007 5:7-12. [Google Scholar]
[8]. Mozdarani H, Meybodi AM, Zari-Moradi S, A cytogenetic study of couples with recurrent spontaneous abortions and infertile patients with recurrent IVF/ICSI failureIndian J Hum Genet 2008 14:1-6. [Google Scholar]
[9]. Jauniaux E, Farquharson RG, Christiansen OB, Exalto N, Evidence-based guidelines for the investigation and medical treatment of recurrent miscarriageHum Reprod 2006 21:2216-22. [Google Scholar]
[10]. Dubey S, Chowdhury MR, Prahlad B, Kumar V, Mathur R, Hamilton S, Cytogenetic causes for recurrent spontaneous abortions - An experience of 742 couples (1484 cases)Indian J Hum Genet 2005 11:94-98. [Google Scholar]
[11]. Pokale YS, Khadke P, Cytogenetic studies of recurrent miscarriage- A reviewISRR 2016 4:1-18. [Google Scholar]
[12]. Stephenson MD, Sierra S, Reproductive outcomes in recurrent pregnancy loss associated with a parental carrier of a structural chromosome rearrangementHum. Reprod 2006 21:1076-82. [Google Scholar]
[13]. Chaithra PT, Malini SS, Kumar CS, An overview of genetic and molecular factors responsible for recurrent pregnancy lossInt J Hum Genet 2011 11:217-25. [Google Scholar]
[14]. Sheth FJ, Liehr T, Kumari P, Akinde R, Sheth HJ, Sheth JJ, Chromosomal abnormalities in couples with repeated fetal loss: An Indian retrospective study 2013 19:415-22. [Google Scholar]
[15]. Sheth F, Pani J, Desai M, Sheth J, Single cell abnormality in couples with bad obstetric history and repeated fetal loss: Occurrence and clinical outcomeInt J Hum Genet 2011 11:259-63. [Google Scholar]
[16]. Sugiura-Ogasawara M, Ozaki Y, Sato T, Suzumori N, Suzumori K, Poor prognosis of recurrent aborters with either maternal or paternal reciprocal translocationsFertil Steril 2004 81:367-73. [Google Scholar]
[17]. Ghazaey S, Keify F, Mirzaei F, Maleki M, Tootian S, Ahadian M, et al. Chromosomal analysis of couples with repeated spontaneous abortions in Northeastern IranFertil Steril 2015 9:47-53. [Google Scholar]
[18]. Goddijn M, Joosten JH, Knegt AC, Franssen MT, Bonsel GJ, Leschot NJ, Clinical relevance of diagnosing structural chromosome abnormalities in couples with repeated miscarriageHum Reprod 2004 19:1013-17. [Google Scholar]
[19]. Bugge M, Bruun-Petersen G, Brøndum-Nielsen K, Friedrich U, Hansen J, Jensen G, Disease associated balanced chromosome rearrangements: a resource for large scale genotype-phenotype delineation in manJ Med Genet 2000 37:858-65. [Google Scholar]
[20]. https://www.ncbi.nlm.nih.gov/gene/ [Google Scholar]