Ability of Oral and Maxillofacial Surgery Residents in Diagnosing Jaw Cysts: A Retrospective 20 Years Study
Hassan Mohajerani1, Mohammad Esmaeelinejad2, Reza Mofidian3
1 Associate Professor, Department Oral and Maxillofacial Surgery, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2 Resident, Department Oral and Maxillofacial Surgery, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
3 Resident, Department Oral and Maxillofacial Surgery, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Reza Mofidian, Department of Oral and Maxillofacial Surgery, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
E-mail: reza_mofidian@yahoo.com
Introduction
Diagnosis of odontogenic cysts despite of their benign nature is a critical and challenging problem especially among undergraduate and postgraduate students.
Aim
This study aimed to evaluate the capability of oral and maxillofacial surgery residents in diagnosing odontogenic cysts.
Materials and Methods
This cross-sectional study was executed on 312 patient records over the past 20 years since October 1995 till December 2014 in Taleghani Hospital, Tehran, Iran. All recorded data was based on 2005 World Health Organization (WHO) classifications. The differential diagnosis was made by 65 residents based on clinical and paraclinical evaluations established in the charts. Differential diagnoses made by the residents were compared to the histopathological examination as the gold standard for identifying the nature of the cysts. Weighted kappa test was used to show the degree of agreement.
Results
Data extracted from 312 records were analyzed. The mean age of examined patients was 27.6 years. The accuracy of diagnosis among the residents was moderate (kw=0.5). The diagnosis made by the residents was significantly related to the radiographic view of the cysts (p<0.05). The residents were able to identify odontogenic keratocysts and dentigerous cysts in most cases.
Conclusion
There are several factors associated with the occurrence of pathologic odontogenic cysts which could help either the clinician or the pathologist in diagnosing the odontogenic cysts of the jaws. The surgeons should consider these related factors before the final diagnosis and choosing the appropriate treatment plan.
Odontogenic keratocyst, Pathology, Surgeons
Introduction
Odontogenic cysts are slow growing lesions of maxillofacial region. The occurrence rate of these cysts is approximately 20% of all the pathologic lesions of jaws and 90% of all oral and maxillofacial cysts [1]. Odontogenic cysts are divided into two main groups of inflammatory and developmental cysts [2]. The prevalence of the various cysts is different in different populations. They could occur in different parts of jaw and their distribution is different in various populations [3,4].
Despite their benign nature and slow growing behaviour they could expand in the jaws and reach to a considerable size that invades the adjacent anatomical structures like neurovascular bundles. On the other hand there is a chance that malignancy tumors like Squamous Cell Carcinoma (SCC) may originate from the epithelium of these benign lesions [5,6], so early diagnosis and treatment of the odontogenic cysts are important issues in the field of oral medicine and maxillofacial surgery.
Training of surgery residents and medical students to diagnose the diseases and pathologic conditions is a comprehensive program which is different in various hospitals and universities [7,8]. It is expected that the maxillofacial surgery residents be able to present the most proper diagnosis for a pathologic cyst in jaws. However, the exact diagnosis of oral and maxillofacial cysts is difficult due to the similarity between some cysts. Several factors have been indicated to contribute in occurrence of the cysts which are similar in some of them [9].
Treatment of the cysts is affected by several factors and could be different. Furthermore in some cases the pathologist is not able to differentiate between some cysts because of their similar histopathologic features [10,11]. In these cases the ability of the surgeon to identify the exact diagnosis of the cyst according to the clinical and radiographic features of the lesion is very important. The surgeon could treat the pathologic lesions very well and choose the appropriate treatment plan by being aware of the whole contributing factors in occurrence of odontogenic cysts and diagnose the lesion correctly.
In the current study, following previous study on jaw cysts conducted by the authors [9], we aimed to evaluate the ability of oral and maxillofacial surgery residents in diagnosing the odontogenic and non-odontogenic cysts and presenting the important factors contributing in helping the clinicians to achieve the best diagnosis. The authors declare that this is the extension of the previous study.
Materials and Methods
The current retrospective study was carried out on 312 records of the patients who were referred to the Department of Oral and Maxillofacial Surgery of the Taleghani Hospital, Tehran, Iran, between 1995 and 2014. The necessary data was extracted from the records including clinical examination charts, histopathology records, and imaging records. The data was collected in a categorized chart.
The inclusion criteria for selecting the patients were: the patients who were hospitalized between October 1995 and December 2014, the patients who were referred for the first time, the patients whose records were complete and with no missing variable, the pathology report of the patient confirmed jaw cysts, the available panoramic view of the cyst.
The patients were categorized in four age groups:
- Group A: Children (≤10 years old)
- Group B: Young patients (>10 and ≤30 years old)
- Group C: Middle aged patients (>30 and ≤50 years old)
- Group D: Elderly patients (more than 50 years old)
All the differential diagnoses were recorded by the chief residents of that time (the fifth year residents). A total of 65 residents contributed in this study.
WHO classification of odontogenic cysts and tumors (2005) was used in current study [12]. Odontogenic Keratocyst (OKC) was categorized as a cystic lesion in the present study; however, it was defined as a benign tumor and classified as a keratocystic odontogenic tumor.
Ethical Considerations: The current study was designed according to the hospital’s ethics committee rules. The name and personal identifications of the patients were omitted from the study.
Statistical Analysis
All calculations were processed using Statistical Package for Social Science statistical software (version 20; SPSS Inc.). Descriptive statistics including tables and graphs were applied to show the information. Weighted kappa test was used to evaluate the degree of agreement between the diagnoses of the lesions recorded by the residents and the pathological reports.
Results
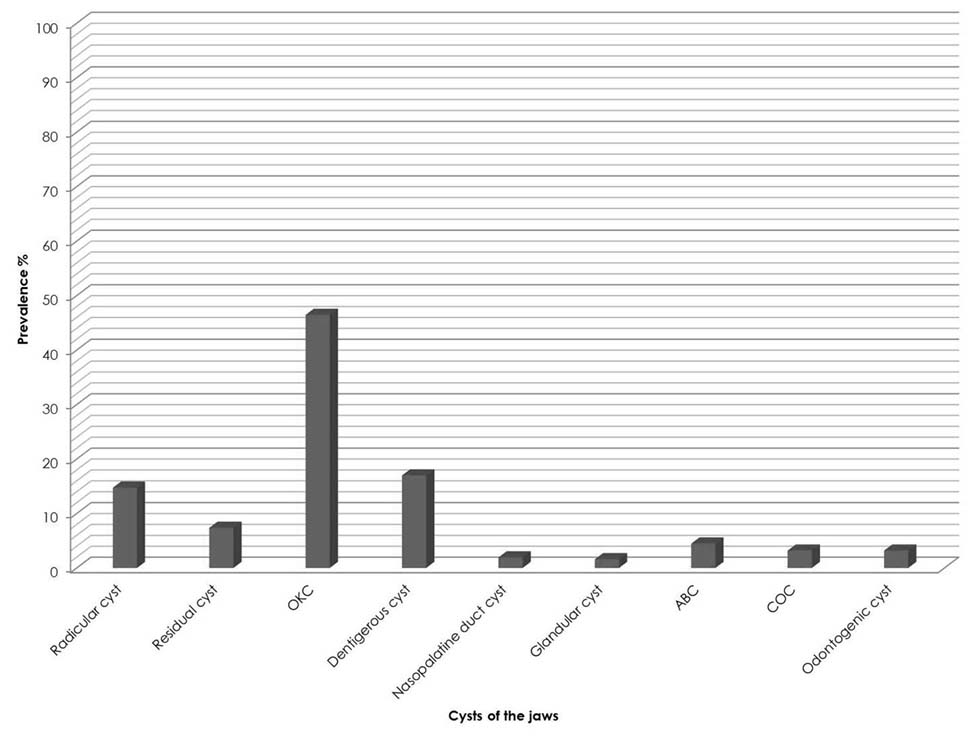
A total of 312 patents (185 men and 127 women) between the ages of 9 to 77 (mean age of 27.6±13.47) were included in the present study. Three hundred cases of total 3466 pathologic lesions of head and neck area (9%) were odontogenic cysts [9]. Glandular cyst was the least common lesion of all [Table/Fig-1]. The age distribution is shown in [Table/Fig-2].
Prevalence of different jaw cysts in Iranian population.
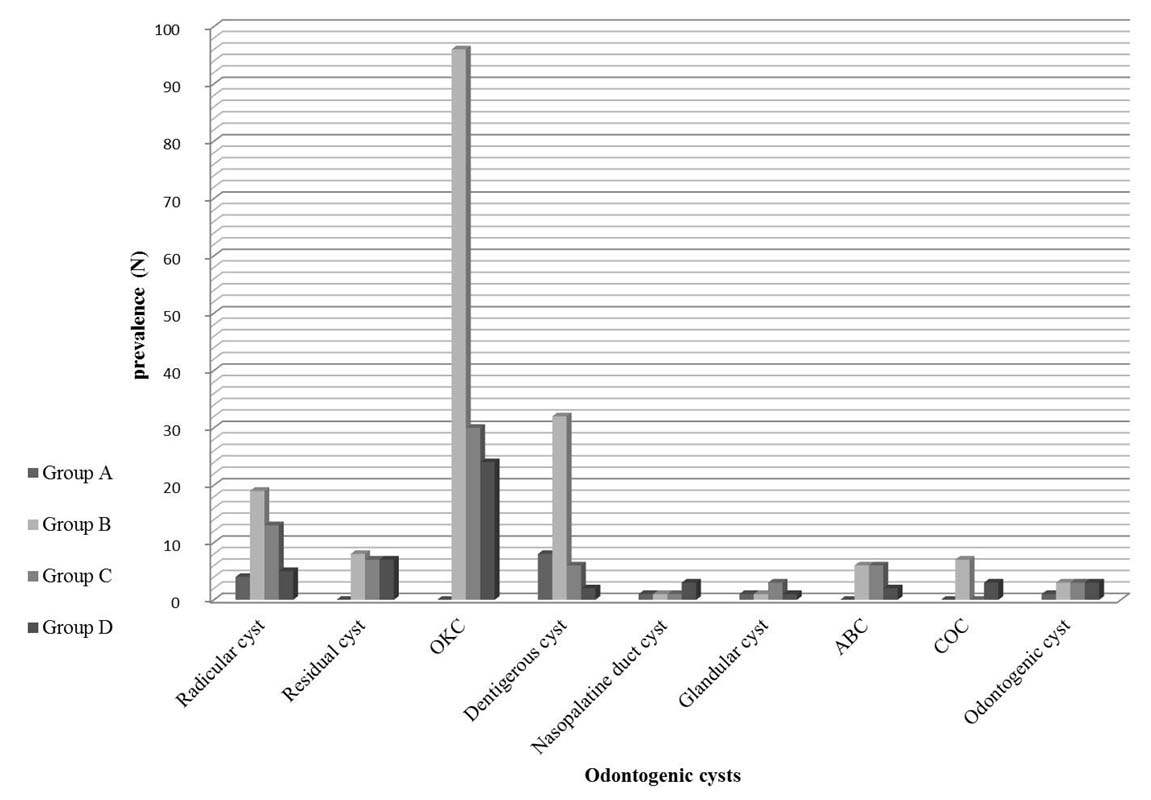
Distribution of various jaw cysts in different age groups.
Group A, children (≤10 years old); Group B, young patients (>10 and ≤30 years old); Group C, middle aged patients (>30 and ≤50 years old); Group D, elderlies (more than 50 years old).
The degree of agreement between the initial diagnosis made by the residents and the final pathologic reports was calculated with weighted kappa (kw), kw was calculated to be 0.5 which showed moderate agreement between the initial differential diagnosis and the final diagnosis of the lesions [Table/Fig-3]. The most common agreement was between the initial diagnosis of OKC and its pathologic report [Table/Fig-4]. There was a significant relationship between the radiographic view of the cyst and the differential diagnosis [Table/Fig-5].
The agreement between the initial diagnosis made by the residents and the pathologic report.
| | Pathologic Report | Total |
|---|
| RadicularCyst | ResidualCyst | OKC | DentigerousCyst | Nasopal-atine Duct Cyst | Glandular Cyst | Odont-ogenicCyst | ABC | COC |
|---|
| InitialDiagnosis | Radicular Cyst | 41 | 0 | 1 | 0 | 1 | 2 | 0 | 0 | 0 | 45 |
| Residual Cyst | 0 | 15 | 10 | 0 | 0 | 2 | 5 | 0 | 3 | 35 |
| OKC | 0 | 5 | 102 | 0 | 0 | 0 | 0 | 0 | 0 | 107 |
| Dentigerous Cyst | 5 | 0 | 10 | 49 | 0 | 0 | 0 | 0 | 0 | 64 |
| Unicyctic Ameloblastoma | 0 | 3 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 4 |
| Nasopalatine Duct Cyst | 0 | 0 | 0 | 0 | 5 | 0 | 0 | 0 | 0 | 5 |
| Glandular Cyst | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 3 | 4 |
| Odontogenic Cyst | 0 | 0 | 22 | 3 | 0 | 0 | 0 | 10 | 0 | 35 |
| ABC | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 4 | 0 | 4 |
| COC | 0 | 0 | 0 | 0 | 0 | 0 | 5 | 0 | 4 | 9 |
| Total | 46 | 23 | 145 | 53 | 6 | 5 | 10 | 14 | 10 | 312 |
OKC: odontogenickeratocyst; ABC: aneurysmal bone cyst; COC: calcifying odontogenic cyst
Degree of agreement between the initial differential diagnosis and histopathological reports.
| | Differential Diagnosis | Total |
|---|
| Radicular Cyst | Residual Cyst | OKC | Dentigerous Cyst | Nasopalatine Duct Cyst | Odontogenic Cyst | ABC | No Diagnosis |
|---|
| Pathologic Report | Radicular Cyst | 41 | 0 | 0 | 5 | 0 | 0 | 0 | 0 | 46 |
| Residual Cyst | 0 | 20 | 0 | 0 | 0 | 0 | 0 | 3 | 23 |
| OKC | 4 | 10 | 93 | 10 | 0 | 25 | 0 | 3 | 145 |
| Dentigerous Cyst | 0 | 0 | 0 | 41 | 0 | 10 | 0 | 2 | 53 |
| Nasopalatine Duct Cyst | 0 | 0 | 0 | 0 | 6 | 0 | 0 | 0 | 6 |
| Glandular Cyst | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 3 | 5 |
| Odontogenic Cyst | 0 | 5 | 0 | 0 | 0 | 2 | 0 | 3 | 10 |
| ABC | 0 | 0 | 0 | 0 | 0 | 6 | 4 | 4 | 14 |
| COC | 0 | 0 | 0 | 0 | 0 | 3 | 0 | 7 | 10 |
| Total | 45 | 35 | 93 | 56 | 6 | 48 | 4 | 25 | 312 |
OKC: odontogenickeratocyst; ABC: aneurysmal bone cyst; COC: calcifying odontogenic cyst
The correlation between initial diagnosis made by residents and the radiographic views.
| | Differential Diagnosis | Total |
|---|
| Radicular Cyst | Residual Cyst | OKC | Dentigerous Cyst | Nasopalatine Duct Cyst | Odontogenic Cyst | ABC | No Diagnosis |
|---|
| Radiographic Representation | Unilocular well-defined | 37 | 33 | 64 | 47 | 5 | 29 | 2 | 12 | 229 |
| Unilocular ill-defined | 5 | 0 | 4 | 0 | 1 | 4 | 0 | 3 | 17 |
| Multilocular well-defined | 3 | 2 | 25 | 9 | 0 | 15 | 2 | 10 | 66 |
| Total | 45 | 35 | 93 | 56 | 6 | 48 | 4 | 25 | 312 |
OKC:odontogenic keratocyst; ABC; aneurysmal bone cyst; COC: calcifying odontogenic cyst
Discussion
Clinicopathological features of odontogenic cysts have been evaluated and presented in various populations [13,14]. Despite their slow growing and benign nature early diagnosis and treatment of these lesions are valuable for rehabilitation of the patient and preventing from some serious complications. Their tendency to recurrence and changing into malignancies are two important factors promoting the clinicians to treat the jaw cysts as soon as possible [15–17]. There are several factors helping the clinicians in diagnosing the oral lesions especially the odontgenic cysts including the clinical and radiographic views of the cysts [18]. So we tried to evaluate the ability of maxillofacial surgery chief residents in diagnosing the odontogenic cysts according to the contributing factors in occurrence of the lesions.
In current study 312 patients with the chief complaint of presence of a pathologic lesion in jaw were included. The final diagnosis of all these lesions was confirmed as an odontogenic cyst by histopathological assessment. OKC and dentigerous cysts were the most common lesions of all. The radicular cyst was the most common odontogenic cyst of all in almost all investigations despite the current survey. The reason of this finding was the referral structure of Taleghani Hospital. As a matter of fact the outgoing patients were referred to the dental faculties in Iran and the patients who should undergo major surgeries were admitted in the hospital. In other investigations dentigerous cysts and OKC were the most common developmental odontogenic cysts of all [19,20].
The ability of the surgery residents was evaluated according to the statistical analysis. The residents were able to detect the OKC very well in the patients following radicular and dentigerous cysts. They were confused and not able to distinguish between OKC and dentigerous cysts in several cases. This problem could be due to similar clinical and radiographical features of these two lesions [21,22]. These findings emphasize on critical and comprehensive work-up which is required for confusing cases and performing biopsy to be sure of the definite diagnosis before forcing the patient to undergo an extensive procedure.
The pathologist was not able to detect the nature of the cyst in 3.2% of the cases exactly. This finding may be due to the common origin of the odontogenic cysts and similar histopathological features of some cases [23]. According to this finding the importance of the ability of surgeons in diagnosing the jaw cysts based on the clinical feature becomes more obvious. On the other hand it is suggested to take several specimens during the incisional biopsy for helping and making it much easier for the pathologist to make the definite diagnosis.
Azevedo RS et al., described the clinicopathological features of OKC in Brazilian population. They showed that there could be several variations of OKC which may make the diagnosis of this lesion challenging in some cases. They suggested that a full analysis of this lesion is necessary to achieve the correct diagnosis [24].
There were two main reasons why we included OKC as an odontogenic cyst in the present study. First of all this study was designed to evaluate the extracted over past 20 years and OKC was categorized as a tumor only 9 years back. On the other hand the behaviour and growing pattern of OKC is still under evaluation and in some investigations the authors still mention a cystic pattern for this lesion.
There are several factors associated with the occurrence of odontogenic cysts which could help the clinicians to reach to the possible diagnosis [4,9,25]. Pattern of radiographic view, aspiration, location of the cyst, presence of an impacted tooth, age of the patient, and gender were the contributing factors included in this investigation. Among all the correlated factors the radiographical views of the lesions were more helpful for the residents to achieve to the best differential diagnosis.
Limitation
Current study was performed in one of the most popular maxillofacial surgery centers of Iran; however, there are several important maxillofacial surgery centers in this country. This was one of the limitations of present investigation. It is suggested similar studies be designed in other centers and the relation of their findings with the different residency education programs be presented.
Conclusion
In conclusion the ability of surgery residents in diagnosing the cysts of the jaws was moderate. This finding indicates that there is a need to improve hospital educational systems in training the residents to learn the most important and common features of the diseases which could help them in diagnosing the disease accurately.
OKC: odontogenickeratocyst; ABC: aneurysmal bone cyst; COC: calcifying odontogenic cyst
OKC: odontogenickeratocyst; ABC: aneurysmal bone cyst; COC: calcifying odontogenic cyst
OKC:odontogenic keratocyst; ABC; aneurysmal bone cyst; COC: calcifying odontogenic cyst
[1]. Del Corso G, Righi A, Bombardi M, Rossi B, Dallera V, Pelliccioni GA, Jaw cysts diagnosed in an Italian population over a 20-year periodInt J Surg Pathol 2014 22(8):699-706. [Google Scholar]
[2]. Nunez-Urrutia S, Figueiredo R, Gay-Escoda C, Retrospective clinicopathological study of 418 odontogenic cystsMed Oral Patol Oral Cir Bucal 2010 15(5):e767-73. [Google Scholar]
[3]. Demirkol M, Ege B, Yanik S, Aras MH, Ay S, Clinicopathological study of jaw cysts in southeast region of TurkeyEur J Dent 2014 8(1):107-11. [Google Scholar]
[4]. Lin HP, Wang YP, Chen HM, Cheng SJ, Sun A, Chiang CP, A clinicopathological study of 338 dentigerous cystsJ Oral Pathol Med 2013 42(6):462-67. [Google Scholar]
[5]. Cavalcanti MG, Veltrini VC, Ruprecht A, Vincent SD, Robinson RA, Squamous-cell carcinoma arising from an odontogenic cyst-the importance of computed tomography in the diagnosis of malignancyOral Surg Oral Med Oral Pathol Oral Radiol Endod 2005 100(3):365-68. [Google Scholar]
[6]. Falaki F, Delavarian Z, Salehinejad J, Saghafi S, Squamous cell carcinoma arising from an odontogenic keratocyst: A case reportMed Oral Patol Oral Cir Bucal 2009 14(4):E171-74. [Google Scholar]
[7]. Cerero-Lapiedra R, Esparza-Gomez GC, Casado-de la Cruz L, Dominguez-Gordillo AA, Corral-Linaza C, Seoane-Romero JM, Ability of dental students in Spain to identify potentially malignant disorders and oral cancerJ Dent Educ 2015 79(8):959-64. [Google Scholar]
[8]. Ali MA, Joseph BK, Sundaram DB, Dental students’ ability to detect and diagnose oral mucosal lesionsJ Dent Educ 2015 79(2):140-45. [Google Scholar]
[9]. Mohajerani H, Esmaeelinejad M, Sabour S, Aghdashi F, Dehghani N, Diagnostic factors of odontogenic cysts in Iranian population: A retrospective study over the past two decadesIran Red Crescent Med J 2015 17(6):e21793 [Google Scholar]
[10]. Fellegara G, Mody K, Kuhn E, Rosai J, Normal dental papilla simulating odonto-genic myxomaInternational Journal of Surgical Pathology 2007 15(3):282-85. [Google Scholar]
[11]. Suarez PA, Batsakis JG, El-Naggar AK, Don’t confuse dental soft tissues with odontogenic tumorsAnn Otol Rhinol Laryngol 1996 105(6):490-94. [Google Scholar]
[12]. Reichart PA, Philipsen HP, Sciubba JJ, The new classification of head and neck tumours (WHO)—any changes?Oral Oncology 2006 42(8):757-58. [Google Scholar]
[13]. Tekkesin MS, Olgac V, Aksakalli N, Alatli C, Odontogenic and nonodontogenic cysts in Istanbul: Analysis of 5088 casesHead Neck 2012 34(6):852-55. [Google Scholar]
[14]. Bataineh AB, Rawashdeh MA, Al Qudah MA, The prevalence of inflammatory and developmental odontogenic cysts in a Jordanian population: A clinicopathologic studyQuintessence Int 2004 35(10):815-19. [Google Scholar]
[15]. Scheer M, Koch AM, Drebber U, Kubler AC, Primary intraosseous carcinoma of the jaws arising from an odontogenic cyst-A case reportJ Craniomaxillofac Surg 2004 32(3):166-69. [Google Scholar]
[16]. Matise JL, Beto LM, Fantasia JE, Fielding AF, Pathologic fracture of the mandible associated with simultaneous occurrence of an odontogenic keratocyst and traumatic bone cystJ Oral Maxillofac Surg 1987 45(1):69-71. [Google Scholar]
[17]. Murakami K, Yamamoto K, Tsuyuki M, Sugiura T, Tsutsumi S, Kirita T, Theoretical efficacy of preventive measures for pathologic fracture after surgical removal of mandibular lesions based on a three-dimensional finite element analysisJ Oral Maxillofac Surg 2014 72(4):833.e1-18. [Google Scholar]
[18]. Tatli U, Erdogan O, Uguz A, Ustun Y, Sertdemir Y, Damlar I, Diagnostic concordance characteristics of oral cavity lesionsScientific World Journal 2013 2013:785929 [Google Scholar]
[19]. Jones AV, Craig GT, Franklin CD, Range and demographics of odontogenic cysts diagnosed in a UK population over a 30-year periodJ Oral Pathol Med 2006 35(8):500-07. [Google Scholar]
[20]. Tortorici S, Amodio E, Massenti MF, Buzzanca ML, Burruano F, Vitale F, Prevalence and distribution of odontogenic cysts in Sicily: 1986-2005J Oral Sci 2008 50(1):15-18. [Google Scholar]
[21]. Chaudhary S, Sinha A, Barua P, Mallikarjuna R, Keratocystic odontogenic tumour (KCOT) misdiagnosed as a dentigerous cystBMJ Case Reports 2013 doi:10.1136/bcr-2013-008741 [Google Scholar]
[22]. Meleti M, van der Waal I, Clinicopathological evaluation of 164 dental follicles and dentigerous cysts with emphasis on the presence of odontogenic epithelium in the connective tissue. The hypothesis of "focal ameloblastoma"Med Oral Patol Oral Cir Bucal 2013 18(1):e60-64. [Google Scholar]
[23]. Gardner DG, O’Neill PA, Inability to distinguish ameloblastomas from odontogenic cysts based on expression of blood cell carbohydratesOral Surg Oral Med Oral Pathol 1988 66(4):480-82. [Google Scholar]
[24]. Azevedo RS, Cabral MG, Santos TCRBd, de Oliveira AV, de Almeida OP, Pires FR, Histopathological features of keratocystic odontogenic tumor: A descriptive study of 177 cases from a Brazilian populationInternational Journal of Surgical Pathology 2012 20(2):152-58. [Google Scholar]
[25]. MacDonald D, Gu Y, Zhang L, Poh C, Can clinical and radiological features predict recurrence in solitary keratocystic odontogenic tumors?Oral Surg Oral Med Oral Pathol Oral Radiol 2013 115(2):263-71. [Google Scholar]