Healthy Mother and Child (MCH) are important by-products of processes leading to development of any nation. Their health being monitored globally as markers of human development. It is a hard truth that India is home to largest numbers of malnourished children and is also the largest contributor to global infant and maternal mortality indicators [1,2]. Deluge of respiratory, diarrheal and other communicable diseases have made matters worse and unless the underlying determinants like, hunger, inaccessibility to quality health care services and unhealthy environment are dealt properly, situation won’t improve [3,4].
In 1975, Indian government initiated Integrated Child Development Service (ICDS) scheme to check maternal and child malnutrition and ill-health and it emerged as one of the world’s largest program for early childhood development [5]. Under the program, a trained female known as Anganwadi (Courtyard) Worker (AWW) along with an assistant (Anganwadi helper-AWH), worked in an Anganwadi Centre (AWC), each catering to fixed numbers of community members based on certain predetermined criteria. Together, they were responsible for bridging the service utilization gap between the vulnerable groups and healthcare system. The main objective of the program was to improve the nutrition and health status of the children below 6 years, by providing supplementary nutrition & immunization; laying the foundation for proper psychological, physical and social development of the child through preschool education; reducing the incidence of disease burden through proper referral; and enhancing the capacity of mothers to take care of themselves as well as their children through health education [6].
Although, four decades have passed since the launch of this program, till today, every third indian children below five years suffer from malnutrition [3]. Equal number of children between 12-23 months remains unvaccinated [7]. The mortality among neonates (28/1000 live births), infants (40/1000 live births), under five year children (49/1000 live births) and mothers (178/100000 live births) does not seem to be reducing [8,9]. Beyond doubt, ICDS has not delivered the desired results. The underlying issues could be related to infrastructural problems, lack of utilisation due to poor awareness about the program, faulty supervision and monitoring mechanisms, corruption in food supplies etc., [10,11].
Success of any program depends on proper planning and its effective implementation. ICDS program though well conceptualized definitely has some implementation issues. Most of these revolve around the AWW and the AWC itself, a factor that assumes a pivotal place in the scheme of things due to its close and continuous proximity to the beneficiaries.
Odisha, one of the eastern states in India has poor maternal and child indicators. Under six malnutrition is 50.5% [12]. It has the highest neonatal mortality rate (37/1000 live births), second worst infant mortality (51/1000 live births) and under five mortality rates (66/1000 live births) [8]. Maternal mortality ratio is 235/100,000 live birth [9]. ICDS as a maternal and child health program is functioning in state of Odisha since its inception. This study was carried out with the aim to assess operational aspects of ICDS program in terms of its implementation and utilization in a rural area of Odisha, in Eastern India.
Materials and Methods
Odisha has 30 districts and 310 blocks. One of the block named Tangi is our field practice area and situated in Khordha district. The block is divided into six sectors each with a primary health centre. The current study was a cross-sectional study carried out from July 2014 to February 2015 in Bhusandapur sector, one of the most crowded sectors of Tangi with 5gram-panchayats (local self-government organization), 56 villages and an estimated population of around 57,000. As per ICDS norm, there should be one AWC for population of every 800 people or less. There were 50 AWCs for 7,400 (under six children) in Bhusandapur sector with estimated deficiency of 22 AWCs as per norms (i.e., 30% gap in infrastructure).
Out of 5gram-panchayats, we selected 3gram-panchayats using convenient sampling method. The selected gram-panchayats had 36 AWCs which constituted our sample. Data was captured using a semi-structured questionnaire and checklist for facility survey developed in the department.
Data Collection and Study Procedures
Information was gathered on variables related to three domains, manpower resource, material resource and functional aspects of the AWC either through interviews of AWWs or by performing observations within the AWC.
We studied the socio-demographic profile of AWW (i.e., manpower resource). Here data was gathered on their age, educational qualification, caste, residential status in the village they worked, and years of work experience. Under material resource we collected information on the status of building, ownership aspects, accessibility to beneficiaries and provision of water, toilet, electricity, and availability of dedicated cooking space. The functional aspects of AWC were determined by analysing the gap between expected and actual enrolment of the beneficiaries (children under six, and pregnant and lactating mothers) from the registers of previous one year, by physically checking the availability of tools for promoting physical and psychological development of the beneficiary children like pre-school education kit, growth charts, weighing machines, and utensils for supplementary nutrition etc.
AWWs were also asked (qualitative inquiry) about the various components of their day to day activities; problems faced in executing their duties that could be related to infrastructure issues, logistics, human resource constraints; their perspective about different stakeholders in the program; and their suggestions for further improvement.
Statistical Analysis
Data were entered and analysed in Microsoft excel (2007). The quantitative variables were summarized using median and inter-quartile range and the categorical variables were expressed in terms of numbers and percentages. The responses (qualitative data) obtained during the interview were recorded in vernacular language, translated to english and presented in the boxes in narrative form.
Ethical Considerations
No ethical approval was sought specially for the study as the data was part of routine monitoring and met the criteria of operational improvement in health services in the field practice area of the Institute. Verbal informed consent was taken from all the participants before the interview and the confidentiality of the data was maintained within the department. Govt. of Odisha has given permission to the institute to take Tangi block as the field practice area. Moreover, it is a cross-sectional study and data was collected through interviews. We have taken utmost care to anonymize the data and to maintain the confidentiality.
Results
The data was available for 36 AWCs. Findings of the study are summarized under three headings as mentioned below:
Manpower Resource
More than 80% of the AWCs had both AWW and AWH. The median age of AWWs was 33.5 years (Interquartile range 29 years, 39 years). All the AWWs had more than 8 years of schooling. In fact, 55% were either graduates or postgraduates. Most of them belonged to general caste (77.8%) and their residence was within 3 kilometres (88.9%) of the AWC. The median years of job experience was 6.5 years (Interquartile range 5 years, 15 years).
Material Resource
A 83.3% of AWCs were pucca houses (made of impervious walls and roof) in nature. Almost one tenth of the total studied AWCs had self-owned building and the rest were functioning in temporary arrangements made either in nearby government schools/office buildings (72.2%), in temple premises (11.1%), or rented houses (5.6%). At some places upto three AWCs operated in the same school premises. Almost 85% of the AWCs were situated within the same village. It is mandatory for every AWW to provide freshly cooked supplementary meals to the beneficiaries. However, only 16.7% AWCs had dedicated cooking space available for the same. In most other centres, cooking activities took place within the same premises that exposed children to severe indoor air pollution as seen in [Table/Fig-1]. Almost 90% of the AWCs did not have adequate provision of water, toilet and electricity [Table/Fig-2].
Smoke coming from the cooking area with children playing around in an AWC in Jhatinuagaon village, Bhusandapur, Tangi, Odisha 2014-15.

Infrastructural facility present at Anganwadi centres (N=36)
| Variables | Number | Percentages |
|---|
| Building StatusGovt. School & officesOwn buildingTemple premisesRented | 26040402 | 72.211.111.15.6 |
| Type of BuildingPuccaMixed | 3006 | 83.316.7 |
| Situation of AWCsWithin the villageOutside of village | 3006 | 83.316.7 |
| Water SupplyAbsentPresent | 3204 | 88.911.1 |
| Electric SupplyAbsentPresent | 3204 | 88.911.1 |
| Toilet FacilityAbsentPresent | 3402 | 94.45.6 |
| Separate Cooking SpaceAbsentPresent | 3006 | 83.316.7 |
Lack of own building forced the AWWs to organize their day to day activities like immunization, growth monitoring, cooking meals etc. in different temporary settings. This put extra burden on them for daily transfer of items like Pre-School Education (PSE) kits, registers, utensils, etc. required for these activities between their place of residence and centre. Scarcity of water at these sites was a major problem [Table/Fig-3]. There was an earmarked budget for the construction of AWCs. However, the site for its construction was left to be determined by the AWW. The villages were mostly overcrowded; therefore, most people had illegally occupied vacant government lands over generations. This led to conflicts while identifying suitable area for construction of new AWCs in those villages and the AWWs were helpless due to local pressure. [Table/Fig-3] summarizes key statements of interviewee and observation made by the interviewers during this study under material resource section.
Narrative comments of the participants with salient observation of the investigators related to material resources of AWCs.
| Narrative comments of participants | Salient observations pertaining to material resources of AWCs |
|---|
| “Nijaraanganwadighara nathibaru, kharahaubabarshahau mote panchayat office varanda re tikadabakupaduchi. Daily mote anaganwadirasabujinishagharakunabaaniba bi karibakupaduchi. Bahutasubidhahauchi”Translation: “Because of lack of own anganwadi building, I have to immunize the children in Panchayat office veranda irrespective of whether there is scorching heat or incessant rains. Daily I have to physically carry different items between AWC and my home. I face a lot of problems” (AWW-3, age 32)“Mote randhiba pain panigote kilometre dura ruanibakupaduchinahelekahakukahijogadakaribakupaduchi”Translation: “For cooking purposes I have to bring water myself from one kilometre distance or have to request others to arrange ”(AWW-2, age 35) | Centers operating in school premises had to wrap up their work before opening of the schools (i.e. by 9.30 AM), which provided hardly two hours to engage the children. Most AWCs didn’t have separate play area. Firewood/coal was used for cooking and lack of ventilation exacerbated the air pollution due to solid fuels in AWCs [Table/Fig-1] Unavailability of safe water in and around AWCs. Children at AWCs practiced open air defecation and urination in the vicinity of centers rendering the environment unsafe to them.
|
Functional Aspects of the AWC
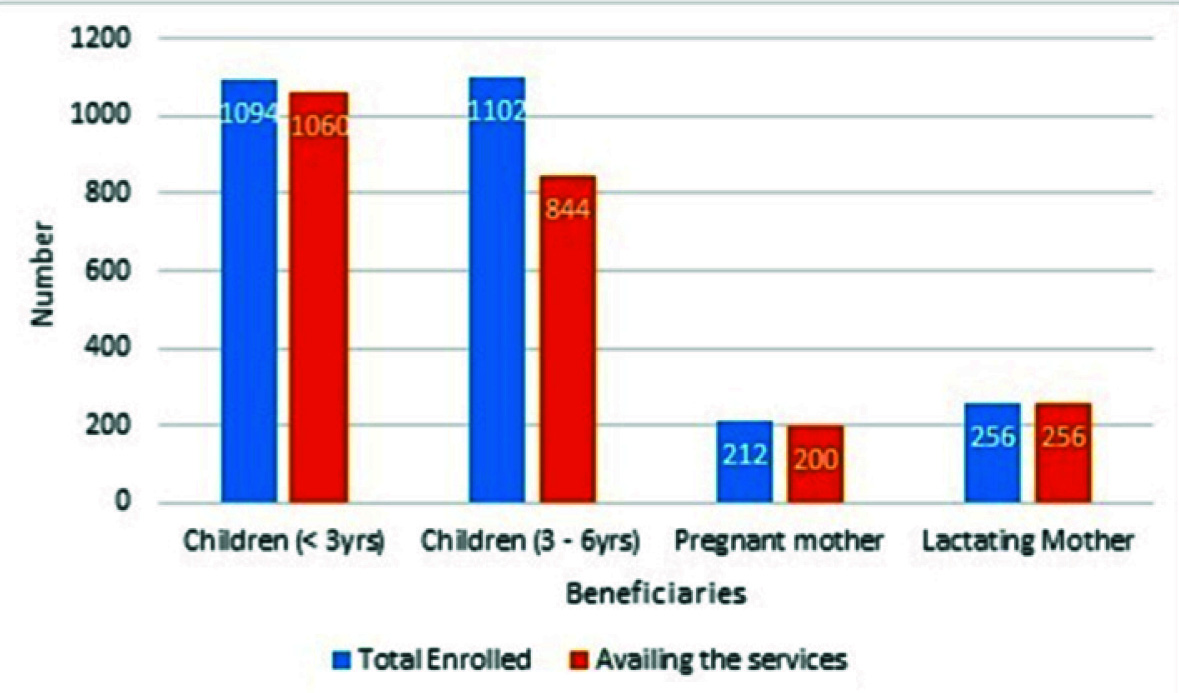
A 96.9% of children less than 3 years of age availed the services as compared to 76.6% of children between 3-6 years of age. Among others while all the lactating mother availed the services, only 94.8% of pregnant mothers availed the services [Table/Fig-4]. Those children who didn’t attend the AWCs, most preferred to attend private play schools. Reasons cited for this, was poor satisfaction with respect to quality of services provided to them. According to the AWCs, supplementary nutrition didn’t meet their demands and supply of only eight eggs per month was not at all acceptable [Table/Fig-5]. Utensils for cooking food weren’t available in 20% of the AWCs.
Percentage of beneficiaries availing services at AWC in Bhusandapur sector, Tangi, Odisha 2014-15.
Narrative comments of participants and salient observation of investigators related to functional aspect of AWCs.
| Narrative comments of participants | Salient observations of investigators |
|---|
| “Lokamanakaraanganwadiuparebharasanahikhaligariba pila asuchanti. Jahar paisa achise ta pila ku private nursery kupathauchi”Translation: “People do not have faith in the anganwadi. Only children of poor family come to centre and those who have money send their children to private nursery school” (AWW-14, age 38)Regarding low attendance of pregnant women one participant said “sarkargarbhabati ma manakusaptahakuditaandadauchanti se bi fix dina re. Semanekahuchantiditaanda pain daily kieasiba”Translation: Government provides two eggs per week to pregnant mothers that too in specific days. Why we should come for two eggs” (AWW-7, age 32)“Ojanamapiba machine sahitajoukapadadiajaichisegudakharap quality ra. Mote ta bahutdara lag eta uparepilankubaseibaku”Translation: “Cloths on the weighing machine (referring to Salter weighing scale) are of poor quality. I feel scared whenever I put babies for weighing” (AWW-10, age 34) | Lack of guidelines for preparing meals on different week days, has resulted in preparation of same type of food each day that could cause resentment among children. Infantometer and stadiometers were not available in any AWCs that could compromise the nutritional assessment of children and early detection of malnutrition. Some of the AWCs even shared the utensils for cooking purposes indicating lack of sufficient funds for their operation. The income generated after selling the packing material of food was used to purchase PSE kits. Each AWC was supplied with a color coded bag with Ready to Use Therapeutic Food (RUTF) for each beneficiary. Local self-help groups provided additional supplementary meals in the form of breakfast separately to these children and were funded under the same ICDS scheme
|
Besides, AWWs also acted as one of the nodal persons for conditional cash transfer under Mamata scheme under reproductive child health program to pregnant and lactating mothers (scheme) [13]. Irregular disbursement of funds under the Mamata scheme often resulted into lack of faith in AWWs which inadvertently also affected their performance in ICDS largely due to non-acceptance.
Under ICDS, preschool education is one of the vital service com-ponents and requires availability of a preschool education kit. This kit consists of picture charts, fruit models, kitchen sets, hollow ball, counting frames, animal toys etc., [14]. Nearly half of the AWCs didn’t have many of these items. All the AWCs lacked simple puzzle game or stacked rings or fun dough for mental stimulation and development of the children. The available kits were old and potentially unusable.
Though, growth charts and weighing scales were universally present, most AWWs didn’t know about zero correction and proper placement of children in the sling of weighing machines. The quality of these slings was also not up to the mark. All these have been captured in narrative statements in [Table/Fig-5]. As per the ICDS scheme, every AWW has to deliver certain services like preschool education, immunization, supplementary nutrition, health education and referral support. On repeated probing about various activities, most AWWs were able to remember their role and responsibilities in each of these service domains. The very fact that it did not come out spontaneously, raises doubt about its execution on regular basis.
It was also observed that AWW had to participate in various other community based activities of the State Government like Village Health Nutrition Days (VHND), monetary disbursements under the Mamata scheme, besides attending monthly meetings with ICDS beneficiaries and updating the demographic information of the village assigned to them. They also had to maintain number of registers like family survey register, immunization register, pregnant & lactating mothers register, birth & death register and growth monitoring registers. This was a paper based record and lacked uniformity in reporting across different AWCs. There was no electronic data gathering system available at these centers [15]. All this overburdened the AWW, who was left confused most of the times while prioritizing the jobs (service delivery, documentation, health promotion, liaising with ASHA etc.,) expected of them.
Nearly 90% AWWs had undergone induction training, but only half of them ever had any refresher training within the last three years [Table/Fig-6]. The reasons cited were lack of training facilities in their localities and their inability to attend trainings 60 kilometres away from their work place in the capital city of Bhubaneswar.
Training of AWWs along with job related problem faced by them.
| Variables | Numbers | Percentage |
|---|
| AWCs undergone induction trainingYesNo | 3303 | 91.68.4 |
| Refresher training in last 3 yrsYesNo | 1719 | 47.252.8 |
| Job related problems faced by AWCsLow salaryHeavy work loadLate disbursement of fundsLack of communication with supervisorsLack of training | 2816090816 | 77.744.425.022.244.4 |
Low salary, heavy work load, late disbursement of fund from gov-ernment and lack of communication with the supervisors etc., were some of the additional problems related to their job that affected their satisfaction levels.
Some of the innovative suggestions given by participants to improve performance of AWCs were provision of milk based products in the daily menu of AWCs, making uniforms mandatory for the children in all AWCs to improve the visibility of AWC and ICDS implementation in the community, introduction of skill based training for adolescent girls to boost their enrolment rates in the AWCs, and providing effective health education services at these centres.
Discussion
Under the ICDS program, AWC represents the grass root level facility which should be manned by one AWW and one assistant i.e., AWH [6]. At national level, nearly 90% AWCs were fully staffed as per the status report on ICDS scheme 2013 [16]. Previously published reports and studies indicated that the educational status of AWWs in Odisha was reportedly higher as compared to other states in India [10,17]. This finding had also reflected in our study. This could be one of the reasons, for better awareness among AWWs about their roles and responsibilities as envisioned under ICDS, and also for maintenance of different registers in our study site, irrespective of its completeness and unlike in other places across the country [18,19].
As per the guidelines issued by Ministry of Women and Child Development, Government of India, AWWs should be selected from the local community, and the selection process should reflect representation of all the sections of the society based on the prevailing caste distribution within the community. This is necessary to improve the accessibility of children of schedule castes and other weaker sections of the society to the centers [20]. Our study site indicated a fair selection of AWWs as per these norms.
Regular refresher and specific need based-training of involved manpower is vital to maintain quality of services rendered. Therefore, Govt. of India had sanctioned 5 billion rupees especially for training during the 11th five year plan for creation of new training centres. However, this vision doesn’t seem to have been translated into reality as per our findings and few other published studies [21,22].
Apart from performing routine duties within the ambit of ICDS, AWWs are forced to participate in other state run programs throughout the country [10,23,24]. Any deficiency in implementation of those programs would negatively impact the image of AWWs and implementation of the ICDS scheme in the bargain. Kishori Shakti Yojana and Sabala scheme focusing on adolescent girls were also planned to be implemented through ICDS infrastructure. However, the existing woes of the AWWs failed to generate any interest among the targeted beneficiaries [25].
AWWs are expected to carry out their routine activities through temporary makeshift arrangements. The scenario is not very different elsewhere in the country [10,26]. This could prove to be a demotivating factor to the workers as well as the beneficiaries [23]. Ministry of Women and Child Development recognized the importance of self-owned buildings for better service provision, in its annual report (2012-13) [11]. But, over last few years there appears to be a lack of political will as indicated by reduction (55%) in budgetary provision for the program both at the centre and state level in Odisha during the last two years [27].
In spite of existence of ICDS for many years, there is no palpable difference in terms of availability of basic facilities like electrification of centres, provision of toilets and safe water supply to the children and working staff across the country [10,23,28,29]. Use of alternate source of fuel in the form of firewood/coal adds to the health hazard of the children. Attendance in private play schools instead of AWCs in our study area reflected the dissatisfaction among parents. The reasons for this were poor quality of services, non-availability of play materials and infrastructural deficiencies. Similar results were obtained in previous studies [30,31].
A motivated, skilled and satisfied worker is essential for improving the quality of services. Lack of communication with supervisors, delay in release of salary, lack of training opportunities and non-recognition of long standing contribution breeds contempt and sense of unfairness among the AWWs which demotivates and results in sub optimal performance [10,17–19,22,24,32].
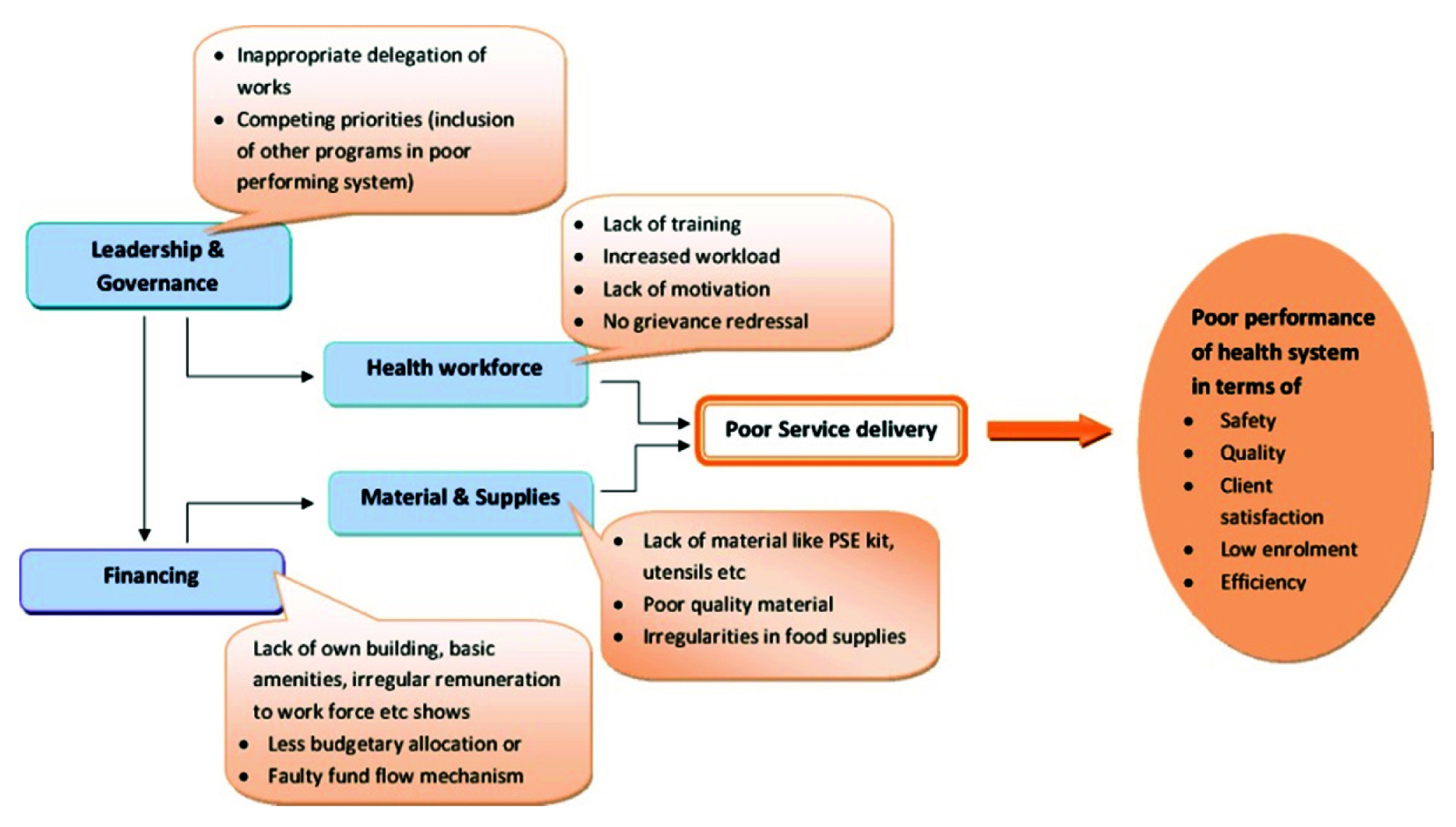
All these findings have been projected from the perspective of health systems analysis in [Table/Fig-7]. It shows how various factors interact with each other resulting into poor service delivery and negatively impact the goals of the program meant for betterment of maternal and child health. Strength of our study lies in combining different approaches of research to corroborate the findings and bring out a clearer picture into focus.
Using Health systems Framework to analyse status of ICDS implementation in Odisha, India.
In recent years, researchers have evaluated the ICDS program at different sites and suggested changes for better functioning of AWCs time to time, but the age old problems of infrastructure, logistics, lack of quality of services, lack of minimum amenities etc. are still persisting that require urgent attention of policy makers.
Limitation
First of all, the study was carried out in a field practice area and is not a true reflection of the performance of the programme at the state level. Secondly, we could not assess the supply chain management, perspectives of AWW supervisors, the policy makers and implementers at state level. However, we believe that it does expose key factors that affect the effective implementation of the scheme and the felt needs of its implementers at the grass root level.
Conclusion
Current study found out many issues regarding manpower, functionality and infrastructure of AWCs under ICDS program. Such issues warrants strengthening of grass root level facilities based on findings of regular needs assessment, effective monitoring and supervision. Involvement of the lowest level workers in stakeholder analysis for performance improvement, adequate supply of logistic, performance based incentives etc. may be some ways that could improve functioning ICDS and can help to achieve its intended goals.