Polycystic Ovarian Syndrome (PCOS) is the most common endocrinopathy and cause of infertility in women [1,2]. Its pathophysiology is complex and obesity and insulin play a major role in its pathophysiology. Anovulation is present in 60% of women with PCOS, and oligomenorrhea or secondary amenorrhea, diagnosed by laboratory and clinical evidence of androgen excess [3]. Hormone imbalances such as anovulation, and androgen excess disorders such as PCOS, adrenal hyperplasia, hyper prolactinemia, and thyroid function disorders are the most important causes of oligomenorrhea [4,5], seen when menstruation intervals are more than 35 days [6], or the total numbers of cycles are 5-7 a year [7]. Statistics report the prevalence of oligomenorrhea10-15% and in infertile women, 10-20%. In Iran, 14-26% prevalence has been reported [8]. Pathologies caused by oligomenorrhea such as infertility, low fertility, malignancies, cardiovascular diseases, diabetes mellitus, hirsutism and acne vulgaris result in problems regarding women’s general health and quality of life. Therefore, timely diagnosis and treatment of these disorders are of utmost importance [9,10].
Anovulation is one of the most important causes of oligomenorrhea in PCOS patients. Metformin is considered the first line treatment for ovulation disorders and infertility [2]. Serum insulin levels are high in these patients; Metformin decreases the insulin levels, LH, and androgen in the ovaries via gluconeogenesis inhibition in liver, glucose uptake stimulation and delay in digestive system glucose absorption; it causes ovulation and thus regulates the menstrual cycle [11,12]. Metformin side effects are nausea, diarrhea, and metallic taste in the mouth, weight loss, loss of appetite, B12 mal absorption, stomach ache, and bloating. It should be avoided in patients with liver, heart, or kidney disease, dehydration, diabetic coma, severe infection, and high-risk of lactic acidosis [2].
Herbal medicine in the treatment of a large number of patients has been traditionally prevalent, considering the side effects of chemical medication [13,14]. Agnugol is a herbal medicine used for treating menopausal disorders and hot flashes, menstrual disorders, secondary amenorrhea, uterine bleeding, PMS, headache, tachycardia, vertigo and mastalgia [15,16]. Agnugol and Vitagnus are the extract of Vitexagnus-castus (chaste tree). Each tablet contains 3.2-4.8 mg of chasteberry dry extract [15]. Studies show that chasteberry decreases the levels of serum prolactin by affecting dopamine receptors [17-19], leading to the stimulation of gonadotropic hormones, LH and FSH, and thus contributing to treatment of menstrual disorders [20].
Because of the effects of menstrual disorders on women’s physical and reproductive health, the side effects of chemical and hormonal medicines and the limitations in their administration, and the lack of studies on the effects of Agnugol on menstrual disorders in PCOS in comparison with those of Metformin, the present study set to compare the effects of Agnugol and Metformin on oligomenorrhea in PCOS patients in Women’s Care Unit of Fatemiyeh Hospital in Hamadan city, Iran, 2015.
Materials and Methods
This double-blind randomized clinical trial was conducted from March to September 2015 in female with PCOS attending to Fatemieh gynaecology clinic in Hamadan city, Iran.
Study was registered in the www.irct.ir with record: IRCT2015072623350N1 after approval from the Research Ethics Committee of Hamadan University of Medical Sciences, Hamadan, Iran. Written informed consent was received from all females.
Inclusion criteria for all women were as follows: Married, not pregnant, Age between 20-45 years, oligomenorrha- with PCOS based on criteria NIH (National Institutes of Health) contains little or anovulation, oligomenorrhea, or clinical evidence of hyperandrogenism and increased chemical LH/FSH ratio sonographic findings, no known physical or mental illness confirmed by psychiatric, non-hormonal drugs for the treatment of menstrual disorders in the past three months, no history of allergies to herbal medicines. Exclusion criteria were as follows: Use of contraceptive pills, Androgen-secreting tumors, high blood prolactin, decline to participant. According to calculations performed to find differences about 30% and pain reduction according to 80% power scale and significance level 0.05, 33 patients in each group were required which is justified the sample size of 60 subjects in this study [4].
The patients first visited a gynaecologist. Patients meeting the requirements of the study were randomly (permuted block randomization) divided into two groups, 60 participants in each group: Group A, patients taking Agnugol, and Group B, patients taking Metformin. The participants were informed that they would be randomly assigned to a group. They signed the informed consent form and filled in researcher-made demographic information forms and checklists. Afterwards, they went through a pre-intervention and three intervention phases in which they received medication. For Group A, the treatment consisted of oral administration of one Agnugol tablet (Isfahan Goldaru Pharmaceutical Laboratory) a day, throughout the cycle, even during menstruation, and for Group B, it consisted of oral administration of 500 mg of Metformin (Osvah Pharmaceutical Company), three times a day, throughout the cycle, even during menstruation. Patients in Group B were advised to take Metformin with meals to reduce its gastronomical side effects. Agnugol was prepared as packs of 100 coated tablets manufactured by Isfahan Goldaru Pharmaceutical Laboratory, each tablet containing 3.2-4.8 mg of chasteberry dry extract. The patients were asked to take one tablet a day after meal, during three phases of treatment (i.e., 3 months) nonstop, even during menstruation. Patients visited every month. At the end of all three phases, they filled in a researcher-made questionnaire and completed a checklist for changes in or regulation of menstrual cycles.
The validity of the Chek list was used of content validity method so that using the obtained resources and books and under the supervision of Faculty of Nursing and Midwifery Hamadan University of Medical Sciences, was approved, and then confirmed. To determine reliability, Cronbach’s alpha between 0.73/0.82. The results were then compared and statistically analysed. Also, the menstruation pattern was assessed during one cycle before and three cycles after the intervention. Data were analysed using IBM SPSS Statistics 21.0, descriptive statistics, chi-squared test, independent-sample t-test, and repeated measures ANOVA, p <0.05.
Results
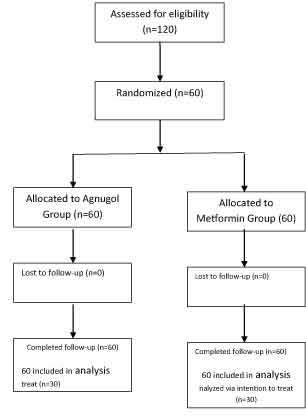
One hundred twenty women with PCOS and oligomenorrhea, aged 20-45, participated in the study. All participants had visited Women’s Care Unit of Fatemiyeh Hospital in Hamadan, met the study requirements, and were fully informed before taking part in the study [Table/Fig-1].
Flow of participants through the trial.
The study groups were homogenous; Kolmogorov-Smirnov test demonstrated no significant differences between the groups in terms of age, BMI, education, occupation, and parity (p> 0.05). The mean and SD of age was 39.45±4.60 for women taking Agnugol and 38.466±.84 for those taking Metformin.
Independent-samples t-test suggested that Agnugol and Metformin groups were not different regarding age, weight, height, BMI, and the number of pads used in menstrual cycles before intervention. Both groups were overweight. The average number of pads used in menstrual cycles was four for both groups [Table/Fig-2].
Baseline characteristics and clinical data of the study population.
| Characteristics | Agnogol Group | Metformin Group | p-value |
|---|
| Age (years) | 39.45(4.60) | 38.46(4.84) | 0.366 |
| Weight (Kg) | 72.38(6.55) | 71.16(4.92) | 0.252 |
| Heigth (Cm) | 162.66(5.51) | 160.50(2.61) | 0.217 |
| BMI (Kg/m2) | 28.1(5.24) | 28.4(6.41) | 0.233 |
| Education |
| Diploma | 43(71.7) | 47(78.3) | 0.305 |
| Advanced Diploma | 13(21.7) | 7(11.7) |
| License | 4(6.7) | 6(10) |
| Menstrual situation |
| Regular | 0(0) | 0(0) | - |
| Irregular | 60(100) | 60(100) |
| Exercises history |
| Yes | 67(55.83) | 61(50.83) | 0.246 |
| No | 53(44.16) | 59(49.16) |
Data for continuous variables is presented as mean (SD); Data for categorical variables is presented as frequency (percentage). p-value for the difference between groups.
Based on [Table/Fig-2], 80% of the Agnugol- and 71.7% of the Metformin-taking groups reported menstruation intervals of >45 days before the intervention. In the Agnugol- group, 65%, and in the Metformin-taking group, 63.3% of women reported the length of their cycles 3-7 [4] days prior to the intervention. Based on the chi-square test, there was no significant difference between the distributions of independent categorical variables.
Both groups showed a decreasing menstrual cycle interval from the beginning of the first to the end of the third month of drug administration. Intervals in the Agnugol group were 35.1±8.4, 31.38±6.13, and 28.83±1.85 at the end of the first, second, and third month respectively, showing a decrease in menstrual interval after 3 months of Agnugol consumption; in the Metformin group, the intervals were 34.7±7.26, 32.13±5.82, and 28.66±1.31 at the end of the first, second, and third month, respectively, showing a decrease in menstrual interval after 3 months of Metformin consumption [Table/Fig-3]. Also, the menstrual length increased after taking Agnugol and Metformin, from an average of 5 to 6 days. The average number of pads used during menstruation increased from seven at the end of the first month and to 11 and 12 at the end of the second and thirds months in both groups.
Scores of menstrual pattern before and after the intervention in the two groups.
| Menstrual pattern | Agnugol GroupN= 60 | Metformin GroupN= 60 | p-value (t-test) |
|---|
| Before the intervention (cycle 0) |
| Interval between cycle (day) | 40.96(1.35) | 38(1.35) | 0.413 |
| Duration of bleeding (day) | 3.66(.54) | 3.56(0.59) | 0.337 |
| The number of used pads | 5.65(2.46) | 5.65(2.17) | 0.994 |
| After the intervention (cycle 1) |
| Interval between cycle (day) | 35.1(8.4) | 34.7(7.26) | 0.781 |
| Duration of bleeding (day) | 5.26(1.2) | 5.45(1.26) | 0.424 |
| The number of used pads | 7.20(2.5) | 7.8(2.4) | 0.181 |
| After the intervention (cycle 2) |
| Interval between cycle (day) | 31.38(6.13) | 32.13(5.82) | 0.494 |
| Duration of bleeding (day) | 6.28(1.04) | 6.28(1.02) | 0.996 |
| The number of used pads | 10.5(3.35) | 10.16(2.8) | 0.557 |
| After the intervention (cycle 3) |
| Interval between cycle (day) | 28.83(1.85) | 28.66(1.31) | 0.571 |
| Duration of bleeding (day) | 6.66(.628) | 6.65(.633) | 0.885 |
| The number of used pads | 12.08(2.18) | 11.61(1.86) | 0.210 |
To assess the trend of change in these variables, repeated measures ANOVA was used, producing two tables of between-subject effects (comparison of variables between groups) [Table/Fig-4] and within-subject effects (comparison of groups based on the trend of variable changes over time) [Table/Fig-5]. Based on the between-subject results, the Agnugol- and Metformin groups were not significantly different in terms of menstruation length, cycle intervals, and the number of pads, p<0.005, i.e., the two drugs had similar effects on menstrual cycle regulation, menstruation length and the number of pads [Table/Fig-5].
Between-subject effects for variables in 2 groups of agnugol and metformin (women with PCOS).
| Variable | Source | Sum of Differences | df | Sum of Squares | F | Sig. |
|---|
| Cycle Interval | Group | .112 | 1 | .112 | .006 | .938 |
| Error | 2179.065 | 118 | 18.467 |
| Menstruation Length | Group | .093 | 1 | .093 | .179 | .673 |
| Error | 61.152 | 118 | .518 |
| No. of Pads | Group | .133 | 1 | .133 | .048 | .827 |
| Error | 329.863 | 118 | 2.795 |
Within-subject effects for variables in 2 groups of agnugol and metformin (women with PCOS).
| Variable | Source | Sum of Differences | df | Sum of Squares | F | Sig. |
|---|
| Cycle Interval | Time | 2257.339 | 2 | 1128.669 | 50.590 | .000 |
| Time * Group | 22.172 | 2 | 11.086 | .497 | .609 |
| Error | 5265.156 | 236 | 22.310 | | |
| Menstruation Length | Time | 107.450 | 2 | 53.725 | 72.669 | .000 |
| Time * Group | .739 | 2 | .369 | .500 | .607 |
| Error | 174.478 | 236 | .739 | | |
| No. of Pads | Time | 1170.022 | 2 | 585.011 | 103.673 | .000 |
| Time * Group | 20.267 | 2 | 10.133 | 1.796 | .168 |
| Error | 1331.711 | 236 | 5.643 | | |
Analysing within-subject effects of variables at time 1 (first month), time 2 (second month), and time 3 (third month) proved a significant interaction effect between the time variable and other variables in the groups (p<0.005). However, there was no significant time-group interaction effect (p<0.005). No significant time-group interaction effect means that the trend of changes over time is the same in both groups. The mean values show that the effect of time was in the direction of decreasing menstrual intervals and increasing menstrual length and number of pads in the second and third months [Table/Fig-6].
Agnugol and metformin side effects, after intervention (women with PCOS).
| Experience side effects |
|---|
| First month | Second month | Third month |
|---|
| Metformin Agnogul | Metformin Agnogul | Metformin Agnogul |
| SD±Mean SD±Mean | SD±Mean SD±Mean | SD±Mean SD±Mean |
| 11(18.33) 41(68.33) | 13(21.66) 46(76.66) | 12(20) 51(85) |
Eighty-seven percent of the Metformin-taking patients reported side effects such as loss of appetite, nausea, vomiting, bloating, excessive intestinal gas, diarrhea, fatigue, and stomach ache, while no such side effects were reported by the Agnugol-taking group. Therefore, Agnugol and Metformin were similarly effective on regulating menstrual cycles and increasing the menstrual length and the number of pads.
Discussion
PCOS is the most common endocrinopathy in women and the main reason for anovulation infertility, the most prevalent symptom of which is oligomenorrhea [1]. The present study was conducted to compare the effects of Agnugol and Metformin on oligomenorrhea in women with PCOS who visited Women’s Care Unit of Fatemiyeh Hospital in Hamadan city, Iran. Today, anovulation is present in 66% of PCOS patients, usually accompanied by oligomenorrhea or secondary amenorrhea [2].
In this study, 80% and 71.7% of Agnugol- and Metformin-taking patients, respectively, reported their menstrual intervals to be>45 days prior to the intervention. In the Agnugol-taking group, 65%, and in the Metformin-taking group, 63.3% of patients reported their menstruation length 3-7 [4] days before the treatment. The average number of pads used prior to the study was four in both groups, showing oligomenorrhea in the PCOS patients. After the treatment with Agnugol and Metformin, menstrual intervals decreased and the length of menstruation and the number of pads increased in both groups. Results revealed that the drugs had similar effects on the treatment of oligomenorrhea and menstrual cycle regulation and were not significantly different. In both groups, after 3 months of taking the drugs, oligomenorrhea was alleviated and menstrual cycles were regulated. The results are in line with those of Eltbogen et al., who conducted their study on 211 patients with menstrual disorders (amenorrhea, oligomenorrhea) [20]. The patients were divided into two groups of 105; the experimental group was administered chaste tree daily for 3 months, and the control group received placebo. Both groups were asked to report their menstrual events. Seventy-nine percent of the experimental group patients reported alleviation in amenorrhea and oligomenorrhea, and a significant difference was observed between the experimental and control groups (p<0.05). Eighty percent were interested in further treatment with chaste tree after the study. Four women reported side effects such as rash, skin redness, and nausea, by weeks 4 to 8. The results suggested that chaste tree is effective in the treatment of menstrual disorders (oligomenorrhea, amenorrhea) [20].
Agnugol is used for treatment of menopausal disorders and hot flashes, menstrual disorders, secondary amenorrhea, uterine bleeding, PMS, headache, tachycardia, vertigo and breast pain [15]. Agnugol and Vitagnus are both the extract of chaste tree [17]. Studies show that chasteberry reduces serum prolactin levels by affecting dopamine receptors, leading to the stimulation of gonadotropic hormones, LH, and FSH, which are crucial in treating menstrual disorders [21]. Also, Shahhosseini and Aghajaniin dictated that Agnugol is effective in treating dysmenorrhea and PMS [21,22]. Studies suggest that the flavonoid in chaste tree affects the pituitary gland directly, especially the LH-secreting section and elevates the progesterone levels and thus, alleviates hormone deficiency disorders such as menstrual disorders [24-27]. The Agnugol effect on the regulation of female hormones has been proven. Agnugol may decrease prolactin levels by binding to dopamine receptors and stopping the secretion of prolactin from the pituitary gland, approved by experiments on rats [25]. Moreover, in Dugan et al., 15 Agnugol drops, 3 times a day, could alleviated menstrual disorders in women [27].
The present study also showed the treating effects of Metformin on oligomenorrhea in line with the results of Al-Zubeidi et al., who investigated the effects of OCP pills and Metformin on PCOS. According to Al-Zubeidi et al., Metformin performed better than OCP in alleviating PCOS symptoms [28]. Also, other studies have proved that Metformin is very effective in the treatment of menstrual disorders, hyperprolactinemia, and amenorrhea, and in reducing androgen levels in PCOS patients [29-31].
With respect to the fact that Agnugol and Metforminhave similar effects in the treatment of oligomenorrhea in PCOS patients and since Agnugol is a herbal medicine and can be tolerated more easily than Metformin, Agnugol can be suggested as an alternative to Metformin in treating oligomenorrhea in PCOS patients. The merits of this study are its intervention design and the random assignment of participants to the groups and the fact that no similar study has been reported on the comparison of these two drugs.
Limitation
The limitations of this study are its small sample and no follow-up study to check the long-term effects of the drugs.
Conclusion
Agnugol and Metformin are similarly effective in the treatment of oligomenorrhea and menstrual cycle regulation in patients with PCOS. Since Metformin is a chemical drug with side effects, Agnugol can be presented as herbal alternative to treat oligomenorrhea.
Funding: The project has been funded by Research Deputy of Hamadan University of Medical Sciences, Hamadan, Iran.
Data for continuous variables is presented as mean (SD); Data for categorical variables is presented as frequency (percentage). p-value for the difference between groups.