Pulsatile Clavicular Swelling as the Sole Presentation of Asymptomatic Renal Cell Carcinoma with an Isolated Metastasis to the Clavicle: A Case Report
Ashwani Kumar1, Nitish Arora2, Paras Kumar Pandove3, Garima Anand4, Bharti Arora5
1 Professor, Department of General Surgery, Government Medical College and Rajindra Hospital, Patiala, Punjab, India.
2 Postgraduate Trainee, Department of General Surgery, Government Medical College and Rajindra Hospital, Patiala, Punjab, India.
3 Associate Professor, Department of General Surgery, Government Medical College and Rajindra Hospital, Patiala, Punjab, India.
4 Postgraduate Trainee, Department of Pathology, Government Medical College and Rajindra Hospital, Patiala, Punjab, India.
5 Postgraduate Trainee, Department of General Surgery, Government Medical College and Rajindra Hospital, Patiala, Punjab, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Nitish Arora, Doctor Hostel Rajindra Hospital Patiala -147001, Punjab, India.
E-mail: arora.nitish999@gmail.com
Renal Cell Carcinoma (RCC) is notorious for its unpredictable dissemination patterns involving both lymphatic and haematogenous route without a clear-cut preponderance for any. Unlike other intra-abdominal malignancies like colorectal carcinoma, renal cell carcinoma is often known to metastasize to distant sites even after a confident and unsuspecting curative resection or often as the primary presentation constantly adding and agitating our presentation patterns for this sneaky tumour. Presented below is a case of such an unsuspecting female patient. She was referred from the orthopaedic OPD to surgery OPD with a right clavicular swelling which was histopathologically examined and diagnosed as a metastatic renal cell carcinoma following which she was diagnosed with right renal cell carcinoma.
Bony swelling, Renal incidentaloma, Symptomatic metastasis
Case Report
A 50-year-old home maker was referred to the surgery outpatient clinic from the orthopaedic department. She complained of a painful swelling in the right shoulder for two months impairing overhead abduction. There was no history of trauma or immobilization. The left shoulder was normal with complete and painless overhead abduction. The swelling was initially a small one which had rapidly grown to the size of a tennis ball within two months span. It was pulsatile and tender to palpation without elevated surface temperature [Table/Fig-1].
Clinical picture of right clavicular swelling (arrow).

The general physical examination revealed pallor. Apart from the bony swelling no nodal swellings were found in the neck. Adjacent ipsilateral neck lymph nodes were not palpable. The abdomen was unremarkable on palpation. Blood urea and serum creatinine were normal. A skiagram for right shoulder showed a non visualized lateral one third of the clavicle on the right [Table/Fig-2].
Skiagram right shoulder joint showing non visualised lateral one third of clavicle(arrow)

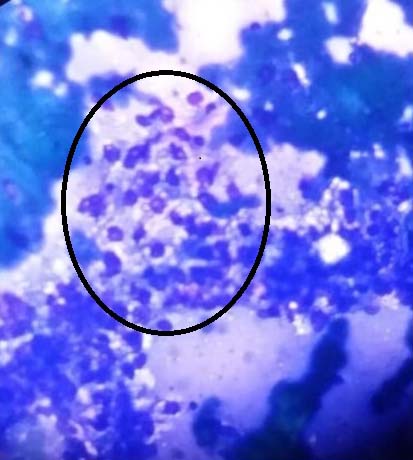
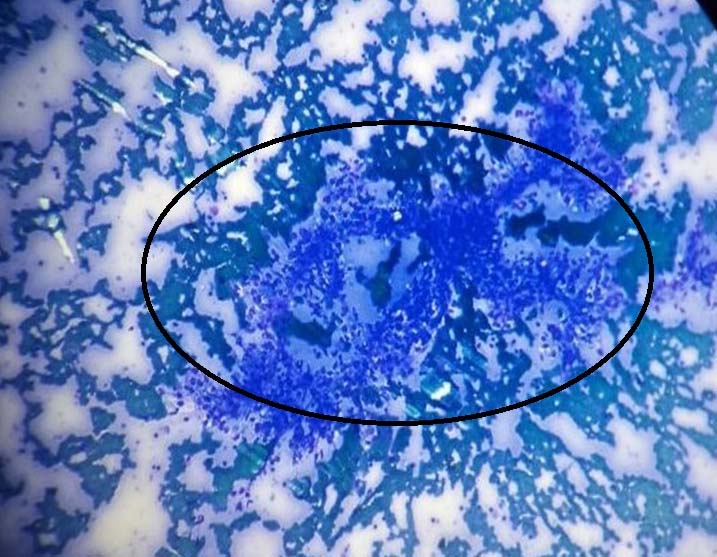
A Fine Needle Aspiration Cytology (FNAC) was taken from swelling. This showed epithelial cells forming clusters, papillaroid structures and papillae with focal fibrovascular core. The cells were medium sized with foamy vacuolated cytoplasm and single, small, hyperchromatic nuclei in some. Thus, the FNAC showed it to be a suspected metastatic deposit with a renal cell carcinoma as the provisional primary [Table/Fig-3,4].
Smear from FNAC under light microscope using 40X magnification and May- Grunwald- Giemsa stain.
Smear from FNAC under light microscope using 10X magnification and May- Grunwald- Giemsa stain.
The patient was re-evaluated for a family history of renal cell carcinoma. No such history was found. There was no history of flank pain, haematuria, abdominal pain, abdominal swelling, abdominal distention and any other bony swelling. Patient gave a history of back pain and loss of appetite in the past few months.
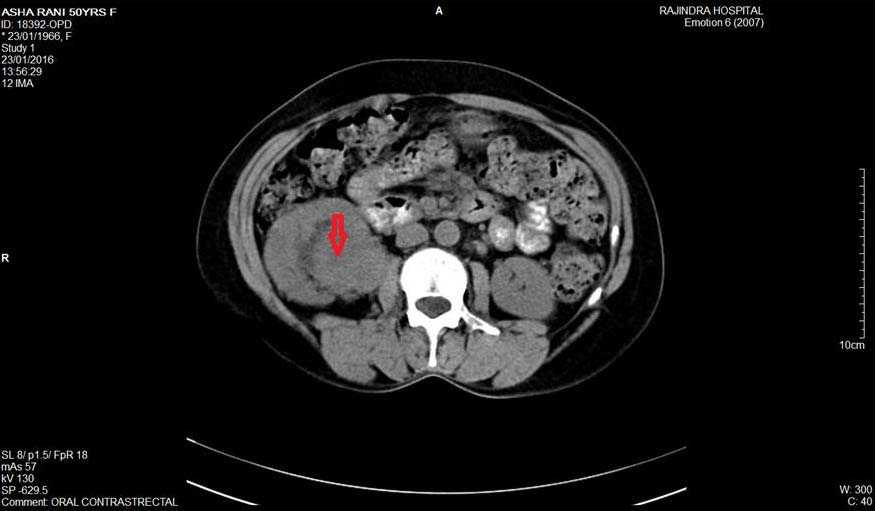
Contrast Enhanced Computerised Tomogram (CECT) abdomen revealed large lobulated peripherally enhancing heterogeneous mass arising from upper, middle pole and pelvis of right kidney. It measured 9 cmx 8 cmx 7.3 cm. It showed central non-enhancing area suggestive of necrosis. Neovascularisation was seen. A poorly enhancing soft tissue density mass was seen in the peri-pelvic suggestive of perinephric infiltration. Right renal vein, inferior vena cava and renal artery were normally opacified by contrast. Right adrenal was displaced by the above mass and not properly visualised. No ascites, no liver metastasis and no abdominal lymphadenopathy were seen [Table/Fig-5].
CECT Abdomen at the level of Right renal Hilum showing heterogeneous mass suggestive of Hypernephroma.
A skiagram chest was negative for metastases. Thus the final diagnosis was a 9cm maximum dimension right renal upper-mid polar carcinoma breaching the gerota’s fascia and perinephric tissue posteriorly with no evidence of direct tumour invasion to right adrenal, right renal vein with no abdominal, chest or cervical lymph nodes, with isolated right clavicular metastasis.
The treatment plan for the patient was External Beam Radiotherapy (EBRT) followed by nephrectomy. The patient is still under treatment and currently undergoing radiotherapy.
Discussion
It is increasingly being realised that the presentation of RCC in our country vary from the west in terms of age at onset, predisposition for metastasis and histological subtypes [1]. RCC commonly presents as incidentaloma on imaging for another cause or as symptomatic RCC with flank pain, flank mass or haematuria or a combination of these [2]. Thus, we can broadly classify RCC for epidemiological purposes into incidentally discovered RCC (I-RCC) and symptomatic RCC(S-RCC). Symptomatic RCC can be further classified as symptoms arising from the primary, vis-à-vis, flank pain, mass, haematuria or a combination of these. The other limb of symptomatic RCC includes those which are symptomatic due to distant metastasis. Common sites of distant metastasis are bone, lung, liver, brain and pelvic organ metastasis in females. The rarer manifestations of renal cell carcinoma reported include cutaneous metastasis [3,4], base of the tongue metastasis [5] and international literature reports metastatic deposits in the orbit, head and neck, thyroid, nasal and paranasal sinuses, parotid, heart, muscles and joints [6]. Solitary, extra axial bone metastasis is rare in RCC.
We faced dilemmas in prognostication and treatment due to lack of any guiding protocols for such a patient. Options available include metastasectomy with nephrectomy, Vascular Endothelial Growth Factor Receptor (VEGFR)– Platelet Drived Growth Factor Receptor (PDGFR) inhibitor based chemotherapy, Short Beam Radio-Therapy (SBRT) [7]. We had planned our patient on EBRT followed by right radical nephrectomy.
Clavicular metastasis in RCC is even rarer accounting less than 1 percent of the skeletal metastasis [8]. In an observational study by Kong Y et al., a total of 17 cases of clavicular metastasis were reported from 1998 to 2014 of which only four were due to RCC [8]. Reports of isolated clavicular metastasis in RCC are far and few in Indian literature and we report this case in order to add to the evidence regarding rare presentations of this tumour.
Other clavicle swellings with such a radiological presentation could be plasmacytomas, osteosarcomas, ewing sarcomas and granulocytic sarcoma with dense sclerosis. Among the benign lesions there are osteochrondromas, haemangiomas and a giant cell tumour secondary to paget disease [9]. In the present case, these differential diagnoses were ruled out by history, FNAC from the clavicular swelling and the corroborative CECT abdomen finding of right renal mass suggestive of hypernephroma. Thus a biopsy from the clavicular lesion with its attendant risks of bleeding and injury to vital structures at the root of the neck like brachial plexus, major vessels and pathological fracture was not deemed necessary by the treating physicians. In our review of literature we also found that the chances of the biopsy significantly altering the diagnosis of RCC were not significant [10].
Conclusion
Thus, the unassuming patient who came with a simple slightly painful clavicular swelling was finally diagnosed with stage IV RCC carcinoma after multiple referrals. The patient had none of the classical clinical findings that are commonly attributed to renal cancer. Crucial in aiding diagnosis was well read fine needle cytology from the swelling which told us about the histological origin of the mass. It helped us in staging the disease and planning treatment. This case reports adds to the various presentations of renal incidentalomas and the possibility of metastatic deposits as a differential for clavicular swelling.
[1]. Jemal A, Siegel R, Xu J, Ward E, Cancer Statistics, 2010CA: A Cancer Journal for Clinicians 2010 60:277-300. [Google Scholar]
[2]. Agnihotri S, Kumar J, Jain M, Kapoor R, Mandhani A, Renal cell carcinoma in India demonstrates early age of onset & a late stage of presentationIndian J Med Res 2014 140(5):624-29. [Google Scholar]
[3]. Rajasekharan P, Kavishwar V S, Butle P, Cutaneous metastasis from silent renal cell carcinomaJ Postgrad Med 2004 50:287-88. [Google Scholar]
[4]. Rajeev TP, Dorairajan LN, Hemal AK, Chest horn: An unusual metastasis from renal cell carcinomaIndian J Urol 2001 17:174-75. [Google Scholar]
[5]. Wadasadawala T, Kumar P, Agarwal J, Ghosh-Laskar S, Palliation of dysphagia with radiotherapy for exophytic base tongue metastases in a case of renal cell carcinomaIndian J Urol 2011 27:550-52. [Google Scholar]
[6]. Sountoulides P, Metaxa L, Cindolo L, Atypical presentations and rare metastatic sites of renal cell carcinoma: a review of case reportsJ Med Case Reports 2011 5:429 [Google Scholar]
[7]. Straka C, Nathan Kim DW, Timmerman RD, Pedrosa I, Jacobs C, Brugarolas J, Ablation of a site of progression with stereotactic body radiation therapy extends sunitinib treatment from 14 to 22 monthsJournal of Clinical Oncology 2013 31(23):e401-03. [Google Scholar]
[8]. Kong Y, Wang J, Li H, Guo P, Xu JF, Feng HL, Pathological clavicular fracture as first presentation of renal cell carcinoma: a case report and literature reviewCancer Biol Med 2015 12(4):409-12. [Google Scholar]
[9]. Smith J, Yuppa F, Watson RC, Primary tumors and tumor-like lesions of the clavicleSkeletal Radiol 1988 17:235 [Google Scholar]
[10]. Aly AM, Shaaban HM, Abou-Sinna I, Accuracy of fine needle aspiration cytology in the diagnosis of bone lesions with radiological assistance: Experience from the National Cancer Institute, Cairo University, EgyptThe Egyptian Journal of Radiology and Nuclear Medicine 2014 45(1):127-35. [Google Scholar]