Carbapenems are among the most potent antibiotics available for the treatment of serious infection caused by Gram-negative nosocomial pathogens. Alarmingly, in the last decade, reports of carbapenem resistant Enterobacteriaceae have been increasing steadily [1]. Most notably, in countries like the United States, Greece and Israel, Klebsiella Pneumoniae Carbapenemases (KPC) have been reported consistently over the last 15 years [2]. Carbapenem hydrolysing Metallo-enzymes VIM (Verona Integron–Encoded Metallo-β-Lactamase) and IMP (Imipenemase) and Oxacillinase-48 (OXA 48) type of carbapenemases have been frequently reported in Europe, Mediterranean and Asia [2,3]. With the identification of highly drug resistant New Delhi Metallo-β-Lactamase-1(NDM-1) producers in Britain, India, Pakistan and several other Asian countries [3] and the recent reports of co-production of NDM-1 with other carbapenemases, the treatment of such infections appears dismal [4].
Accurate detection of carbapenemases pose a significant challenge for clinical laboratories in resource constrained regions [5]. Identification of the resistant genes with certainty can be done by molecular techniques, though these may not be available in resource constrained laboratories [6], while screening by phenotypic methods like Modified Hodge Test (MHT) and Combined Disk Diffusion Test (CDT) using EDTA can be performed [5,6]. The MHT is proposed by the Clinical and Laboratory Standards Institute (CLSI 2014) for screening of carbapenemases for epidemiological purposes [6]. As per the CLSI 2015 and CLSI 2016 guidelines for carbapenem detection Carba NP test is recommended for carbapenemase detection [7,8]. Although, Carba NP test is highly sensitive and specific [9], however, it can be expensive for resource poor countries and might not be available easily in all the laboratories in India.
The overall sensitivity and specificity for detecting MBL and NDM by MHT is low 77% and 39% respectively [10]. This study was therefore undertaken to evaluate statistically, the use of MHT and to look for any significant improvement in performance of MHT by using MacConkey Agar (MCA) for detecting MBL and KPC, to genotypically confirm the presence of blaKPC and to find logical and economically viable phenotypic tests which can be used routinely for detection of carbapenemase production, till the Carba NP test becomes economical and easily available for all laboratories or more economical alternatives with comparable sensitivity and specificity become widely available.
Materials and Methods
A prospective laboratory based study was conducted in the Microbiology laboratory at Kasturba Medical College and Hospital Ambedkar Circle and the samples from KMC Hospital Ambedkar Circle and KMC Hospital Attavar Mangalore, from January 2014 to December 2015 were collected. Approval from the Kasturba Medical College Mangalore, Manipal University Institutional Scientific and Ethics Committee was obtained (IEC 09/13-171).
One hundred and fifty three ESBL positive isolates (as determined by CLSI 2014,15 CDT) [7,8] of clinically significant Klebsiella pneumoniae were collected from various clinical samples and subjected to carbapenem sensitivity testing by modified Kirby-Bauer disk diffusion using the following antibiotic disks: Imipenem (10 μg), Meropenem (10μg) and Ertapenem (10μg) (Becton Dickinson, Sparks, MD, USA) [7]. K.pneumoniae ATTC© 700603 was used, as per the CLSI 2014 and CLSI 2015 [7,8]. Detection of AmpC production by Cefoxitin three dimensional disk test was performed for isolates with disk diffusion zones of <18mm for Cefoxitin. Amp C detection was done so as to rule out false positive MHT due to CTX- M type of ESBL and AmpC hyper production [11].
Isolates resistant to either Imipenem, Meropenem, or Ertapenem by Kirby-Bauer disk diffusion as per the interpretive criteria of CLSI 2014 [7] i.e., Ertapenem (10μg) ≤18, Imipenem/Meropenem (10μg) ≤19, were subjected to MHT on MHA and MCA and also to CDT using Imipenem and Imipenem with EDTA for carbapenemase detection [12]. All the isolates were then subjected to PCR for detection of blaKPC.
MHT on Muller Hinton Agar
MHT on Muller Hinton Agar was performed as described by CLSI 2014 [7].
MHT using Mac Conkey agar
Lawn culture of McFarland 0.5 normal suspension of E. coli, ATCC 25922, done on MCA plate, followed by placement of a 10 μg Ertapenem disk in the centre of the test area. Using a 10 μl loop, 3-4 colonies of test organism grown overnight on blood agar plates were picked and streaked in a straight line from the edge of the disk to the edge of the plate and incubated overnight at 35°C. After 16 to 24 hours of incubation, the plate was examined for a clover leaf-shaped indentation at the intersection of the test organism and the E.coli ATCC 25922 within the zone of inhibition [Table/Fig-1].
MHT done on MacConkey Agar and on Muller Hinton agar. The arrow indicates indentation indicating a positive test result.

The CLSI (2014-16) recommends a 1:10 dilution of McFarland 0.5 normal turbidity suspension organism for detection of KPC β-lactamase, but dilution was not performed in this modification of the MHT [11]. Enhanced growth was inferred as positive for carbapenemase production while no enhancement as negative for carbapenemase. The presence of a cloverleaf-shaped indentation was considered as MHT positive [7–9,11].
Detection of MBL production by Combined disk diffusion using Imipenem (10 μg) and Imipenem with EDTA. A 10 μg 0.5 M EDTA (750μg) trisodium salt (Merck India Laboratories) was put on Imipenem disk and difference of zone size ≥ 7 mm was taken as MBL positive [5,12,13] [Table/Fig-2].
Combined Disk Test for detection of Metallo-Beta-Lactamase Production.

Detection of blaKPC by PCR
DNA extraction was performed from well-isolated colonies grown on sheep blood agar plates following overnight incubation by boiling method [14]. The resistance genes blaKPC was amplified by Polymerase Chain Reaction (PCR). Universal primers for blaKPC family, Uni-KPC (PCR Primers from Sigma Aldrich Chemicals Pvt. Ltd Bangalore) F (5′-ATGTCACTGTATCGCCGTCT-3′) R (5′-TTACTGCCCGTTGACGCCC-3′) 882 kbp [15].
Lysates derived from Escherichia coli ATCC 25922 and blaKPC-carrying K.pneumoniae strain BAA-1705 were used as negative and positive controls, respectively, in each PCR. Amplified products were detected by gel electrophoresis using 1% agarose and stained by ethidium bromide.
Statistical Analysis
Chi-square test with Fisher’s-exact was used to compare MHT on MHA with the modification of MHT on MCA. Level of significance for this study was 5% (p-value <0.05 was taken as significant). SPSS version 16.0 was used for statistical analysis. As there is no gold standard test and the new test done is a modification of the existing test, Mc Nemar test is not used.
Results
A total of 54 isolates were carbapenem resistant by Modified Kirby-Bauer disk diffusion. Among these 79.6% (43/54) isolates were sensitive to Imipenem, while only 33.3% (18/54) isolates were sensitive to Meropenem. A 7.5% (4/54) isolates were sensitive to Ertapenem. Resistance to all three Carbapenems was seen in 18% (10/54) isolates.
Out of 54 isolates, 13 isolates were positive for conventional MHT (method as described by CLSI). When MHT was done on Mac Conkey agar 10 more isolates gave positive result, thus the total number of MHT positive isolates (MA and MCA) was 23. A total of 31 isolates were MHT negative. A total of 29 isolates (53%) out of the 54 were found to be Amp-C test positive i.e., ESBL + Amp-C co-producers. When CDT was done using Imipenem and Imipenem with EDTA, 23 out of 54 were MBL producers. Only 5 out of the 23 MBL producing isolates could be detected by the conventional MHT, while the MHT on MCA detected 11 isolates (including the ones detected in conventional MHT). The remaining 12 MBL positives (by CDT) were missed by both conventional MHT and that done using Mac Conkey. Hence, although there was a considerable improvement in MBL detection when MHT was done on MCA, it could still not identify 52% of the MBL producers (12 of the 23) [Table/Fig-3,4 and 5].
Total carbapenemases detected by Phenotypic tests (MHT, CDT) and Genotypic Tests (blaKPC) (n= 54)., NA: Not Applicable/Not performed in this study.
| Carbape-nemases | Combined disk test Positive | MHT positive on Muller Hinton | MHT on Mac Conkey’s | PCR positive | Phenotypic test Negative |
|---|
| MBL | 23 | 5 | 11 | NA* | 31 |
| KPC | NA | 2 | 2 | 2 | |
| Type of Carbapenemase Detected (By MBL Combined Disc Test and blaKPC PCR) | |
|---|
| MHT on Muller Hinton Agar | | Positive | Negative | |
| Positive | 10 (40%) | 3(10.3%) | 13(24.1%) |
| Negative | 15(60%) | 26 (89.7%) | 41(75.9%) |
| Total | | 25(100%) | 29 (100%) | 54(100%) |
| Type of Carbapenemase Detected(MBL Combined disk test and blaKPC PCR) | |
|---|
| MHT on Mac Conkey Agar | | Positive | Negative | |
| Positive | 16 (64%) | 7 (24.1%) | 23(42.6%) |
| Negative | 9 (36%) | 22 (75.9%) | 31(54.4%) |
| Total | | 25 (100%) | 29 (100%) | 54(100%) |
For Carbapenemase production, MHT done on MHA had a sensitivity of 40.0%, specificity of 89.7%, Positive Predictive Value (PPV) is 10/13 = 76.92% (probability of test showing positive will be carbapenemase producer). Negative Predictive Value (NPV) is 26/41 =63.41% (negative test will rule out carbapenemase producer). Sensitivity of MHT on MCA for detecting carbapenemase production was 64.0%, specificity 75.9%. PPV 16/23 is 69.56%. NPV 22/31 is 70.96% [Table/Fig-4,5].
Molecular analysis for presence of blaKPC
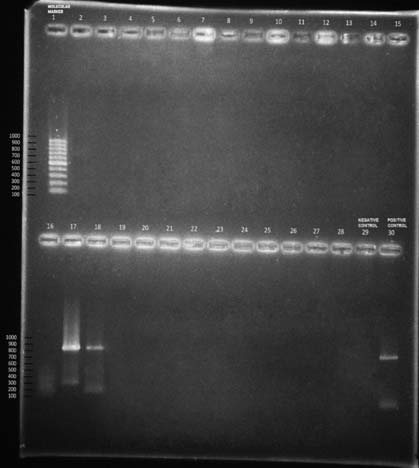
Two isolates tested positive for blaKPC [Table/Fig-6]. Both these isolates were positive for MHT done on MHA as well as on MCA. Total carbapenemase detected by phenotypic and genotypic tests is 25 i.e. 23 MBL and 2 KPC [Table/Fig-3].
Gel picture showing amplified products of BLAKPC gene.
Lane 1: Molecular Marker/ DNA ladder (100 bp)
Lane 17 and 18: Test Positive for BLAKPC at 882 bp
Lane 29: Negative Control
Lane 30: Positive Control
Discussion
Using modified Kirby-Bauer disk diffusion 54 Klebsiella pneumoniae isolates were carbapenem resistant. Among these 79.6% (43) isolates were sensitive to Imipenem, while only 33.3% (18) isolates were sensitive to Meropenem. A 7.5% (4) isolates were sensitive to Ertapenem.
We observed that proportion of carbapenem resistance is on the rise. In our study 35.2% of the total isolates were carbapenem resistant out of which of blaKPC was 3.7% i.e., 2 of the total 54 carbapenem resistant isolates. Gupta et al., from the All India Institute of Medical Sciences, New Delhi in 2006 found that resistance to meropenem was 6.9% [16]. Deshmukh et al., observed that out of 638 isolates of Gram negative bacilli, 21 (3.39%) isolates were carbapenem resistant out of which 18(85%) isolates showed MBL production [17]. The total number of isolates showing KPC carbapenemase was 2 isolates i.e., only 0.3%. Parveen M, Harish BN and Parija SC from a tertiary care hospital in Pondicherry found that out of 134 clinical isolates of Klebsiella, 43.6% percent isolates were resistant to meropenem, 32% to imipenem, 20.3% to ertapenem by disk diffusion [18].
CLSI 2014 and CLSI 2015 recommend the use of MHT for the detection of carbapenemase production as it is highly sensitive and fairly specific test to detect KPC type of carbapenemases [7,8]. We performed MHT (both conventional and modification) on MCA, CDT and PCR for all these 54 isolates which were carbapenem resistant by Modified Kirby-Bauer disk diffusion. The modification of MHT on MCA is a better test for detection of carbapenem resistance as it allowed detection of 23 isolates, while the conventional MHT detected only 13 isolates out of the 54 isolates tested. All isolates detected by the conventional MHT were also detected by the MHT on MCA. Therefore, a significant improvement in the results by use of MCA was observed (p-value <0.01) [Table/Fig-7]. Improved performance can be due to the increased release of periplasmic enzymes caused by the inhibitory substances like bile compounds included in MCA [13,19].
Comparison of MHT done on Muller Hinton’s agar was compared with MHT on Mac Conkey’s agar. As one of the cells has value of less than 5, fishers-exact test p-value is calculated.
| MHT Muller Hinton agar | Total | p-value |
|---|
| | Positive | Negative | | |
| MHT Mac Conkey’s agar | Positive | 16 | 7 | 23 | <0.001 |
| Negative | 0 | 31 | 31 |
| Total | 16 | 38 | 54 |
Now, to find the other possible enzymatic mechanism of carbapenem resistance (like MBL) CDT using Imipenem and Imipenem plus EDTA was done. We found that 23 out of 54 isolates were MBL producers, by CDT.
For detection of MBL activity, we found that the MHT modification done on Mac Conkey had a better sensitivity (64% as compared to 40% of the conventional MHT). Albeit, the overall sensitivity of MHT to detect MBL is poor, as only 11 out of the 23 MBL producers could be detected.
Lee et al., studied use of MCA for MHT in 18 isolates (confirmed Gram Negative bacilli producing MBL) and calculated the mean distortions of the inhibition zones obtained ranged from 2.7mm to 7.2mm depending on the test conditions, and in general the distortions were larger and more distinct with MCA. When the results were analyzed separately according to enzyme type, the mean distortions observed on MCA and MHA were 4.9mm and 3.7mm, respectively, for 11 MBL-producing isolates, concluding that MHT done on MCA gives better results [13]. We found that the results of MHT on Mac Conkey were more pronounced and the clover leaf indentation was appreciated better and the strains missed by CLSI MHT were detected by using the same. In a recent study, published in March 2015, Kim, park and Sung et al., also found that MHT done using MCA and use of Ertapenem disk improved the sensitivity of MHT to detect carbapenemases like the NDM [19].
The MHT can produce false positive results. Isolates producing CTX-M-type ESBLs or increased amounts of AmpC beta–lactamases can lead to false-positive results [20]. On the contrary, false-negative results can also occur, with isolates producing MBL and NDM or other enzymes exhibiting weak carbapenemase activity [19–21]. We found that among the 23 MHT positive, the presence of blaKPC gene was confirmed by PCR in 2 isolates, and 11 isolates were MBL positive by CDT. Ten MHT positives were neither MBL nor KPC. We observed that 7 out of these were AmpC and ESBL co-producers, which might have resulted in a false positive, while the mechanism for the remaining 3 MHT positives could not be detected. The positive result might be due to hyper production of ESBL (false positive) or due to other carbapenemases (e.g., OXA carbapenemases) [20,21].
A study done by Shanthi et al., states that OXA-48 may not be a major mechanism of carbapenem resistance in Enterobacteriaceae [22], thus hyper production of ESBL, porin loss and efflux pumps can be the other important contributing factors leading to carbapenem resistance. Both the PCR confirmed blaKPC isolates were picked up by MHT proving that MHT is highly sensitive (100%) phenotypic test for detection of KPC. PCR is the gold standard for its identification in clinical microbiology laboratory [22]. We recommend the use of MCA as an alternative to conventional MHT, as it remains as economical as the conventional MHT, yielding better results, with an increased sensitivity for detecting MBL group of carbapenemases. However, the MHT cannot be used as the sole method for the detection of carbapenemase positive Enterobacteriaceae and we suggest concomitant use of phenotypic tests for detection of MBL and NDM type of carbapenemases. Newer phenotypic tests for carbapenemase detection are emerging as replacements for MHT. But these tests are not easily available and can be expensive. Thus, MHT on Mac Conkey is a better screening test than the MHT recommended by CLSI 2014, 2015, since it can also be used for detection of MBL.
Limitation
Molecular analysis of other enzymatic mechanisms of carbapenem resistance like MBL, NDM-1 and OXA would have added more value to the present study.
Conclusion
Overall, the findings of our study indicate that there is an alarming rise in the proportion of carbapenem resistant Klebsiella isolates. The prevalence of KPC gene i.e., blaKPC in carbapenem resistant isolates from our geographical area (South Western India) seems to be very less and most isolates that show carbapenem resistance owing to carbapenemases of either MBL or NDM type or due to hyper production and co-production of AmpC and ESBL and/or due to porin loss and efflux. In resource constrained laboratories, where newer phenotypic tests and genotypic detection is not routinely done for the isolates resistant to carbapenem by disk diffusion, performing the MHT on MCA (for KPC and MBL detection) and the combined disk test using Imipenem and Imipenem-EDTA (for MBL detection) along with routine ESBL and Amp-C detection seems to be logical and economically viable method for detection of carbapenemase production for epidemiological purposes.