Calcaneum is the most commonly fractured tarsal bone. A total of 70% calcaneal fractures are intra-articular and 30% are extra- articular [1-3]. The incidence of fracture calcaneum has remained relatively constant [3]. Axial loading is most common mode of injury, fall from height causing bilateral calcaneal fractures. Other fractures associated with fall from height have to be excluded such as pelvic and spinal fractures. Others like break pedal injuries and high-velocity trauma leading to open fractures are also common [1,2,4].
Talus is driven down into calcaneum by axial load which results in primary fracture line which runs across the posterior facet forming anteromedial and posterolateral fragments. Sustantacular fragment stays associated with the talus due to strong ligaments. Posterior fragment is important as it contains posterior facet. Essex Lopresti described secondary fracture lines, which can produce tongue type and joint depression type calcaneal fractures. Secondary fracture line extending through tuberosity of the calcaneum produces tongue type fracture and if it extends through dorsal aspect of calcaneum joint, depression type fracture results [3,5].
Conservative treatment of intra-articular fractures very often leads to increased morbidity due to incongruency of articular surface [1-4], widening of heel, talar dorsiflexion, loss of talo-calcaneal lever arm and peroneal tendon impingement [6-10]. Hence, focus has shifted to operative management with better outcome [3,6-9]. As far as operative treatment is concerned, best treatment option is controversial with several available options.
Previously, surgeons have used anterior cervical spine fusion plate, reconstruction plates, Sanders or modified Sander’s plate and 4mm simple cancellous screws for fixation after achieving acceptable reduction [3]. There were inconsistent results with conventional calcaneal plates. We evaluated the outcomes of open reduction and internal fixation of displaced intra-articular fractures of the calcaneum by locking calcaneal plate [Table/Fig-1].
Aim of the study was to evaluate the functional outcome after open reduction and internal fixation of displaced intra-articular fractures of the calcaneum by locking calcaneal plate.
Materials and Methods
This was a prospective interventional study conducted in the Department of Orthopaedic Surgery, Regional Institute of Medical Sciences (RIMS) and a tertiary care centre. Study was done in all patients having intra-articular fracture of calcaneum meeting inclusion and the exclusion criteria. Only those patients who had closed fracture, intra-articular fracture and where follow-up of 2 years is possible were included in the study. Open fractures, pathological fractures, fractures with spinal cord injury and head injury were excluded from the study.
Ethical approval was taken from Institution Ethical Committee. Informed consent was taken from all participants. X-rays were taken after initial vitals stabilization and complete clinical evaluation. Fracture pattern was assessed by using lateral, axial and Broden’s view of both feet for comparison. Fractures were classified by Essex Lopresti classification system based on X-rays. Gissane’s angle and Bohler’s angle were measured. CT scan was done to assess the extent of fracture comminution, geometry and the dimensions of the fracture (Only patients with comminuted fractures and patients in whom fracture geometry could not be assessed by plain x rays where subjected to CT scan). Preoperatively, Jone’s bandages were applied around the ankle and limb elevation was ensured. After admission to ward, all routine investigations were done and patients were operated as early as possible, once the patient became fit for surgery and skin condition was good. Patient with gross edema surgery was postponed for 10 to 14 days and till then limb was kept elevated till the wrinkle sign became positive.
The surgery was carried out in general/spinal anaesthesia. A systemic antibiotic was administered just before induction of patients by anaesthetists. After placing the patient on lateral position with affected side up on a radiolucent table, a thigh tourniquet was applied and whole foot and ankle painted up to leg and draped. Right-angled skin incision was planned [Table/Fig-2]. Tip of lateral malleolus, base of fifth metatarsal and tendo achillis tendon were the three landmarks, which were marked on the skin. Incision was started midway between tendoachillis tendon and tip of lateral malleolus which was extended downwards vertically till the junction of skin and sole of the foot where it was turned towards the fifth metatarsal base. Angle was curved and not sharp. Retraction of skin was done subperiosteally thereby, flap of tissue was elevated to avoid skin necrosis. Care was taken to avoid injury to peroneal sheath containing peroneal tendons without opening it. Retraction was maintained by k-wires fixed to lateral malleolus, neck of talus and cuboid distal to calcaneocuboid joint which were bent away from operating field. Fixation was aimed at restoring the length, axial alignment (varus and valgus angulations) and alignment of articular surface of subtalar joint. Interfragmentary screw was used to fix the sustentaculum tali to the lateral wall. Schanz pin was used as a joy sticks to achieve reduction by inserting into posterolateral tuberosity of calcaneum. Plate was bent according to the contour of lateral wall of the calcaneum and excessive holes were cut. Locking calcaneal plate was temporarily fixed with K wires to the lateral wall after adjusting the holes. Predrilling was done with suitable drill bit. Care was taken to avoid damage to medial neurovascular structures. After checking with depth, gauze plate was fixed with screws [Table/Fig-3]. Articular reduction, plate placement and screw length were confirmed under C-arm. Skin closure done with or without number 10 drain after removing the k wires [Table/Fig-4]. Compressive bandage was applied.
Incision and retraction with k wires.


Closure with number 10 drain.

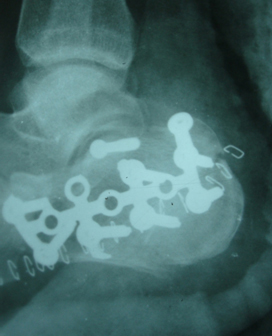
Post-operatively foot was elevated for 48 hours. Active ankle, subtalar and knee exercises were started after 48 hours. Post-operatively antibiotics were stopped after 48 hours. Drain was removed after two days. Post-operative dressing was done on fifth day. Sutures were removed after 2 weeks and discharged with advice of strict non weight bearing for two months. Follow-up was done at 3,6,12 and 24 months. Serial x rays were taken [Table/Fig-5,6]. Gissane’s angle and Bohler’s angle were calculated. The final outcome based on the above observations was done as per American Orthopaedic Foot and Ankle Society Score (AOFAS), Ankle–Hindfoot Scale, The clinical results were graded as 90 excellent, 80 good, 70 fair and ≤70 as poor [11,12].
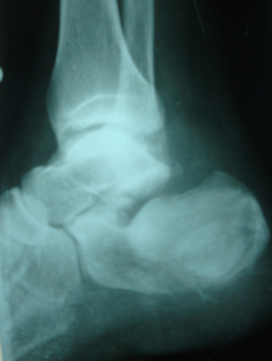
Post-operative x-ray restoring Bohler’s angle.
Results
A total of 30 calcaneal fractures in 24 patients were randomly selected treated by locking calcaneal plate. Among the 24, 6 patients had bilateral fracture calcaneum. No patients were lost to follow-up.
In the present study, average age was 37.5 years ranging from 17 to 59 years. Twenty patients were male and four patients were female. Twenty fractures were on right side and 10 fractures on left side. In 21 (87.5%) patients, mechanism of injury was fall from height and 3 patients (12.5%) had road traffic accidents. Fractures were classified according to Essex Lopresti classification in which 19 (63.3%) feet had joint depression fracture and 11 (36.6%) had tongue type fracture configuration. All the patients were operated within two weeks from date of injury. Average operating time was 88 minutes. Mean time of union was 12.5 weeks. Preoperatively, average Bohler’s angle was 8.1° (range,−8° to 19°) improved to 30.9° (range, 25° to 41°) Post-operatively. At final, follow-up assessment of AOFAS score was calculated, the mean AOFAS score was 79.9 (Range 49-96). In the present study, 13 (43.3%) patients had excellent results, 10 (33.3%) patients had good, three (10%) patients had fair and four (13.3%) patients had poor results. Heel widening was the most common complication noted in our study group [Table/Fig-7]. Patient with wound dehiscence healed in 3 weeks without any complications.
The incidences of complications among the study population.
| Complication | Percentage |
|---|
| Heel widening | 93.3% |
| Ankle swelling | 50% |
| Heel pain | 33.3% |
| Early subtalar arthritis | 10% |
| Wound dehiscence | 0.3% |
| Sural nerve injury | 0.3% |
Discussion
Open reduction and internal fixation of displaced intra-articular calcaneal fractures by locking calcaneal plate maintains the joint congruity and decrease the incidence of subtalar arthritis. Although, conservative treatment was considered gold standard previously, there is increase tendency towards internal fixation with excellent results. Extended ‘L’ lateral approach had given a good exposure in our cases. In our study, average age was 37.5 years ranging from 17 to 59 years. Jain S et al., in their study assessing 30 cases ranged from 24-49 years with a mean age of 31.6 years [13]. In our study 20 fractures (66.6%) were on right side and ten fractures (33.3%) on left side [Table/Fig-8] [14-16].
A comparative evaluation of studies based on the laterality of the fracture side.
| Present study | Almeida V et al., [14] | Buckley R [15] | Crosby LA et al., [16] |
|---|
| Right | 66.6% | 54.5% | 51% | 40% |
| Left | 33.3% | 45.5% | 49% | 60% |
| Bilateral | 25% | 47% | 47% | 10% |
In our study, most common mode of injury was fall from height which constituted 21 patients (87.5%) and rest were due to road traffic accidents. Zeman P et al., in their study, the most frequent cause of injury was a fall or jump from height; this was recorded in 27 patients (93.1%) [17]. Jain S et al., in their study assessing 30 cases most common mode of injury was fall from height in 21 patients, while road traffic accident was in 3 patients [13]. Pendse A et al., in their study, noted the mechanism of injury was fall from height in 26 patients and road traffic accidents in 3 patients out of 19 patients [3]. In our study, 19 (63.3%) patients had joint depression fracture and eleven (36.6%) had tongue type fracture configuration. Pendse A et al., in their study, 21(70%) fracture had joint depression variety and 9(30%) fractures had tongue type fracture [3]. Study conducted by Mostafa MF et al., comprising 18 cases noted 12 cases were of joint depression type and six cases were of tongue type fractures [5]. Timing of operation was a very crucial decision to make in the operations of calcaneal fractures as soft tissue break down was devastating complication. All of our patients were operated on within mean 8.9 days (ranging from 6-21 days). Jain S et al., in their study patients were operated within mean 9.2 days [13]. Zeman P et al., in their study, surgical procedure was performed on average within 11.7 days of injury [17].
At final, follow-up assessment of AOFAS score was calculated, the mean AOFAS score was 79.9 (Range 49-96). Excellent results were achieved in 13 (43.3%) cases, good results in 10 (33.3%), fair result in three (10%) cases and poor result in four cases (13.3%). These results were comparable to other study conducted by other authors [Table/Fig-9] [12-14]. Mean AOFAS score was 86.3 in study by Jain S et al., 77.89 in study by Almeida V et al., 70 in study by Ibrahim T et al., and 66 in study by Howard et al., [13,14,18,19].
A comparative evaluation of studies based on the final outcome.
| Present study | Almeida V et al., [14] | Jain S et al., [13] | Weber M et al., [12] |
|---|
| Excellent | 13 | 43.3% | 31.8% | | 38% |
| Good | 10 | 33.3% | 11.4% | 86% | 46% |
| Fair | 3 | 10% | 29.5% | 7.7% | 12% |
| Poor | 4 | 13.3% | 27.3% | 3.7% | 4% |
Bohler’s angle is crucial and predicts the outcome of fractures. Loss of Bohler’s angle (normal 25 to 40) was associated with poor outcome and restoration following surgery resulted in excellent outcome. In our study, Bohler’s angle measured preoperatively decreased to average of 12 degrees Post-operatively we were able to increase to an average of 32 degrees. Bohler’s angle was restored in 25(83.3%) feet after 24 months of follow-up, which was comparable to study conducted by Haddad M et al., who noted restoration of Bohler’s angle [20] 74% of calcaneum and 86.6% of calcaneum in study conducted by Jain S et al., [13].
Heel widening was the most common complication in our study followed by ankle swelling. One patient had wound dehiscence. Jain S et al., noted flap necrosis in 3 patients [13] and Weber et al., noted wound dehiscence in one patient [12].
Limitation
The limitation of the study is its small number of patients and the short term follow-up. Multicentric randomised control studies with long term follow-up of patients is required to prove the superiority of calcaneal locking compression plates over conventional calcaneal plates.
Conclusion
Based on our research findings and results, we conclude that open reduction and internal fixation with locking calcaneal plate is excellent treatment option with good functional outcome for intra- articular displaced fracture of calcaneum. Local skin condition, timing of surgery and soft tissue dissection are most important in determining the success of surgery and rate of infections. As serious complication rates are relatively low and most of the complications are minor, locking calcaneal plate should be considered first choice of implant in displaced intra-articular fractures of calcaneum.