Identification of human remains is one of the prime factors addressing the victims in case of mass disasters such as fire accidents, explosions, aircraft and railway accidents. Anthropometry which is a branch of physical anthropology is a series of systematic quantitative measurements of human body and skeletal dimensions [1]. Traditio-nally, this method is employed to determine the identification of an individual from the skeletal remains [2]. Personal identification in true sense is determining and establishing the identity of an individual. This aspect of identification has assumed importance in almost all aspects of life where the need is obvious for social and medico legal purposes [3].
In majority of natural and manmade disasters, identification of re-mains in official investigations has received innumerable contributions from forensic/legal dentistry [4]. The four essential factors usually represented as ‘big fours’ in determining personal identification are age, sex, stature and ethnicity [3]. Stature is the height of a person in the upright posture. Every body part possesses more or less constant relationship with stature [5] and it is also an essential factor in personal identification which aids in cut shortening the investigation process [6]. The definite dimensional relationship with each and every part of the human body has been the focus of research among many anthropologists and investigators [7].
In this regard, an aspect of human/personal identification that has received scant attention from investigators, when only skull is available, is the estimation of stature using tooth dimensions [8]. No two individuals have identical tooth features and furthermore, teeth are resistant to peri- and post-mortem alterations [9], this aspect who helps in identification of individuals.
Although the relationship between crown size and body size has been questioned previously, few studies have reported positive but low-order correlations between crown size and various body dimensions [10]. A study conducted by Kalia S et al., among Mysorean population of India had shown a low but statistically significant correlation between tooth dimensions and stature [11].
The seeds for stature estimation through tooth dimensions were sown by an Argentinean professor, Juan Ubaldo Carrea in 1920. He developed a mathematical calculation to estimate the stature considering the anterior mandibular tooth dimensions [12]. Quite a few studies were conducted to estimate stature using this formula [4,8,12,13].
With the increasing frequency of natural and man-made mishaps, there is always a need for such studies which help in identifying the victims of the same where the literature is quite scanty. In such situations, a better correlation between dental measurements and stature can be useful in anthropology and forensic identification. An updated research among the population residing at various geographic zones is of prime importance in preserving the records which could aid in identification process [14-16].
The current study has enrolled the mixed population of southern India and to our knowledge this is the first study of its kind to be conducted using Carrea’s index among this section of Indian population. Given the paucity of literature and a need to bridge the gap between the odontometric measurements and forensic science, the study was undertaken with an aim to determine the possible correlation between tooth dimensions and stature estimation using Carrea’s index.
Materials and Methods
The present cross-sectional study was carried out among the subjects reported to the Department of Oral Medicine, Oral Diagnosis and Radiology, Vishnu Dental College, Bhimavaram, Andhra Pradesh, India. An observational cross-sectional study was conducted among 82 individuals aged between18 to 30 years selected using convenience sampling. Each subject was explained about the need for the study and intervention to be conducted on them. A written informed consent was obtained from each subject before enrollment into the current study. Ethical approval was obtained for this study from the Institutional Research Ethics Committee.
Subjects of either sex aged between 18-30 years were included in the study. Subjects having complete set of intact mandibular anterior teeth with healthy periodontium and the subjects who had agreed to participate and signed the terms of informed consent were included in the study.
Individuals with history of orthodontic treatment and syndromes which interferes with growth of the body or tooth anomalies which alters the tooth dimensions were excluded from this study.
Actual height of each participating subject was measured and lower dental casts of those subjects were obtained after taking alginate impressions. The sampling unit was one hemiarch, so 82 subjects were selected to give a sample size of 164 hemiarches. For examining the casts, each hemiarch was considered separately, equaling 164 inferior hemiarches, which were divided according to the dental alignment into three groups.
The following is the criteria under which categorization of arches have been done [17].
Normal (n=85): The arches that presented with regular dental positioning that had no crowding or spacing between the canine, lateral incisor and central incisor.
Crowded (n=53): Crowding between canine, lateral incisor or central incisor, loss of perimeter bow manifested in the absence of interdental space and consequent misalignment of the anterior teeth.
Diastema (n=26): Presence of spaces among teeth resulting in lack of interproximal contact. Diastema is considered between canine, lateral incisor or central incisor.
The measurements of each hemiarch were performed as described by Carrea (1939) [12].
Data Collection
Measurement of height (real stature): The measurements of real stature were made using standard anthropometer by making the subject stand erect on the horizontal plane, barefooted, in the anatomical position according to the Frankfort plane, in inspiratory apnoea, aligning the posterior surface of heels, pelvic girdle, scapular girdle, and occipital region to the vertical plane. The distance of the subject from the ground to the highest point of the vertex in the median sagittal plane was recorded [8].
Dental measurements (estimated stature): The patient was made to seat comfortably in dental chair and plaster models of the lower dental arch of each subject were obtained using alginate impressions. A standardized procedure was followed for mixing of dental stone with water, taking fixed water/powder ratio (W/P ratio) for all the models constructed.
Analysis of measurements on lower dental casts: On examining the cast, each hemiarch was considered separately and measurements of arch and chord values were made for each hemiarch. The obtained chord and arch values were inserted in the formula described by Carrea to obtain maximum and minimum statures in centimeters [12].
Arch (maximum stature): Sum of the mesiodistal diameters of lower central incisor, lateral incisor and canine, were measured on the labial surface of teeth using digital caliper [Table/Fig-1].
Chord (minimum stature): Linear distance between the ends of the arch, represented by the mesial edge of central incisor and the distal edge of canine on the same side, measured on the lingual surface with a digital caliper [Table/Fig-2].
Measurement of ‘Arch’ (mesio-distal dimensions on labial surface) using digital calliper.
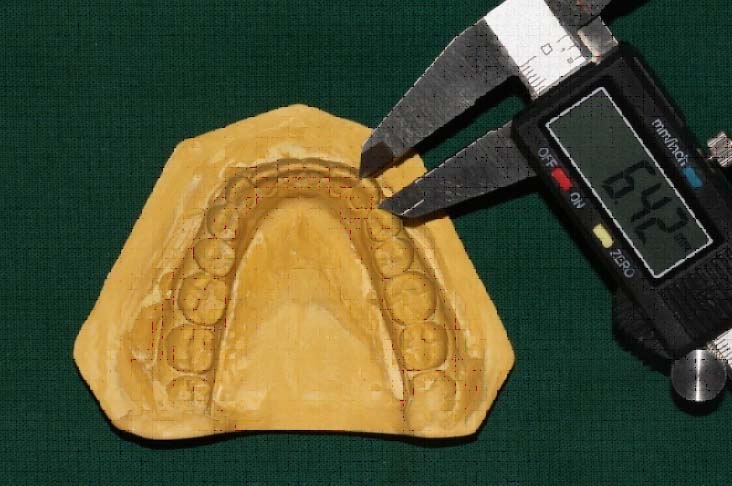
Measurement of ‘Chord’ (lingual surface) using digital calliper.

These measured chord and arch values for each tooth were substituted in the formula given by Carrea to obtain the minimum and the maximum estimated height of a person [12]. These resultant values were estimated by following method and compared with real stature.
Successful prediction: The real stature measurements coincided with the interval between the minimum (chord) and maximum (arch) estimated stature measurements (tooth dimensions).
Unsuccessful prediction: The real stature measurements which does not coincide with the interval between the minimum (chord) and maximum (arch) estimated stature measurements (tooth dimensions).
Accuracy/deviation between actual and estimated stature was calculated from obtained values and the number of cases that fall within and out of range of estimated height for each kind of arch (i.e., Normal, Crowded and Diastema) were also quantified. All the measurements as well as clinical examinations were conducted by a single dentist. The intra-examiner variability for the measurement of the actual height and the arch and chord values of 12 casts was assessed.
Statistical Analysis
The data was then analyzed using the SPSS software (version 11.5). Frequencies of accurate height assessment were measured. Proportion of accurate measurements were compared according to sex, the types of dental alignment and side of arch utilizing Chi square test and the Pearson’s coefficient test to know the reliability of Carrea’s index. A p-value of <0.05 was taken as statistically significant.
Results
Regarding the intra examiner test, there was a reliable result by the Kappa index (0.74), with a confidence interval of 95%. The descriptive statistics related to sex for each kind of dentition consists a total of 42 male (51.6%) and 40 female (48.7%) subjects which make a sample of 164. When all the 164 inferior hemiarches were grouped accordingly (Normal, Crowded and Diastema) highest number of individuals (85) were present with normal dental alignment.
[Table/Fig-3] shows the comparison of mean estimated stature with the mean actual stature of the subjects. In the sample of 164, the adult males showed higher mean actual stature and estimated stature values. The calculated estimated height (162.5±6.4cm) for males differs by 2.5±1.25cm from actual height of males (165±5.15cm) whereas in females, the estimated height (155±11.3cm) differs by 2.5±6.15cm from actual height of females (157.5±5.15cm).
Descriptive statistics of the actual stature and estimated stature (arch and chord) values in the study population.
| Measurement (in cm) | Males | Females | Total |
|---|
| Actual | 165±5.15 | 157.5±5.15 | 160±5.2 |
| Maximum Height | 167.5±5.18 | 160±5.15 | 162.5±7.5 |
| Minimum Height | 157.5±7.7 | 150±17.5 | 155±12.5 |
| Total Estimated Height | 162.5±6.4 | 155±11.3 | 158.8±10 |
Mean values
[Table/Fig-4] shows the distribution of successful and unsuccessful predictions of arches with normal alignment according to sex. Out of 85 normal arch population, 65 individuals (76.5%) were within the estimated height range and 20 (23.5%) were out of estimated height range. Higher success rate was seen among males (81.8%) compared to females (73.1%). The same inference can be obtained when sides were compared where 72 individuals (84.7%) showed successful prediction and 13 individuals (15.29%) showed unsuccessful prediction and moreover, right side showed higher success rate (87.2%) when compared to left side (81.57%).
Distribution of successful and unsuccessful predictions for normal arches according to sex and side.
| Normal Dental Alignment |
|---|
| Males | Females | Total | Right | Left | Total |
|---|
| N | % | N | % | N | % | N | % | N | % | N | % |
|---|
| Successful prediction | 27 | 81.8 % | 38 | 73.1 % | 65 | 76.5 % | 41 | 87.2 % | 31 | 81.6 % | 72 | 84.7 % |
| Unsuccessful prediction | 6 | 18.2 % | 14 | 26.9 % | 20 | 23.5 % | 6 | 12.8 % | 7 | 18.4 % | 13 | 15.3 % |
| Total | 33 | 100 % | 52 | 100 % | 85 | 100 % | 47 | 100 % | 38 | 100 % | 85 | 100 % |
| p-value | 0.172 | 0.239 |
Chi –square test
[Table/Fig-5] shows the distribution of successful and unsuccessful predictions of arches with crowded alignment according to sex. Out of 53 crowded arch samples, 38 subjects (71.6%) showed successful prediction and 15 subjects (28.4%) showed unsuccessful prediction. Higher success rate was seen among males (76.5%) compared to females (63.1%) but with no statistically significant difference (p=0.016). The same inference can be obtained when sides were compared where 40 individuals (75.5%) showed successful prediction and 13 individuals (24.5%) showed unsuccessful prediction and yet again right side showed higher success rate (80.0%), when compared to left side (71.4%), with no statistical difference between them (p=1.00).
Distribution of successful and unsuccessful predictions for crowded arches according to sex and side.
| Crowded Dental Alignment |
|---|
| Males | Females | Total | Right | Left | Total |
|---|
| N | % | N | % | N | % | N | % | N | % | N | % |
|---|
| Successful prediction | 26 | 76.5 % | 12 | 63.1 % | 38 | 71.6 % | 20 | 80.0 % | 20 | 71.4 % | 40 | 75.5 % |
| Unsuccessful prediction | 8 | 23.5 % | 7 | 36.9 % | 15 | 28.4 % | 5 | 20.0 % | 8 | 28.6 % | 13 | 24.5 % |
| Total | 34 | 100 % | 19 | 100 % | 53 | 100 % | 25 | 100 % | 28 | 100 % | 53 | 100 % |
| p-value | 0.016 | 1.00 |
Chi –square test
[Table/Fig-6] shows the distribution of successful and unsuccessful predictions of estimation of arches with diastema alignment according to sex, which shows mere balanced distribution of success and failure for estimation of height. Out of total 26 subjects, 14 subjects (53.9%) were within the range of estimated height and 12 subjects (46.1%) were outside the range of estimated height. There was a 52.9% and 55.5% success rate for males and females respectively but with no statistically significant difference (p=0.197). The right sided hemiarches showed a higher success rate (60.0%) as compared to the left side (43.75%) and half of the individuals showed successful prediction (50%) and other half showed (50%) unsuccessful prediction.
Distribution of successful and unsuccessful predictions for arches with diastema, according to sex and side.
| Diastema Dental Alignment |
|---|
| Males | Females | Total | Right | Left | Total |
|---|
| N | % | N | % | N | % | N | % | N | % | N | % |
|---|
| Successful prediction | 9 | 52.9 % | 5 | 55.5 % | 14 | 53.9 % | 6 | 60 % | 7 | 43.75 % | 13 | 50.0 % |
| Unsuccessful prediction | 8 | 47.1 % | 4 | 44.4 % | 12 | 46.1 % | 4 | 40 % | 9 | 56.25 % | 13 | 50.0 % |
| Total | 17 | 100 % | 9 | 100 % | 26 | | 10 | 100 % | 16 | 100 % | 26 | 100 % |
| p-value | 0.197 | 0.593 |
Chi –square test
[Table/Fig-7] represents that correlation is significant at the 0.05 level (2-tailed). All the estimated measurements show significant positive correlation with actual stature and it also depicts that the correlation between the estimated heights through Carrea’s index with the actual height, is at 0.05 level of significance. The correlation coefficient of 0.8 for estimated height on right side and 0.4 for left side indicates there is a true relation between estimated height and actual height.
Correlation of actual height with estimated height.
| | Maximum estimated height right | Minimum estimated height right | Maximum estimated height left | Minimum estimated height left |
|---|
| Actual Height | Pearson’s Correlation | 0.880** | 0.457** | 0.847** | 0.444** |
| p-value | 0.001* | 0.001* | 0.001* | 0.001* |
| N | 82 | 82 | 82 | 82 |
Pearson’s correlation coefficient
Discussion
Stature forms the basic pillar in anthropological protocol and has utmost importance in reconstruction and identification of skeletal remains. Validity of stature estimation through body parts such as facial bones, long bones, trunk and foot bones have already been established; whereas, stature estimation through tooth dimensions is quite scanty in literature. At this juncture, the current study is undertaken to fill this lacuna. In various instances, tooth has been the tool of research in the process of stature estimation.
If there were to exist a correlation between teeth and stature, the likelihood of embryological relationship between tooth formations and long bones almost explains this phenomenon. Both, dentin that forms bulk; depicts the tooth dimensions and long bones which determines the height or stature of an individual are basically derived from mesenchymal tissue (Dentin-Ectomesenchyme; Long bones-Mesoderm) and have similarities in structural composition [9]. Henceforth, it is presumable to accept the mere relationship between teeth and stature.
In the present study, out of 164 inferior hemiarches considered, highest percentage (51.8%) of individuals were shown to have normal arches. The minimum estimated statures were lower than the actual stature and on the other hand, the maximum estimated statures were higher than the actual statures. The total mean actual height of the sample (160±5.2cm) differs by 1.2±4.8cm from total mean estimated height sample (158.8±10cm), this depicts that actual height was within the range of estimated height (i.e., within maximum and minimum height). The calculated estimated height for males (162.5±6.4cm) differs by 2.5±1.25cm of actual height (165±5.15 cm) whereas in females, the estimated height (155±11.3cm) differs by 2.5±6.15cm of actual height (157.5±5.15cm) [Table/Fig-3]. In the current study, when real/actual statures were measured, males showed high mean actual stature than females. Similarly, the estimated height measured from tooth dimensions also showed higher mean values among males than females.
When successful and unsuccessful predictions were compared among both the genders in the normal arch group, a higher percentage of success rate was observed, though males showing the highest percentage of correct estimated height. Similar results were obtained when sides of the arches (normal) were compared, with right side showing the highest success rate (87.2%) [Table/Fig-4].
The above findings are in accordance with the results obtained from the observations of originally described Carrea’s index and also with the findings of Lima L et al., [13]. This shows the relative acceptance of Carrea’s index in the studied sample. The categorization of the arches (Normal, Crowded and Diastema) in the present study is not in accordance with the previous original studies [18] where the crowded and normal arches were considered together.
Unlike few other studies which had discarded the application of Carrea’s index on crowded arches, the present study results have revealed that Carrea’s index is applicable on crowded arches and highest percentage of hits were recorded among males (76.5%) and on right side [Table/Fig-5] bearing a slight difference with that of females (63.1%) which suggests an overall appreciable success rates. The results are contradictory to the findings of Croce and Croce junior [19] who had opposed the use of Carrea’s index in crowded arches. The significant success rate and successful predictions obtained in the crowded arches might have been due to the individual measurements of each tooth using digital calipers where accurate measurements of each tooth were obtained.
In case of hemiarches with diastema, a lower success rate was seen compared to other arch groups [Table/Fig-6]. This can be attributed to the fact that there exists difference between the estimated arch and chord value. In case of diastema subjects there is an increase in the chord values. The results are in accordance with the observations made by Rekhi A et al., and Lima L et al., [8,13]. Normally, the chord values pertaining to the arches are lesser than that of arch values which are higher. But in case of diastema arches, as the spacing is present between the teeth, there is compromise in chord value. This in turn led to error between minimum stature and maximum stature values. The error occurred with this difference might have been the reason for low success rate percentage [4,8].
Based on the results obtained and considering the principle of bilateral symmetry and eliminating small variations as normal asymmetries [20], the present study shows that Carrea’s index is applicable on crowded arches. In the present study, there was a higher correlation between stature estimation and right side of hemiarches but statistically insignificant. These observations are contradictory to the findings of Calvacanti AL et al., [17] who had shown equivalent success rates for both sides (modified method) and higher correlation to left hemiarch (conventional method). This can be best explained based on the factors such as plasticity, which is the ability of the dentition to physically adjust to changing environmental conditions which might alter the dimension of tooth and also on the ethnic difference where the present study was carried out in southern part of India.
When Pearson’s correlation was assessed [Table/Fig-7], a significant correlation was obtained between actual stature and estimated stature using Carrea’s index. When sides of arches were considered the highest correlation was found on right side, this implies that as actual height increases, the estimated parameters also increases. Interestingly, the present study has witnessed the mere close relationship between actual height and estimated maximum height among males.
Limitation
The present study was intended mainly to ascertain the level of correlation between tooth dimensions and actual stature of an individual. This is shown to be true in the current study where strong correlation was established between tooth dimensions and real stature. Nevertheless, few limitations refrains the study from its possible correlation between tooth dimensions and stature estimation. Primarily, low sample size in the current study is a major drawback where if larger population was included, the study could have been detailed better about the accuracy and application of Carrea’s index. The other limitation could be the age group, where a little increase in the inclusion of age group of the subjects would provide a better view of the reliability of tooth dimensions in estimating stature. Finally, lack of regression equation analysis on the current study population also remains a drawback of the study.
Conclusion
Estimation of height/stature is a key element in person identification. The present study within its limitations, has reasonably achieved a moderate correlation and Carrea’s index had achieved a satisfactory success rate among males and females; between right and left dental arches. Henceforth, Carrea’s index is applicable to the current population. The overall tooth-stature correlation suggests that assessment of tooth dimension can be used as an adjuvant method in identifying a person.
Nevertheless, any person identification procedures have to be tested and validated on local samples. So, the future research is directed towards the establishment of a strong correlation between tooth dimensions and stature considering the variation levels in human ethnic groups so that it can be useful in anthropological and forensic identification.
Mean values
Chi –square test
Chi –square test
Chi –square test
Pearson’s correlation coefficient