Dengue is an arthropod borne viral disease caused by Flavivirus. It is one of the 18 neglected tropical diseases stated in WHO report [1] with increasing prevalence in tropical and sub-tropical regions. Though dengue has global distribution, South-East Asian region and Western Pacific region contributes to 75% of the total disease burden [2]. Dengue was first reported in Chinese Medical Encyclopedia from Chin Dynasty (265-420 AD) [3]. There are many descriptions in the literature regarding the epidemics due to dengue in 17th century but the major epidemics were reported between 1779-1780 in Asia, Africa and North America simultaneously, after that infrequent epidemics were reported till 1940 and subsequently the prevalence kept on increasing [4,5].
Dengue has four serotypes DEN1, DEN2, DEN3, DEN4, well known for more than 50 years. A fifth serotype DEN5 was also reported few years back in 2013, from the serum samples collected during 2007 dengue outbreak in Malaysia [6]. These serotypes differ genetically and therefore, infection with one serotype does not confer immunity against other serotypes.
The first clinical case report of dengue was from Philadelphia, by Berjanin Rush, who coined the term “Break Bone fever” because of the symptoms of myalgia and arthralgia [7]. In India, dengue was first reported in 1946, DENV-1 was first reported in 1956 at Vellore, DENV-2 in 1956, DENV-3 in 1965 and DENV-4 in 1964 [7,8]. Subsequently several outbreaks were reported with different serotypes. In latest outbreaks reports, prevalence of almost all the serotypes is reported simultaneously [7].
Despite genetic variations, each of the dengue serotypes results in the same disease and range of clinical symptoms. The present study was planned to look for the the seroprevalence and various epidemiological factors that affected the dengue virus infection in our region.
Materials and Methods
The present retrospective study was conducted at Department of Microbiology, Government Medical College Hospital, Chandigarh during a period of six years from January 2010 to December 2015. Blood samples were collected from the patients who were clinically suspected to be suffering from dengue infection according to WHO definition [3] both in outpatient department and indoor every year.
Five mililitre blood sample was obtained by venepuncture from each suspected patient under strict aseptic precautions and the serum was separated by standard methods. Serum samples were tested immediately for dengue IgM antibodies/ NS1Ag to diagnose dengue virus infection. If not possible to put up immediately, the sera were stored at -20oC till testing. Sera exhibiting haemolysis, lipaemia and turbidity were rejected.
All the samples were processed for the presence of dengue IgM antibodies and/or NS1Ag by PanBio MAC ELISA (μ capture) and NS1Ag ELISA, supplied by Inverness Medical Innovations Pvt., Ltd, Australia. The test was performed as per the instructions of the manufacturer. Four thousand four hundred and eighty six (4486) samples were tested for NS1Ag and 6288 samples were put up for dengue IgM anti-body testing. Sample positive for either of them was considered positive as per WHO criteria [3]. Combination of serology tests (both NS1Ag and IgM on same serum sample) was done when needed by clinician to increase the accuracy of dengue diagnosis in patients presenting at various stages of illness.
Results
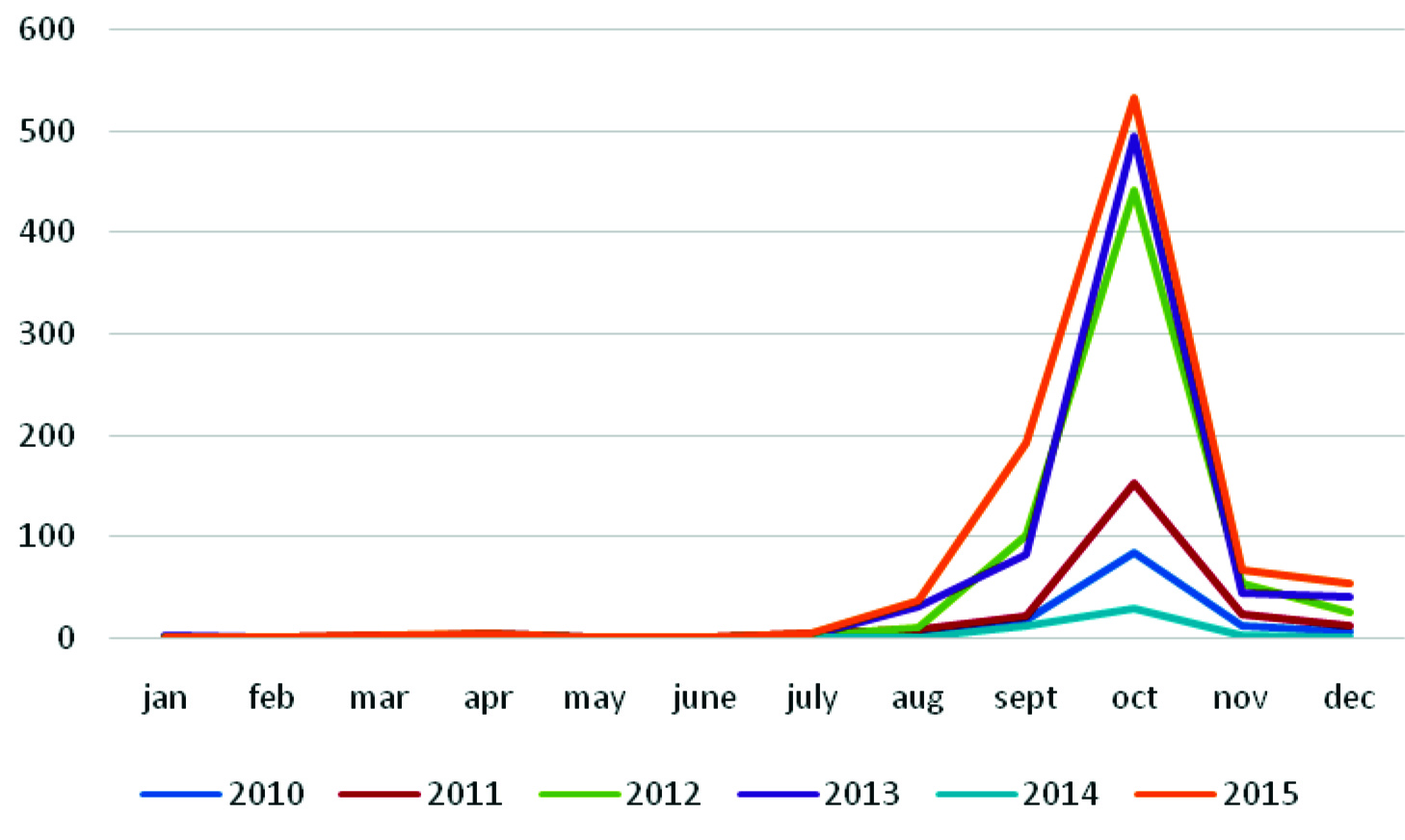
Over the period of six years (2010 - 2015), a total of 10,774 samples were processed. Among them 2,449 (22.7%) samples were positive for dengue. Dengue was endemically prevalent in the region in all the years (2010-2015) [Table/Fig-1]. Positivity ranged from 24-27% in this six years data, except in 2014 when the positive cases were markedly less i.e., 3.45%. Positivity showed marked seasonal variation, rarely 0-2 cases were seen from the month of January to July every year. Infection started in the post monsoon season and positive cases peaked in October (>70%) and tapered till December every year [Table/Fig-2].
Seroprevalence of dengue virus infection over the six year period 522 samples over a six year period were positive for both IgM antibodies and NS1Ag.
| Year | No. Positive/total number ofsamples (%) | NS1Ag positive/total number put up | IgM positive/totalnumber put up |
|---|
| 2010 | 119/448 (26.5) | – | 119/448 |
| 2011 | 207/849 (24.4) | 128/405 | 157/444 |
| 2012 | 493/1915(25.7) | 212/800 | 374/1115 |
| 2013 | 698/2931 (23.8) | 414/1261 | 395/1670 |
| 2014 | 42/1215 (3.45) | 14/212 | 34/1003 |
| 2015 | 890/3416 (26.0) | 551/1808 | 526/1608 |
| Total | 2449/10774 (22.7) | 1319/4486 | 1652/6288 |
Month wise distribution of dengue cases over six year period.
A total of 29.4% (1319/4486) samples were positive for NS1Ag and 26.3% (1652/6288) were positive for dengue IgM antibodies. Out of total positive samples, 522 samples were positive for both NS1Ag and IgM antibodies.
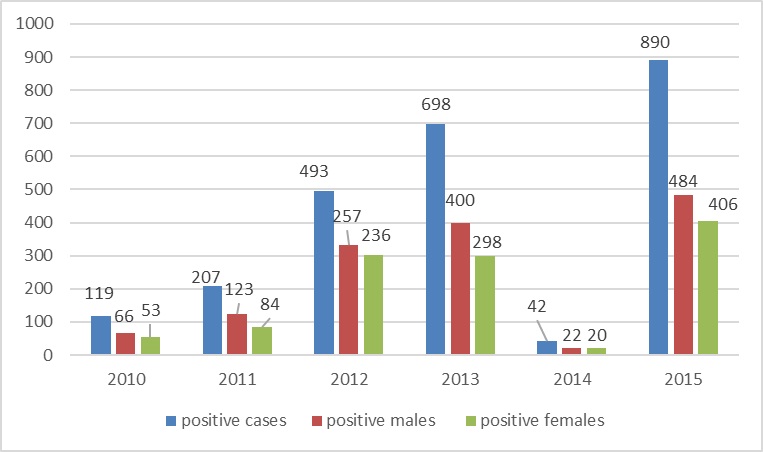
The adult age group (16-45 years) showed maximum positivity (83.3%) with (35.7%) positive in the 16-30 year age group and 47.6% positive in the age group of 31-45 years. Least infection was seen in paediatric age group (2.8%), with 9.2% persons affected in 46-60 years and 5.01% in elderly (> 60 year) age group. Males 1352 (55.2%) were more positive for the disease as compared to females 1097 (44.7%) [Table/Fig-3].
Distribution of dengue cases among male and females.
Discussion
The endemicity of dengue is spreading and has witnessed a 30-fold increase with rapid expansion to new countries and in the present decade, from urban to rural settings. During the present study period, a total of 22.7% of the samples were serologically positive for dengue infection. Considering year-wise positivity, the infection was least reported in 2014, only 3.45% of cases and maximum in 2010 (26.5%) and 2015(26.0%). This variation can be attributed to the monsoon trend during these years in Chandigarh, monsoon was reported maximum in 2010, 2015 (> 1000mm) and minimum in 2014 (< 400mm) [11]. According to National Vector Borne Disease Control Program (NVBDCP) data, adjacent states like Punjab, Haryana and Delhi has also reported the same pattern of dengue infection [12]. For seasonal variation, month-wise data was analysed and it was observed that >70% of the cases occurred in the month of October i.e., post-monsoon season. This post-monsoon rise in the disease has also reported in literature which in turn is due to the favourable temperature and humidity conditions for the mosquito to breed [2,3,8,13,14]. Various post-monsoon environmental factors like man made water stagnation sources (collection of water in open scrape yards in tyres, disposable bottles and other solid waste), labour colonies and low-lying areas without proper drainage system, stagnant water in open containers, aquatic flowering plants containers and coolers provide conducible environment for mosquito breeding. Therefore, this post-monsoon rise can be checked by timely implementation of the control measures.
Out of 2449 positive samples, 1319 samples were positive for NS1Ag and 1652 for dengue IgM antibodies. Both the tests have their own importance in diagnostics. NS1 antigen is a highly conserved glycoprotein which is abundant in the serum of the patients during early stages of dengue infection (from day 0 to day 9) and directly correlates with viremia. Thus, it is an easy, fast and feasible alternative to real time, Reverse Transcriptase Polymerase Chain Reaction (RT- PCR) in developing countries, with simple laboratory set up saving cost, time and labour [15]. Dengue IgM antibodies start appearing by 4-5 days but peak at 2 weeks time. IgM antibodies show cross reactivity with other flavivirus infections so gives false positive results [16]. False-negative IgM reactions can be observed during secondary infections [1]. However, it has high sensitivity and specificity and IgM remains stable at tropical room temperature [17]. In endemic countries, where subclinical infections are common, patient may fail to present within the first few days of illness (the time period for maximum NS1Ag serologic detection), then, it is the IgM antibody detection which clinches the diagnosis [18].
In the present study, we observed that if we had used only NS-1Ag for the diagnosis we would have missed 1130 positive cases reporting only 1319 cases among 2449 positive samples and in case only IgM ELISA test had been done, 797 positive patients would had been missed. NVBDCP (India) has given the guidelines to test for NS1Ag ELISA in the first 5 days of illness and to test for IgM antibodies if the duration of illness is more than 5 days [19]. Two points are of importance in this regard: first, that the day of illness of the patient is recorded diligently to choose an appropriate test. Second, the time zone of 5-9 days is very crucial. During this period, an interaction between the clinician and the microbiologist and putting up both the tests on the same sample could be crucial to effectively diagnose dengue illness. As previously suggested by Mahapatra et al., also, first five days, NS1Ag assay should be the test of choice but sixth day onwards, combination of MAC ELISA and NS1Ag assay should be put up to increase the sensitivity of diagnosis and after 10 days, IgM ELISA should be the method of choice for diagnosis [20].
We found dengue to be more prevalent in males but the ratio M:F (1.2:1) was not significant. Literature have reported varying results with some authors reporting similar pattern [14,21] and others reporting significant male preponderance (2:1). [1,2]. Though no reasons of genetic or environmental factors have been explained for this gender affinity.
Infection was found in all the age groups, but the most affected was 16-45 yrs, similar affected population was reported from Southern India, Indo-Myanmar, Andhra Pradesh (secondary infection), Chandigarh and Pakistan [8,9,13,17,22]. Predominance of the infection was seen in paediatric group by Garg et al., in his five year study but we report only 2.8% infection in paediatric population [2]. Dengue prevalence in pregnant females in our study was found to be 4.6% of the total positive patients. The importance and outcome in pregnancy with dengue is not yet established and various studies have reported varying results [23,24].
As there is no specific treatment for the disease, it is important to implement public health policies and vector control measures, presently as the only way to curtail the disease. Though Chandigarh is well planned and clean city but urbanization and construction activities in the periphery is poorly maintained and mosquitoes find favourable breeding sites like open water storage tanks, discarded tyres, tins and dumps. In Indoors, people unknowingly provide favourable sites for mosquito breeding like indoor aquatic plants and coolers. These should be cleaned periodically and it should be stressed that simple changing of the water from these containers is not sufficient. Education regarding mosquitoes egg laying habits is necessary as aedes lay eggs at the water-air interface and due to slimy nature, these egg rafts attach firmly to the vessels and coolers, requiring vigorous scrubbing to detach them [25]. Moreover, these eggs are resistant to desiccation and can withstand drying for long periods (up to six months or more) [25]. They are capable of entering a state of dormancy and subsequently in suitable environment they complete their development [26]. With increasing endemicity of the dengue virus illness, it has become pertinent to take control of these mosquito species.
Limitation
Limitations of the present study include not able to do dengue IgG testing on the positive serum samples to ascertain primary or secondary dengue infection, due to economical restraints. We were also not able to determine the serotypes of the dengue virus, due to non feasibility of RT - PCR at our centre.
Conclusion
Dengue infection is endemic in our region with a trend which doesn’t appear to be waning. So, in the present scenario best way to control the disease is limited to the increasing surveillance capacity, outbreak response, integrated vector management coupled with early appropriate diagnosis. One vaccine has recently been approved which is effective in preventing severe dengue against all serotypes of dengue (Dengvaxia’ by Sanofi Pasteur) but for better management, we look forward to more antivirals and better vaccines in future to make dengue control a success.