Micrometastasis Detection using Special Stains in Nodal Tissues of Oral Squamous Cell Carcinoma – A Histochemical Study
Wasim Raja Mumtaz1, Veda Hegde2, Nikhil Yadav3
1 Postgraduate Student, Department of Oral Pathology, SDM College of Dental Sciences and Hospital, Dharwad, Karnataka, India.
2 Professor, Department of Oral Pathology, SDM College of Dental Sciences and Hospital, Dharwad, Karnataka, India.
3 Postgraduate Student, Department of Oral Pathology, SDM College of Dental Sciences and Hospital, Dharwad, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Wasim Raja Mumtaz, Department of Oral Pathology, SDM College of Dental Sciences and Hospital, Dharwad-580009, Karnataka, India.
E-mail: wasi.doc@gmail.com
Introduction
Micrometastasis to the lymph node is an important prognostic factor in survival and recurrence and even in making critical decisions regarding postoperative radiation treatment. Methods like Immunohistochemistry (IHC), serial sectioning and Polymerase Chain Reaction (PCR) are very sensitive; however, they are expensive and time consuming. Hence, there is a need for the detection of micrometastasis by method which is easily feasible and inexpensive.
Aim
This study was undertaken to identify if special stains (Modified Papanicolaou stain and Ayoub Shklar stain) are valuable in detecting micrometastasis which are routinely missed in Haematoxylin and Eosin stain and also to compare their efficacy over Haematoxylin and Eosin stain in detection of metastatic tumour cells in non-metastatic lymph nodes.
Materials and Methods
This study constituted a total of 300 histopathologically proven non metastatic lymph node sections. Other than Haematoxylin and Eosin stain, Modified Papanicalaou and Ayoub Shklar stain were used for identification of micrometastatic deposit.
Results
Papanicolaou stain was the only stain useful in detecting micrometastasis which accounted to 7% of non metastatic lymph node sections used in our study.
Conclusion
Papanicolaou stain has definitely proved valuable in detecting micrometastasis over routine Haematoxylin and Eosin and Ayoub Shklar stain with an added advantage of being economical, easily available and technique insensitive.
Haematoxylin and Eosin stain, Lymph nodes, Metastasis, Papanicoloaou stain
Introduction
Oral cancer is the 6th most common cancer worldwide. In India, it accounts for one fourth of cancers in males and one tenth of cancers in females [1]. Squamous Cell Carcinoma of the Head and Neck (SCCHN) frequently metastasizes to the regional lymph nodes; hence, the status of the cervical lymph nodes is the most important prognostic factor in squamous cell carcinoma of the upper aerodigestive tract. The status of lymph node like number of metastatic nodes, extracapsular spread, size of the node, level of metastatic nodes and histopathological features in the involved nodes are the commonly used prognostic factors. The amount of changes brought about by the metastatic deposits in the cervical lymph nodes is significantly important for survival of and recurrence in the patient. Hence, histopathological evaluation of cervical lymph nodes provides basic information for diagnosis, staging and prognosis [2].
A macrometastasis is a nodal deposit which can be identified either by the surgeon on physical examination or by the radiologist via imaging studies, but assessing the lymph node in the absence of clinical enlargement is challenging, even the most sophisticated imaging procedures may not be able to reveal small foci of tumour cells or micrometastasis [3]. Ferris RL et al., in their study had mentioned that preoperative clinical methods and newer radiographic techniques are suboptimal and misdiagnose the presence or absence of nodal metastasis in many patients [4]. The major limitation of analysis of lymph node with routine Haematoxylin and Eosin stain is that micrometastasis are often missed. Studies have shown that routine evaluation misses up to 21% of diseased nodes and the risk of micrometastasis is particularly high for cancers of the oral cavity, oropharynx, hypopharynx and supraglottis [5]. The presence of even a single island of micrometastasis in a lymph node has the potential to seriously affect the recurrence and survival for the patient. Approximately 10% of patients have been reported with regional recurrence who were histologically diagnosed as non metastatic, suggesting that tumour cells were present but not detected in the resected nodes [6].
Although various sensitive methods are available for detection of micrometastasis like Immunohistochemistry (IHC), Reverse Transcriptase Polymerase Chain Reaction (RT-PCR) and serial sectioning, but these have various disadvantages. Both IHC and RT-PCR are expensive and technique sensitive, so it is practically not possible for the surgeon to subject so many nodes to detect micrometastasis. Similarly serial sectioning has the disadvantage of being very laborious and time consuming. Hence, there is a need for the detection of micrometastasis by a method which is easily feasible and inexpensive. Thus, this study was undertaken to identify if special stains (Modified Papanicolaou stain and Ayoub Shklar stain) are able to detect micrometastasis which are routinely missed in Haematoxylin and Eosin stain.
Materials and Methods
This retrospective study consisted of evaluation of a total of 300 sections of lymph nodes, 100 each stained by Haematoxylin and Eosin stain, modified Papanicolaou stain and Ayoub Shklar stain. It included paraffin embedded tissue blocks of 100 lymph node specimens histopathologically diagnosed as non-metastatic, obtained from 73 oral squamous cell carcinoma patients who had undergone neck dissection, retrieved from the archives of Department of Oral Pathology and Microbiology of SDM College of Dental Science and Hospital, Sattur, Dharwad, Karnataka, India. The study protocol was approved by the Institutional Review Board of the above mentioned institution.
Level I and Level II lymph nodes of sizes equal to/or greater than 1cm at their greatest diameter were included in the study. These lymph nodes did not show any metastatic deposit when analyzed with ultrasonography. All 100 sections of histopathologically proved non metastatic lymph node which were stained by routine Haematoxylin and Eosin stain were re-evaluated for detection of micrometastasis. A total of 100 sections each were then stained by both Modified Papanicolaou stain and Ayoub Shklar stain. Phloxin B was added in Papanicolaou stain so that it could be used on paraffin embedded sections instead of cytosmear. Phloxine-B, a red acid dye with distinctly bluish shade is used to stain mucin, prekeratin and keratin which appear conspicuously red in colour [7]. Moreover, the time of staining was also increased in our study to 1hr each for Orange G and Eosin Azure compared to 5 minutes in cytosmears. All the 300 sections were then analyzed for the detection of micrometastasis and the results of all the three stains were compared to evaluate the efficacy of these three stains in detecting micrometastasis. Two oral pathologists independently evaluated the stained sections and agreement was taken when necessary. Since the number of micrometastasis detected were only seven out of 300 lymph node sections, statistics could not be applied. Analysis was done based on percentage evaluation.
Results
The age of 73 patients ranged from third to seventh decade of life. Out of 73 patients in the study, five were females and 68 were males. A 63% of them had the habit of smokeless tobacco and site of distribution predominantly was buccal mucosa (58%). Forty nine were of well differentiated, 14 were of well to moderately differentiated, nine were of moderately differentiated and one was of moderate to poorly differentiated.
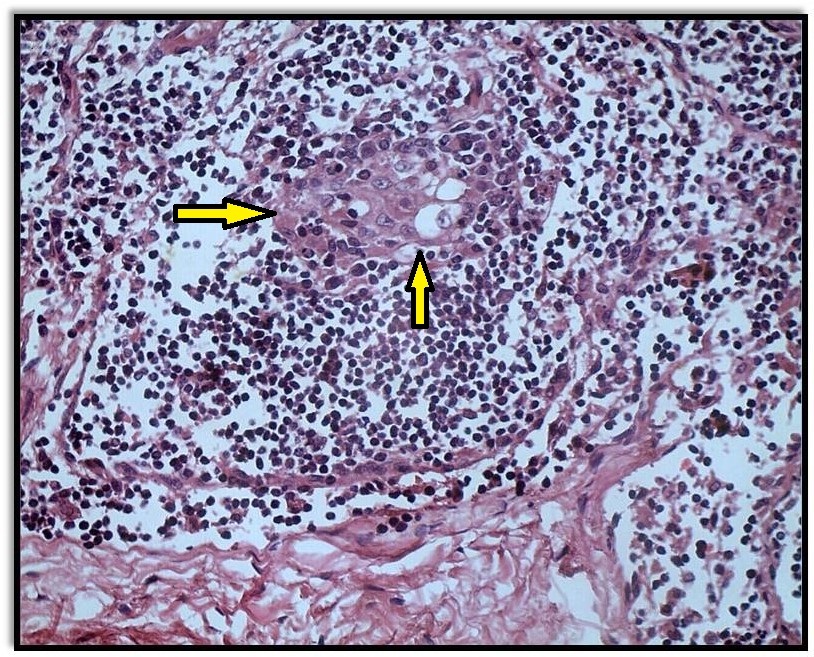
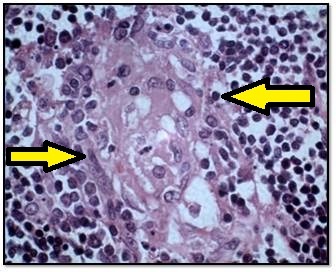
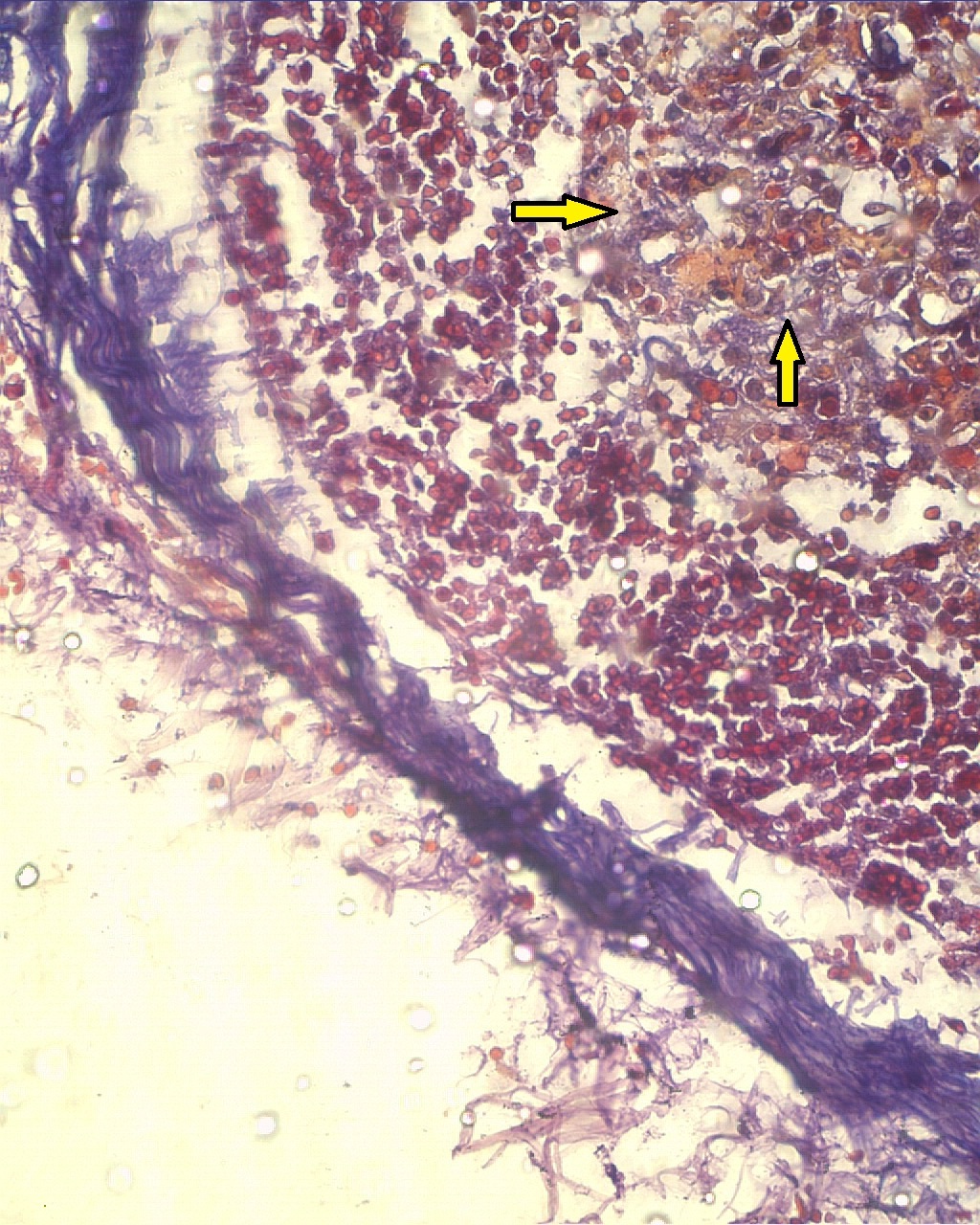
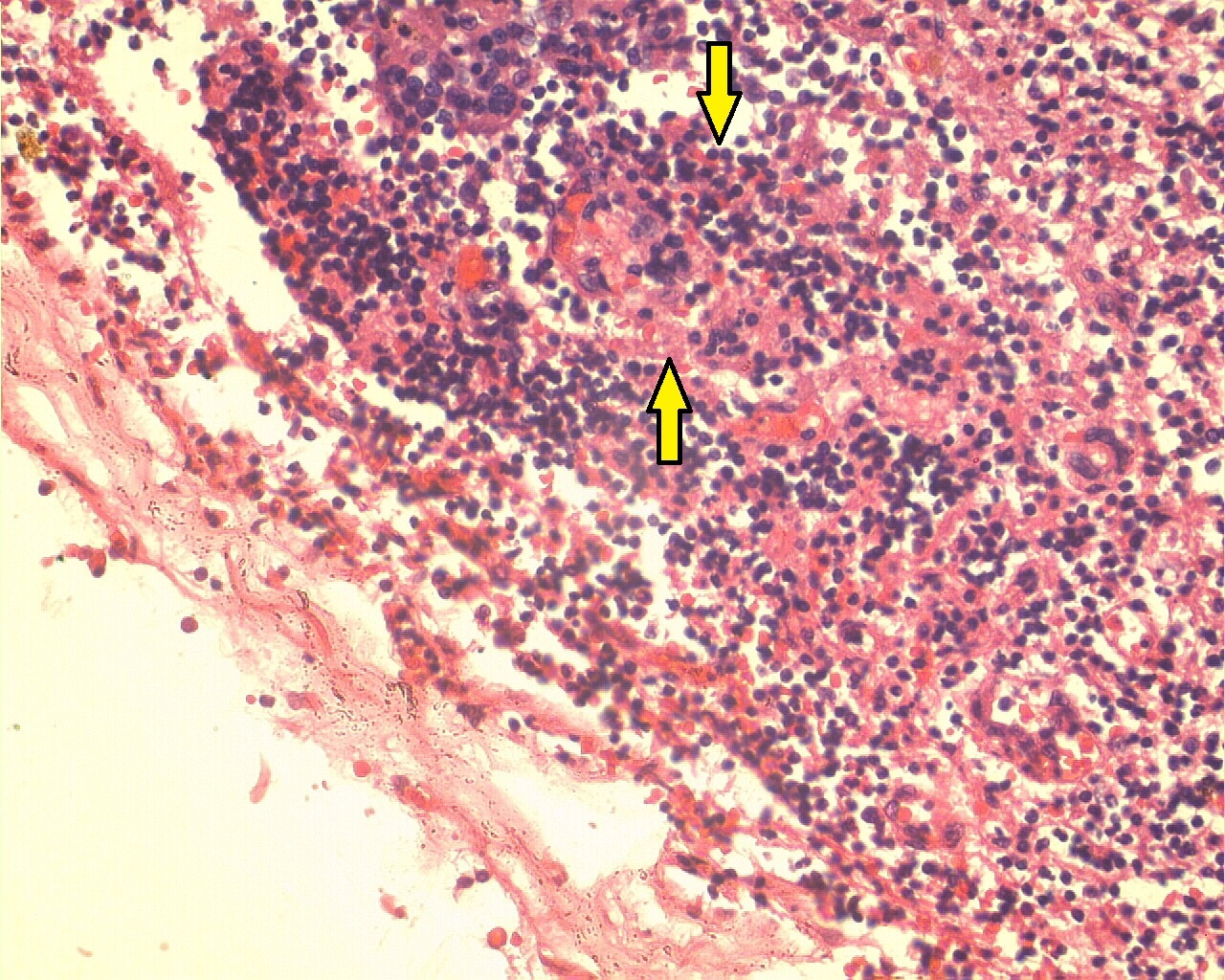
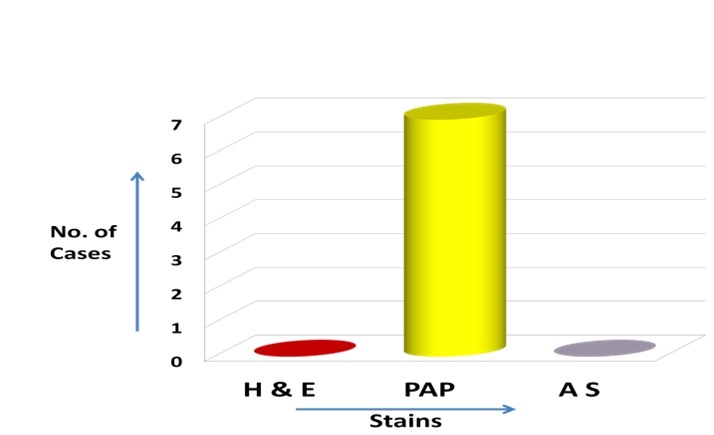
Out of the 300 sections which were analyzed for detection of micrometastasis, seven sections stained by Modified Papanicolaou stain showed positivity in detecting micrometastasis [Table/Fig-1,2]. In these seven cases, five were males and two were females with predominant site being buccal mucosa and all of them had the habit of chewing smokeless tobacco. All these seven cases were histologically graded as well differentiated squamous cell carcinoma [Table/Fig-3]. Micrometastatic deposit was located in the subcapsular sinus of the lymph node in all these seven cases. Both Ayoub Shklar stain [Table/Fig-4] and Haematoxylin and Eosin stain [Table/Fig-5] were ineffective in detecting micrometastasis in all the sections examined [Table/Fig-6].
Photomicrograph reveals micrometastatic deposits in subcapsular area stained by Papanicolaou stain (x40).
Photomicrograph reveals micrometastatic deposits in lymph node stained by Papanicolaou stain (x100).
Clinical details, staging, grading and size of the node in seven positive cases.
| CaseNo. | Age | Sex | Site | Habit | Histologicgrading | TNM staging | Size of LN(cm) |
|---|
| 1. | 55 | F | Tongue | Smokeless Tobacco | Well Differentiated | T2N1M0 | 1.2x1 |
| 2. | 60 | M | Lip | Smokeless Tobacco | Well Differentiated | T2N1M0 | 1.5x1 |
| 3. | 42 | M | Tongue | Smokeless Tobacco | Well Differentiated | T3N1M0 | 1x.8 |
| 4. | 55 | F | Buccal Mucosa | Smokeless Tobacco | Well Differentiated | T3N1M0 | 1x.6 |
| 5. | 32 | M | Buccal Mucosa | Smokeless Tobacco | Well Differentiated | T3N1M0 | 1x.8 |
| 6. | 32 | M | Buccal Mucosa | Smokeless Tobacco | Well Differentiated | T3N1M0 | 1x.5 |
| 7. | 37 | M | Buccal Mucosa | Smokeless Tobacco | Well Differentiated | T3N1M0 | 1x1 |
Photomicrograph of the lymph node sections stained by Ayoub Shklar stain (x40).
Photomicrograph of the lymph node sections stained by Haematoxylin and Eosin stain (x40).
Comparison of the efficacy of all the three stains in detecting micro-metastasis in lymph node sections.
Discussion
Metastatic deposits in the regional lymph nodes have always been a subject of great concern in oncology. Different authors have defined micrometastasis; like Black et al., defined micrometastasis as tumours occupying < 20% of the sections area [8]. De Mascarel et al., defined micrometastasis as tumour deposits which measured less than 0.5mm in span [9]. Tumour deposits within the lymph nodes were classified and staged according to the revised guidelines by the Union for International Cancer Control (UICC) which defined metastasis occupying between 0.2mm to 0.2cm of the sectioned area as micrometastasis [10]. Various studies have been done for the detection of micrometastasis in breast cancer and all of them have shown to have a significant difference in prognosis of the patient [8,9]. Few studies have been published on the detection of micrometastasis in the cervical lymph node of oral squamous cell carcinoma but the literature is scanty [11].
Level I lymph nodes are drained by the anterior oral cavity while Level II are drained by the posterior parts of the oral cavity. About 50% of the patients suffering from oral cancer reveal lymph node metastasis [12]. Hence in the present study Level I and Level II lymph nodes were included as the metastasis of oral cancers predominantly takes place in Level I and Level II lymph nodes.
Radical neck dissection leads to a significant functional and cosmetic morbidity of the affected patients. Two most common complications after neck dissection are intraoperative opening of internal jugular vein and postoperative thrombosis [12]. Moreover, the risk of developing a chylus fistula after radical neck dissection amounts to an average of 1-2.5% with a majority (75-90%) on the left side [13]. Another important complication after neck dissection is the functional disturbance of the accessory nerve, which may lead to complex clinical symptoms, the so called shoulder-arm syndrome [14]. So, if patient after undergoing such major surgery suffers recurrence, the chance of morbidity of the patient increases drastically. This shows the importance of detection of even a single micrometastasis, which has a significant role in prognosis and survival of the patient.
Papanicolaou stain is a routinely used stain, commonly available in laboratories. It is a multichromatic stain containing Harris’s Haematoxylin, Orange G6, Eosin-Azure and is used to differentiate cells in cytosmear preparations for various body secretions. The main use of Orange G6 in the Papanicolaou stain is to stain keratin. Superficial cells with high content of keratin stain yellow-orange hue and parabasal cells stain green to blue in colour [7]. Ayoub Shklar stain consists of two solutions. Solution 1 consists of 5% Acid Fuschin and Solution 2 consists of Aniline Blue, Orange G and Phosphotungstic acid. It is also used to stain keratin, brilliant orange in colour [7].
Papanicolaou stain though commonly used for cytosmears has been used to stain paraffin embedded tissue sections for demonstration of keratin. Since very few studies have been done using Papanicolaou stain in tissue sections, there is scarcity of published data. Johnson Pergy L and Klein Morris N, in 1956 reported the use of Papanicolaou stain in paraffin embedded tissue sections, for staining of keratin [15]. Elzay RP has reported the addition of phloxine B on papanicolaou stain to demonstrate keratin in tissue sections [16]. Preethis et al., in their study compared the efficacy of Haematoxylin and Eosin stained tissue sections with Papanicolaou stained tissue sections and concluded that Papanicolaou stains more clearly demonstrated key morphological features associated with keratinization [17]. Rao RS et al., in their study compared special stains like Papanicolaou stain and Ayoub Shklar stain to demonstrate keratin in tissue sections of various cases like normal gingival, hyperkeratosis, squamous papilloma, verrucous hyperplasia, verrucous carcinoma, well differentiated squamous cell carcinoma and keratocystic odontogenic tumour and concluded that the above mentioned special stains have the potential to be used as an alternative stain for keratin [18]. Similarly Ramulu S et al., used modified Papanicolaou stain and Ayoub Shklar stain for stain keratin in well differentiated squamous cell carcinoma, verrucous carcinoma and odontogenic keratocyst and concluded the efficacy of both modified Papanicolaou stain and Ayoub Shklar stain to be comparable with Haematoxylin and eosin stain [7]. The above mentioned studies were done in tissue sections of different cases like verrucous carcinoma, well differentiated squamous cell carcinoma etc., but these special stains (modified Papanicolaou and Ayoub Shklar stain) were used for the first time in lymph nodes in our study utilizing the basic concept that above mentioned stains are keratin specific stains and that keratins are frequently the most abundant cellular proteins which constitute the major component of the cytoskeleton of all epithelial cells. These intermediate filaments provide mechanical support for the cells and nucleus [7]. Thus, keratins can be used as a marker protein to detect metastatic epithelial cells or micrometastasis. These stains may highlight even small foci of overt epithelial differentiation that sometimes is missed in routine Haematoxylin and Eosin staining by imparting orange to pink colour to the cytoplasm of the metastatic epithelial cells.
In the present study, Ayoub Shklar stain was not useful in detecting micrometastasis as the metastatic tumour cells could not be differentiated from other lymphoid cells even though strict staining protocol was followed. Modified Papanicolaou stain definitely proved valuable in detecting micrometastasis. Modified Papanicolaou stain has advantage of being inexpensive, easily available, routinely used and more sensitive in identifying micrometastatic deposit as seen in the present study, so it can be used as an adjunct to a routinely used more sensitive IHC marker, Pancytokeratin, to stain lymph nodes of oral squamous cell carcinoma patients. Micrometastatic deposit identified by modified Papanicolaou stain can be confirmed using IHC marker Pancytokeratin which will help us to further strengthen the role of Pancytokeratin in detecting micrometastasis. Hence, if all the lymph node sections are stained and analyzed for micrometastasis with Modified Papnicolaou stain instead of routine Haematoxylin and Eosin stain as the former has proved to be more efficient, and then the suspected lymph node sections be further confirmed with Pancytokeratin instead of subjecting all the lymph nodes to Pancytokeratin, then even a single micrometastasis can be detected in a very economical manner; thus, preventing recurrence and improving survival of the patient.
Limitation
This study has few limitations like the sample size was too small to be analyzed statistically. Also, the hypothesis that whether the two special stains mentioned in this study can be used to detect micrometastasis is debatable. Hence, more extensive studies are required in this field.
Conclusion
The present study concluded that modified Papanicolaou stain is definitely valuable and sensitive in detecting micrometastasis over Haematoxylin and Eosin stain and Ayoub Shklar stain. Detection of micrometastasis post surgically is definitely beneficial for the patient as it alters the treatment plan for the patient in terms of both radiotherapy and chemotherapy. As this stain was used for the first time in lymph node with various alterations in time and concentration, still better results may be obtained if further studies are done on it.
[1]. Agarwal P, Chaudhary M, Patil S, Hande A, Gawande M, Agarwal P, Diagnostic accuracy of various methods to detect lymph node metastasis in oral squamous cell carcinomaJ Evolution Med Dent Sci 2014 3(22):6003-10. [Google Scholar]
[2]. Ambrosch P, Brinck U, Detection of nodal micrometastases in head and neck cancer by serial sectioning and immunostainingOncology (Williston Park) 1996 10(8):1221-26. [Google Scholar]
[3]. Ferlito A, Rinaldo A, False negative conventional histology of lymph nodes in patients with head and neck cancerORL J Otorhinolaryngol Relat Spec 2000 62:112-14. [Google Scholar]
[4]. Ferris RL, Xi L, Raja S, Hunt JL, Gooding WE, Kelly L, Molecular staging of cervical lymph nodes in squamous cell carcinoma of the head and neckCancer Res 2005 65(6):2147-56. [Google Scholar]
[5]. Shivers SC, Wang X, Li W, Joseph E, Messina J, Glass LF, Molecular staging of malignant melanoma: Correlation with clinical outcomeJAMA 1998 280(16):1410-15. [Google Scholar]
[6]. Thakare E, Gawande M, Chaudhary M, Seralathan M, Kannan K, Detection of micrometastasis in lymph nodes of oral squamous cell carcinoma: A comparative studyJ Oral Maxillofac Pathol 2013 17(3):374-80. [Google Scholar]
[7]. Ramulu S, Kale AD, Hallikerimath S, Kotrashetti V, Comparing modified papanicolaou stain with ayoub-shklar and haematoxylin-eosin stain for demonstration of keratin in paraffin embedded tissue sectionsJ Oral Maxillofac Pathol 2013 17(1):23-30. [Google Scholar]
[8]. Black RB, Roberts MM, Stewart HJ, Prescott R, Cant EL, Sumerling MD, The search for occult metastases in breast cancer: does it add to established staging methods?Aust N Z J Surg 1980 Dec 50(6):574-79. [Google Scholar]
[9]. de Mascarel I, Bonichon F, Coindre J M, Trojani M, Prognostic significance of breast cancer axillary lymph node micrometastases assessed by two special techniques: reevaluation with longer follow-upBr J Cancer 1992 66(3):523-27. [Google Scholar]
[10]. Prakash AR, Kumar GS, Shetty P, A Study on the detection of micrometastasis in the cervical lymph nodes of oral squamous cell carcinomas by serial sectioningJ Clin and Diagn Res 2011 5(1):78-81. [Google Scholar]
[11]. Ferlito A, Rinaldo A, Devaney KO, Nakashiro K, Hamakawa H, Detection of lymph node micrometastases in patients with squamous carcinoma of the head and neckEur Arch Otorhinolaryngol 2008 265(10):1147-53. [Google Scholar]
[12]. Teymoortash A, Werner JA, Current advances in diagnosis and surgical treatment of lymph node metastasis in head and neck cancerGMS Curr Top Otorhinolaryngol Head Neck Surg 2012 11:Doc04 [Google Scholar]
[13]. De Gier HH, Balm AJ, Bruning PF, Gregor RT, Hilgers FJ, Systematic approach to the treatment of chylous leakage after neck dissectionHead Neck 1996 18(4):347-51. [Google Scholar]
[14]. Cheng PT, Hao SP, Lin YH, Yeh AR, Objective comparison of shoulder dysfunction after three neck dissection techniquesAnn Otol Rhinol Laryngol 2000 109(8):761-66. [Google Scholar]
[15]. Johnson Pergy L, Klein Morris N, Application of papanicolaou stain to paraffin sectionStain Technol 1956 5:223-25. [Google Scholar]
[16]. Elzay RP, A modification of Papanicolaou exfoliative cytology stain to demonstrate keratin in paraffin-block tissue sectionsOral Surg Oral Med Oral Pathol 1983 56:51-53. [Google Scholar]
[17]. Preethi S, Sivapathasundharam B, Will modified Papanicolaou stain be the new stain for keratin?Journal of Histotechnology 2015 38(1):9-13. [Google Scholar]
[18]. Rao RS, Patil S, Majumdar B, Oswal RG, Comparison of special stains for keratin with routine hematoxylin and eosin stainJ Int Oral Health 2015 7(3):1-5. [Google Scholar]