Cerebral Venous Thrombosis in Pregnancy-A Poignant Allegory of an Unusual Case
Sheeba Marwah1, Gaikwad Harsha Shailesh2, Sumedha Gupta3, Manjula Sharma4, Pratima Mittal5
1 Research Officer, Department of Obstetrics and Gynecology, VMMC and Safdarjung Hospital, New Delhi, India.
2 Professor, Department of Obstetrics and Gynecology, VMMC and Safdarjung Hospital, New Delhi, India.
3 Postgraduate Student, Department of Obstetrics And Gynecology, VMMC and Safdarjung Hospital, New Delhi, India.
4 Professor and Consultant, Department of Obstetrics and Gynecology, VMMC and Safdarjung Hospital, New Delhi, India.
5 Professor and Head, Department of Obstetrics and Gynecology, VMMC and Safdarjung Hospital, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sheeba Marwah, Research Officer, Department of Obstetrics and Gynecology, VMMC and Safdarjung Hospital, New Delhi-11129, India.
E-mail: sheebamarwah@yahoo.co.in
Cerebral Venous Thrombosis (CVT), also known as cortical venous, cerebral sinus, cerebral venous sinus, or dural sinus thrombosis, is an infrequent grave condition affecting pregnant females, resulting from clot formation in one of the many outflow tracts of the brain. Although pregnancy-associated stroke or CVT is uncommon, the risk of stroke is greatly increased above the low baseline rate in young patients during late pregnancy and, even more so, during the puerperium. Haemorrhagic infarction can occur in the acute stage of CVT. The article reports a case of CVT in puerperium in woman without any risk factors for thrombosis, highlighting the difficulties encountered in differentiating this rare cause from common diagnoses such as eclampsia. Also, clinical considerations and relevant literature review on prognostic factors affecting outcome have been addressed. CVT is an uncommon serious neurologic disorder in young gravidas requiring prudent assessment of the potential differential diagnoses and prompt management.
Management, Neurologic disorder, Stroke
Case Report
A 22-old-year P1L1 postpartum day seven was brought to gynaecology emergency with complaints of multiple episodes of seizures since, one day. She also had a continuously aggravating postural headache, predominantly located in the neck and both eyes. However, there was no history of fever. She had a full term vaginal delivery by a midwife (dai) at home seven days back, without any complications. There was no history of high blood pressure during pregnancy.
On examination at admission, she was conscious but drowsy with a Glasgow Coma Scale of E4V2M6. She was normotensive, afebrile, respiratory rate of 18/min, pulse rate 100/minute good volume. There was no albuminuria. Chest and cardiovascular system were essentially normal. On abdominal examination, uterus was well-involuted; local examination showed healthy lochia.
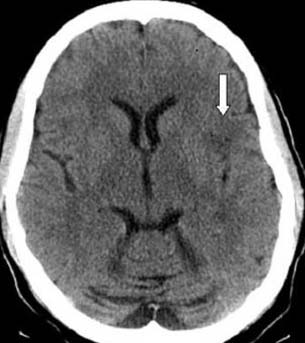
She was admitted in high dependency unit of the department and put on continuous maternal surveillance. She was administered loading dose of intravenous phenytoin followed by maintenance dose. All relevant blood investigations were sent. Intensive care and neurological referrals were taken and further examination showed no neurological deficit. Ultrasound whole abdomen revealed normal postpartum uterus with no pelvic collection. Her blood pressure remained normal throughout. Laboratory examination showed a normal complete blood count with haemoglobin 9.8mg/dl and normal renal, hepatic, and coagulation profiles. High vaginal swab showed infection with Escherichia coli and her antibiotics were changed as per sensitivity report. But she again convulsed, and hence, was put on injectable lorazepam 0.4mg as and when required. Fundal examination showed normal disc and non-contrast computed tomography scan of head showed white matter oedema in left frontal lobe [Table/Fig-1].
Non contrast computed tomography of head showing frontal lobe infarct.
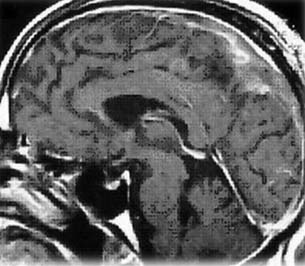
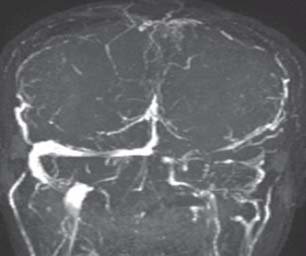
Based on her persistent altered sensorium, Magnetic Resonance Imaging (MRI) of the brain and Magnetic Resonance Venogram (MRV) [Table/Fig-2,3] were done which revealed superior sagittal sinus thrombosis with frontal venous infact. Treatment with mannitol was commenced immediately to control intra-cranial hypertension and dose-adjusted low-molecular-weight heparin was started to maintain activated partial thromboplastin time between 1.5 and 2.0 times of control value. Also, Colour Doppler of bilateral lower limbs was performed that revealed right sided deep vein thrombosis at distal femoral vein and popliteal veins, with recanalization of veins and thrombosis in great saphenous vein and small saphenous veins of lower half of leg.
MRI brain T1 weighted image of the patient showing saggital sinus thrombosis.
Magnetic Resonance Venogram (MRV) of the patient showing saggital sinus thrombosis and left transverse sinus thrombosis as evidenced by empty delta sign.
Anti-coagulation with high-dose warfarin and injectable neurocetam was then initiated. Blood tests showed elevated D-dimers (3.39μg/ml) that gradually decreased after re-adjusting the anticoagulation dose in liaison with cardiologist. Gradually, with continuous monitoring, her condition improved and was subsequently started on oral drugs. She was then discharged in stable condition 20 days of admission on anti-epileptic, anti-coagulants.
She’s been following up regularly with cardiology and neurology departments since discharge, and is convalescing well.
Discussion
Pregnancy and postpartum period is a high-risk phase for innumerable complications in a woman’s lifetime, because of re-disposition of the maternal cardiovascular circulation, particularly third trimester of pregnancy and the first four weeks postpartum [1-5]. In addition, neurological symptoms like headache befall, often instigated by sleep deprivation, irregular food intake, or dehydration. All these factors along with the hormonal vacillations in oestrogen levels may result in postpartum headache and clouding of consciousness [6-9].
Diagnosis can be easily muffed with other common causes of headache or seizure presenting with similar clinical features in pregnancy. It was the same in our case. However, the most frequent symptom is constant or postural headache (70–88%) [10]. Symptoms may also include dizziness, nausea, vomiting, blurred vision, neurologic signs, papilloedema, lethargy, seizures, and coma [4,11]. It usually increases gradually over a couple of days, but it can also start rapidly while mimicking a subarachnoid haemorrhage. The specific presentation depends on location and extent of the thrombosis, the degree of collateral venous circulation, and the presence of associated cortical lesions. Signs of cerebral hernia can appear in patients with mass effects, such as oedema, infarction and haemorrhage. In addition, symptoms may fluctuate as thrombosis and fibrinolysis occurs simultaneously, leading to changes in surrounding blood flow and intracranial pressure [12]. The presented case is an example for possible symptom fluctuation as after amelioration of the headache, she developed seizures and signs of thrombus organization. However, unlike usual cases of occlusion of sagittal sinus, focal neurological deficits leading to paraperesis/paraplegia were conspicuously absent in the concurrent case.
Largely patients with Cerebral Venous Thrombosis (CVT) have a substantially benign prognosis with low mortality rates (5.6% in acute phase; 9.4% after 12 months) [13]. Most women attain a complete recovery. Many risk scores have been formulated by researchers in past to predict the outcome of patients with CVT and have been proven to be quite accurate for the same [14].
In absence of haemorrhage or infarction the, findings of CVT on an non-enhanced CT are very indiscernable [15]. Also being non-invasive and non-ionizing, a combination of MRI brain and MRV become the modality of choice for the investigation of suspected CVT in pregnant women [10,16]. In the present case though D dimer assays were high, their use as a diagnostic marker has been explored only in small studies with non-conclusive results [16].
The treatment of CVT is predominantly supportive, although endovascular thrombolysis and surgical thrombectomy are mulled over in women who are resistant to anti-coagulation therapy, have worsening of symptoms, do not have intra-cranial haemorrhage and are not at risk for impending herniation [17]. Vitamin-K antagonists like warfarin remain the drug of choice for the long term, secondary prevention of CVT. Evidence suggests use of maintenance anti-coagulation for a period of 3 months in presence of high risk factors and for 6–12 months in patients with idiopathic cases and women with mild hereditary thrombophilias. Indefinite anti-coagulation should be contemplated in patients with recurrent episodes of CVT and in those with a simple episode of CVT along with concomitant ‘severe’ Thrombophilia. In the extant case, the patient received intravenous heparin and warfarin for 12 months. Afterwards, the therapy was modified to lifelong low-dose anticoagulation.
Conclusion
CVT is a rare entity presenting with a wide conglomeration of symptoms. This case shows the rare coincidence of suspected postpartum eclampsia and a CVT. This vivid description emphasizes the significance of carefully evaluating potential differential diagnoses of headache and seizures in the postpartum period and the difficulty of discerning unusual from customary conditions. This case also accentuates the importance of interdisciplinary alliance for provision of optimal care to such women in the peripartum period. An MRI combined with MRV may be the best choice for the investigation of a suspected CVST in a pregnant woman.
[1]. Shah M, Agarwal N, Gala NB, Prestigiacomo CJ, Gandhi CD, Management of dural venous sinus thrombosis in pregnancyEJVES Short Reports 2014 27(5):e41-2. [Google Scholar]
[2]. Bansal BC, Prakash C, CVTJournal of Indian Academy of Clinical Medicine 1999 5(1):55-61. [Google Scholar]
[3]. Cole B, Criddle LM, A case of postpartum cerebral venous thrombosisJ Neurosci Nurs 216 38(5):350-53. [Google Scholar]
[4]. Nie Q, Guo P, Ge J, Qiu Y, Cerebral venous sinus thrombosis with cerebral haemorrhage during early pregnancyNeurosciences 2015 20(1):48-51. [Google Scholar]
[5]. Saposnik G, Barinagarrementeria F, Brown Jr RD, Bushnell CD, Cucchiara B, Cushman M, Diagnosis and management of cerebral venous thrombosis: a statement for healthcare professionals from the American Heart Association/American Stroke AssociationStroke 2011 42(4):1158-92. [Google Scholar]
[6]. Treadwell SD, Thanvi B, Robinson TG, Stroke in pregnancy and the puerperiumPostgrad Med J 218 84(991):238-45. [Google Scholar]
[7]. Nazziola E, Elkind MS, Dural sinus thrombosis presenting three months postpartumAnn Emerg Med 213 42(4):592-95. [Google Scholar]
[8]. Canhao P, Ferro JM, Lindgren AG, Bousser MG, Stam J, Barinagarrementeria F, ISCVT Investigators. Causes and predictors of death in cerebral venous thrombosisStroke 215 36:1720-25. [Google Scholar]
[9]. Ashjazadeh N, Haghighi AB, Poursadeghfard M, Azin H, Cerebral venous-sinus thrombosis: a case series analysisIran J Med Sci 2011 36:178-82. [Google Scholar]
[10]. Thammishetti V, Dharanipragada S, Basu D, AnanthakrisHnan R, Surendiran D, A prospective study of the clinical profile, outcome and evaluation of D-dimer in Cerebral Venous ThrombosisJournal of Clinical and Diagnostic Research 2016 10(6):OC07-OC10. [Google Scholar]
[11]. Deguchi I, Dembo T, Kato Y, Yamane F, Ishihara S, Tanahashi N, A patient with deep cerebral venous sinus thrombosis in whom neuroendovascular therapy was effectiveJ Stroke Cerebrovasc Dis 2012 21:e5-e8. [Google Scholar]
[12]. Zis P, Tavernarakis A, Headache and status epilepticus in the postpartum period; posterior reversible encephalopathy syndrome or cerebral Venous Thrombosis?Case Reports in Emergency Medicine 2013 1-3:680327 [Google Scholar]
[13]. Gupta R, Aggarwal M, Patil S, Vyas V, Cerebral venous thrombosis associated with pregnancy: A case reportIOSR Journal of Dental and Medical Sciences 2015 14(5):43-45. [Google Scholar]
[14]. Ferro JM, Canhao P, Stam J, Bousser MG, Barinagarrementeria F, Prognosis of cerebral vein and dural sinus thrombosis: Results of the international study on cerebral vein and Dural Sinus Thrombosis (ISCVT)Stroke 214 35:664-70. [Google Scholar]
[15]. Narra R, Kamaraju SK, Pasupaleti B, Juluri N, Case of cerebral Venous Thrombosis with Unusual Venous InfarctsJournal of Clinical and Diagnostic Research 2015 9(4):TD08-TD10. [Google Scholar]
[16]. Sultana N, Chowdhury MH, Mahbub MS, Alam MB, Cerebral venous sinus thrombosis: A rare presentation of headache mimicking subarachnoid haemorrhageJ Medicine 219 10:115-18. [Google Scholar]
[17]. Einhaupla K, Stamb J, Bousserc MG, Bruijnd SFTM, Ferroe JM, Martinellif I, Guideline on the treatment of cerebral venous and sinus thrombosis in adult patientsEuropean Journal of Neurology 2010 17:1229-35. [Google Scholar]