Correlation between Age, Gender, Waist-Hip Ratio and Intra Ocular Pressure in Adult North Indian Population
Shikha Baisakhiya1, Surjit Singh2, Prafulla Manjhi3
1 Assistant Professor, Department of Physiology, Maharishi Markandeshwar Institute of Medical Sciences and Research, Mullana (Ambala) Haryana, India.
2 Professor, Department of Physiology, Maharishi Markandeshwar Institute of Medical Sciences and Research, Mullana (Ambala) Haryana, India.
3 Professor, Department of Ophthalmology, Maharishi Markandeshwar Institute of medical sciences and research, Mullana (Ambala) Haryana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Shikha Baisakhiya, F-18, MMU Campus, Mullana (Ambala), India.
E-mail: nitishikha2478@rediffmail.com
Introduction
Intraocular pressure (IOP) is affected by various systemic and local factors. The significance of studying the factors affecting IOP is because of its association with potentially blinding condition known as glaucoma.
Aim
Present study was conducted with the aim to find out the correlation between gender, age, Waist-Hip Ratio (WHR) and IOP.
Materials and Methods
The study included 300 healthy individuals between 40-79years of age. The subjects were divided into 2 categories according to gender i.e., male and female. The subjects were divided into 4 categories according to age i.e., 40-49years, 50-59years, 60-69years and 70-79years. The subjects were divided into two groups according to Waist-hip ratio (WHR) as per WHO guidelines: WHR <0.9 and WHR >0.9 in males and WHR <0.85 and WHR >0.85 in females. IOP was recorded in each group using Goldmann Applanation tonometer and statistical comparisons were made to find correlation between gender, age, Waist-hip ratio and IOP.
Results
There was no statistically significant difference between IOP of males and females (p=0.235). The age and IOP were positively correlated with each other i.e., IOP increases with increasing age (r=0.511, p<0.001). Higher WHR is associated with significantly higher IOP in both the genders (males r =0.644, p<0.001; females r=0.794, p<0.001).
Conclusion
There is no significant difference in IOP amongst males and females. Increasing age and higher WHR are risk factors for raised IOP.
Age and IOP, Gender and IOP, Glaucoma, Waist-hip ratio on IOP
Introduction
Intraocular Pressure (IOP) is affected by various systemic and local factors. The significance of studying the factors affecting IOP is because of its association with potentially blinding condition known as glaucoma. Various cross-sectional studies in the past have emphasized on a positive correlation between IOP and age and also association of IOP with various anthropometric parameters [1,2]. It has also been suggested that racial and ethnic differences in the individuals can also affect IOP. The region wise difference in IOP can also be attributed to environmental factors [3]. As genetic and environmental factors attribute to the region wise difference in levels of IOP hence data collection from different populations carries significance. There is abundance of data available on association of IOP with various systemic and local factors from Korean [3], Central Indian [4], Asian [5], South Indian [6], Chinese [7], Japanese [8] and Nigerian population [9]. Literature search suggest the inadequacy of data available from North Indian population. Most of the studies in the past have used BMI [9,10] as the parameter of obesity although it has now been suggested that WHR is superior to Body Mass Index (BMI) in predicting the association of diseases with obesity. Hence we used WHR as the index of fitness [11,12]. There is paucity of availability of data from the North Indian population so we conducted the present study to find out the relationship between gender, age, WHR and IOP in this region.
Materials and Methods
The current study was an observational, cross-sectional study conducted in the Department of Physiology in collaboration with Department of Ophthalmology of Maharishi Markandeshwar Institute of Medical Sciences and Research, Mullana (Ambala), Haryana during October 2014 and November 2015. The institutional research committee and ethics committee approval was taken before undergoing the study. The study included 300 healthy individuals. Informed consent was procured from all participants. A correlational study sample size was calculated from data available in published literature [13]. In this study, the r-value is 0.25. By calculating sample size using r=0.25, the sample size is calculated as 125. We have taken a sample size of 300 which is more than the desired. As there was availability of subjects we took a larger sample size. Subjects included in the study were between 40-79years of age. Subjects having diabetes mellitus, hypertension, or any other chronic metabolic disease were excluded from the study. Patient on medication of any form were also not included in the study. The subjects were divided into 2 categories according to gender i.e. male and female. The subjects were further subdivided into two categories based on WHR as per WHO guidelines: WHR <0.9 and WHR >0.9 in males and WHR <0.85 and WHR >0.85 in females [11,12]. The measurement of the waist circumference was done at the narrowest point between the inferior costal margin and iliac crest. The measurement of hip circumference was done at the most protuberant part of the buttocks. The subjects were divided into 4 categories according to age i.e., 40-49years, 50-59 years, 60-69years and 70-79years. We used slit lamp mounted Goldmann applantion tonometer-Haag-Streit model. The IOP recording was done in sitting position. Topical 0.5% paracaine drops was used for anaesthetizing the ocular surface. The tear film was stained using moistened fluoroscien strip. The mires were observed under Cobalt blue light by touching biprism to the cornea. The inner borders of the mires were touched with each other to obtain the IOP readings in grams. The reading obtained in grams was multiplied by 10 to obtain IOP reading in mm of Hg [14].
Statistical Analysis
The statistical analysis of the data was done using SPSS version 18.5. Student t-test was used to compare the two groups according to the gender and WHR. ANOVA test was used to compare the IOP in the groups according to age. Linear regression test was used to determine change in IOP per unit change in age and Waist-hip ratio. The p-value of <0.05 was considered significant in all the tests.
Results
The genderwise distribution of subjects was 158 females and 142 males. The mean systolic BP (s BP), diastolic BP (d BP) IOP and BMI is described age wise in [Table/Fig-1]. All these parameters increased with increasing age. The mean IOP of the males was 16.40±2.38mmHg. The mean of IOP of females was 16.03±2.94mmHg. The difference was statistically non-significant (p = 0.235) [Table/Fig-2]. The mean IOP of the age group 40-49year was 14.41±2.3mmHg. The mean IOP of the age group 50-59year was 16.17±2.11mmHg. The mean IOP of the age group 60-69year was 17.53±2.41mmHg. The mean IOP of the age group 70-79year was 18.08±2.32mmHg [Table/Fig-3]. The IOP was found to increase with age in both the genders. The difference was found to be statistically significant using ANOVA test (p <0.001) [Table/Fig-3]. The mean IOP of males with WHR <0.9 was 12.90±2.59mmHg and with WHR >0.9 was 16.56±3.11mmHg (p<0.001). The mean IOP of females with WHR<0.85 was 11.71±1.94mmHg and females with WHR>0.85 was 16.82±3.11 (p<0.001) [Table/Fig-4]. Linear regression tests were performed to determine change in IOP per unit change in age and WHR [Table/Fig-5,6 and 7]. The results of our study suggest an increase in IOP by 0.511 mm of Hg with each decade after the fourth decade of life. In females for increase in WHR by 0.2 there occurred a rise in IOP by 0.794mm of Hg. While in males an increase in WHR by 0.2 led to rise in IOP by 0.644mm of Hg.
Mean SBP, DBP, BMI and IOP age wise.
| Agegroup | Number ofsubjects(Total no.=300) | Mean s BP (mmHg) | Mean d BP(mmHg) | Mean BMI(Kg /m2) | Mean IOP(mmHg) |
|---|
| 40-49years | 102 | 117.69±12.55 | 77.69±7.98 | 22.56±3.27 | 14.41±2.3 |
| 50-59years | 77 | 131.19±16.38 | 84.47±9.12 | 23.59±3.89 | 16.17±2.11 |
| 60-69years | 74 | 150.65±12.7 | 92.24±4.84 | 25.89±4.1 | 17.53±2.41 |
| 70-79years | 47 | 158.34±10.14 | 94.60±5.32 | 27.37±4.16 | 18.08±2.32 |
| Significance* | <0.001 | <0.001 | <0.001 | <0.001 |
p<0.05* considered significant)
Note: s BP- systolic BP; d BP- diastolic BP; IOP- Intraocular Pressure
Statistical comparison of IOP among males and females.
| Mean IOP(femalen=158) | MeanIOP(Malen=142) | df | Sig.(2 tailed) | 95%confidenceInterval(lower) | 95%confidenceInterval(lower) |
|---|
| IOP mean | 16.03±2.9 | 16.4±2.3 | 298 | 0.235 | -0.24184 | -0.98208 |
p >0.05 considered non significant
Note: IOP- Intraocular Pressure
Statistical comparison of IOP with age (ANOVA test).
| Agegroup(years | MeanIOP | Sum ofSquares | df | Meansquare | F | Significance |
|---|
| 40-49 | 14.41±2.3 | 621.740 | 3 | 207.247 | 39.743 | <0.001* |
| 50-59 | 16.17±2.11 |
| 60-69 | 17.53±2.41 | 1543.530 | 296 | 5.215 |
| 70-79 | 18.08±2.32 | 2165.270 | 299 |
p <0.05*considered significant
Note: IOP- Intraocular Pressure
Mean IOP in males and females according to Waist-hip ratio groups.
| Male | WHR>0.9 | WHR <0.9 | Sig 2 tailed |
|---|
| Number | 81 | 61 | |
| IOP | 16.56±3.11 | 12.90±2.59 | <0.001* |
| Female | WHR >0.85 | WHR <0.85 | Sig 2 tailed |
| Number | 84 | 74 | |
| IOP | 16.82±3.11 | 11.71±1.94 | <0.001* |
p <0.05* was considered significant
Note: IOP- Intraocular Pressure; WHR- Waist Hip Ratio
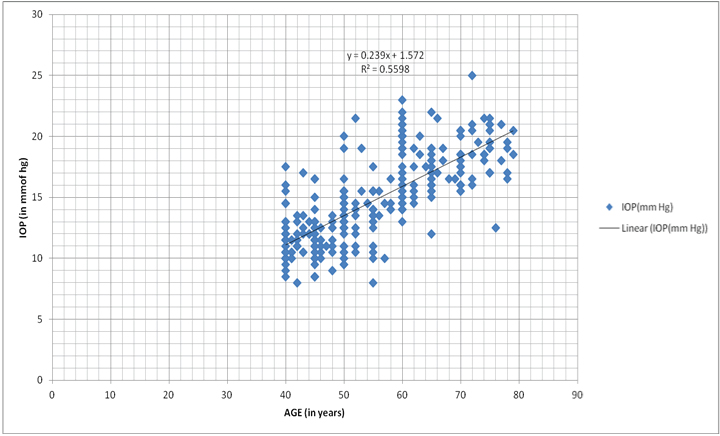
Graph representing correlation between IOP and age.
Note: IOP- Intraocular Pressure
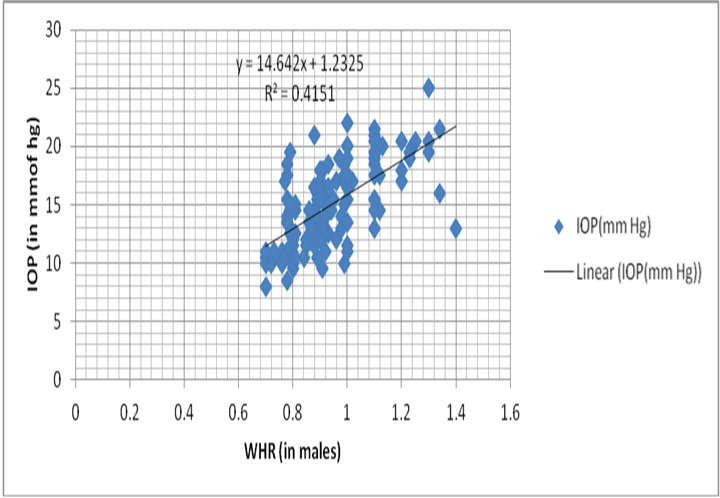
Graph representing correlation between IOP and WHR in males.
Note: IOP- Intraocular Pressure; WHR- Waist Hip Ratio
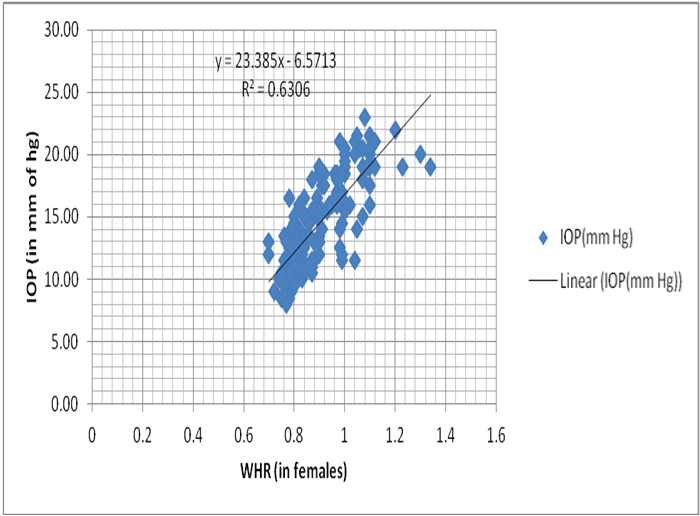
Graph representing correlation between IOP and WHR in males.
Note: IOP- Intraocular Pressure; WHR- Waist Hip Ratio
Discussion
Our observations suggest that IOP increases with increasing age and increasing WHR. The difference was found to be statistically significant in both the genders. We did not find any significant difference in IOP gender wise. In our study, the mean IOP of males was higher than that of females although, the difference was statistically non-significant. Gender wise difference reported in IOP in studies from various regions has shown variable results. Some studies report higher IOP among females while others report higher IOP in males. The genderwise difference in IOP could be due to hormonal factors, environmental conditions or inherent constituents [3] Similar to our findings, a study done on Central Indian population found no statistically significant difference between the IOP of males and females [4]. Shiose et al., also reported a higher mean IOP of 12.0 mm of Hg in males as compared to 11.5 mm of Hg in females by non-contact tonometry but the difference was non-significant [15]. A trend of higher IOP in males was also seen in Korean population. Also a high blood pressure and obesity index was noted among the males as compared to females hence the difference could be indirectly attributed to the systemic parameters. The findings of previous investigator suggest that with growing age the difference of IOP among males and females tend to decrease reaching similar-values for subjects above 70years of age. However, in younger age group males have higher IOP as compared to females [3]. We have also seen this trend in our findings the mean IOP of females in sixth and seventh decade was higher than the male counterparts in the same age group. Higher IOP in females have also been documented by few researchers [1,16].
In present study, there is a positive correlation of IOP with age in both the sexes. The mean IOP of 40-49year age group was lowest while that of 70-79year was highest. The results of our study suggest an increase in IOP by 0.511 mm of Hg with each decade after the fourth decade of life. The trend of increase in IOP with increasing age was found to be statistically significant (p<0.001). The results of our study showed a statistically significant difference in IOP between the age groups. Our findings were consistent with Wong T et al., they also noted an increase in IOP up to sixth decade. Beyond sixth decade there was no significant rise in IOP [5]. Investigators have noted an increasing trend of IOP with age in Pakistani, Iranian and Western population [1,2,17]. Epidemiological study done on South Indian population noted that the prevalence of glaucoma increased with age [6]. In our study, we noted higher SBP, DBP, BMI and Waist-hip ratio in subjects with increasing age. The increasing trend of IOP with age could be because of age related changes in the trabecular meshwork or could be indirectly attributed to change in systemic health parameters like high systemic arterial blood pressure and BMI [1,11,18]. Histological studies document a number of age related changes in the trabecular meshwork like thickening and fusion of trabecular sheets. With increasing age, there occurs accumulation of wide spacing collagen which decreases the aqueous outflow facility. With ageing, the crystalline lens increases in thickness and density in turn leads to compression of the schlemm’s canal and as a result obstruction of aqueous outflow [14]. Rise in systemic blood pressure and/or changes in anthropometric parameters could also be attributed to the rise in IOP with age [16]. Japanese population noted a decrease in IOP with increasing age. Also, a decrease in systemic blood pressure and body mass were noted with increasing age in them [8]. Study on Chinese and Singaporean population found no consistent relationship of age with IOP [7].
In our study, increase in WHR in both the sexes is associated with increase in IOP i.e., a positive correlation of IOP is seen with WHR. In females for increase in WHR by 0.2 there occurred a rise in IOP by 0.794 mm of Hg. While in males, an increase in WHR by 0.2 led to rise in IOP by 0.644 mmHg. Researchers in the past have investigated the effect of BMI on IOP and found a positive correlation between the two. Obesity has been recognized as an independent risk factor for glaucoma by various workers in the past. Recent study done on Nigerian population suggests a positive correlation between obesity, blood pressure and IOP [9]. Positive correlation between BMI and IOP has been noted in Central and South Indian population [4,6,19]. The similar findings were noted in Chinese and Singaporean population in the Tanjong Pajor eye study [7]. Most investigators in past have used BMI as a measure of obesity while WHR and waist circumference has been documented by only a few researchers. Gutenberg health study on European population found a positive association between IOP, waist circumference and WHR [20]. The physiological basis for the correlation between raised IOP and obesity could be due to accumulation of fat in the periorbital space leading to raised episcleral venous pressure [10,15]. Increased resistance in aqueous outflow could also be attributed to the raised haematocrit in obese individuals. The exaggerated cortisol response in obesity could also be another cause [21,22]. Higher incidence of hypertension in obese subjects could also be indirectly linked to higher IOP in them.
Limitation
The current study was a cross-sectional study, we suggest longitudinal study to see the trend of IOP in both gender with increasing age. The positive effect of weight reduction and life style modification need further research.
Conclusion
The results of our study conclude that the gender has no significant correlation with IOP, while increasing age is a risk factor for raised IOP and hence for glaucoma. Higher WHR is positively correlated with IOP in both the genders. Periodic checking of IOP in elderly and overweight individuals can play an important role in reducing the morbidity due to glaucoma. Life style modification in the form of exercise and dietary alteration can also be an important preventive measure.
p<0.05* considered significant)
Note: s BP- systolic BP; d BP- diastolic BP; IOP- Intraocular Pressure
p >0.05 considered non significant
Note: IOP- Intraocular Pressure
p <0.05*considered significant
Note: IOP- Intraocular Pressure
p <0.05* was considered significant
Note: IOP- Intraocular Pressure; WHR- Waist Hip Ratio
[1]. Qureshi IA, Intraocular pressure: a comparative analysis in two sexesClin Physiol 1997 17(3):247-55. [Google Scholar]
[2]. Schulzer M, Drance SM, Intraocular pressure, systemic blood pressure and age: a correlational studyBr J Ophthalmol 1987 71:245-49. [Google Scholar]
[3]. Lee JS, Choi YR, Lee JE, Choi HY, Lee SH, Oum BS, Relationship between intraocular pressure and systemic health parameters in a Korean populationKorean J Ophthalmology 2002 16:13-19. [Google Scholar]
[4]. Nangia V, Martin A, Bhojwani K, Kulkarni M, Yadav M, Jonas JB, Optic disc size in a population based study in central India. The central India eye and medical studyActa Ophthalmol 2007 86:103-04. [Google Scholar]
[5]. Wong TT, Wong TY, Foster PJ, Crowston JG, Fong CW, Aung T, The relationship of intraocular pressure with age, systolic blood pressure and central corneal thickness in Asian populationInvest Ophthalmol Vis Sci 2009 5(9):4097-102. [Google Scholar]
[6]. Vijaya L, George R, Paul PG, Baskaran M, Arvind H, Raju P, Prevalance of primary open angle glaucoma in a rural south Indian populationInvest Ophthalmol Vis Sci 2005 46:4461-67. [Google Scholar]
[7]. Foster PJ, Machin D, Wong TY, Ng TP, Kirwan JF, Johnson GJ, Determinants of intraocular pressure and its association with glaucomatous optic neuropathy in Chinese Singaporeans: The Tanjong Pagar studyInvest Ophthalmol Vis Sci 2003 44:3885-89. [Google Scholar]
[8]. Mori K, Ando F, Nomura H, Sato Y, Shimokata H, Relationship between intraocular pressure and obesity in JapanInternational Journal of Epidemiology 2000 29:661-66. [Google Scholar]
[9]. George GO, Ajayi OB, Relationship between body mass index, Intraocular pressure, blood pressure and age in Nigerian populationJ Clin. Exp Ophthalmol 2015 6(3):1-5. [Google Scholar]
[10]. Baisakhiya S, Singh S, Mushtaq F, Correlative study of intraocular pressure and body mass index in North Indian subjectsInternational Journal of Medical and Health Sciences 2015 4(4):453-56. [Google Scholar]
[11]. Welborn TA, Dhaliwal SS, Preferred clinical measures of central obesity for predicting mortalityEuropean Journal of Clinical Nutrition 2007 61:1373-79. [Google Scholar]
[12]. Srikanthan P, Seeman TE, Karlamangla AS, Waist-hip-ratio as a predictor of all-cause mortality in high-functioning older adultsAnnals of Epidemiology 2009 19:724-31. [Google Scholar]
[13]. Kisan R, Kisan SR, Anitha OR, Chandrakala SP, Koujalagi RS, Correlation between the intraocular pressure and the blood pressure in different age groupsJournal of Clinical and Diagnostic Research 2012 6(4):581-85. [Google Scholar]
[14]. Stamper RL, Lieberman MF, Drake MV, Becker Shaffer’s diagnosis and therapy of the glaucomas 1999 7th editionMissouriMosby publishers [Google Scholar]
[15]. Shiose Y, Intraocular pressure new perspectivesSurv Ophthalmol 1990 34(6):413-35. [Google Scholar]
[16]. Bulpitt CJ, Lodes C, Everitt MG, Intraocular pressure and systemic blood pressure in the elderlyBr J Ophthalmol 1975 59(12):717-20. [Google Scholar]
[17]. Hashemi H, Kashi AH, Fotouhi A, Mohammad K, Distribution of intraocular pressure in healthy Iranian individuals: the Tehran eye studyBr J Ophthalmol 2005 89:650-57. [Google Scholar]
[18]. Baisakhiya S, Singh S, Manjhi P, Correlation between intraocular pressure and blood pressure in North Indian subjectsInternational Journal of Advanced Research 2015 3(7):1545-54. [Google Scholar]
[19]. Pai S, Pai S, Pai A, Ramasamy C, Kini RD, A Correlative Study of BMI and IOP in diabetic and nondiabeticThai Journal of Physiological Sciences 2008 21(2):74-78. [Google Scholar]
[20]. Hoehn R, Mirshahi A, Hoffmann EM, Kottler UB, Wild PS, Laubert-Reh D, Pfeiffer N, Distribution of intraocular pressure and its association with ocular features and cardiovascular risk factors: the Gutenberg Health StudyOphthalmology 2013 120(5):961-68. [Google Scholar]
[21]. Pasquali R, Gagliardi L, Vicennati V, Gambineri A, Colitta D, Ceroni L, ACTH and cortisol response to combined corticotropin releasing hormone arginine vasopressin stimulation in obese males and its relationship to body weight, fat distribution and parameters of the metabolic syndromeInt J Obes 1999 23:419-24. [Google Scholar]
[22]. Zafar D, Malik R, Ahmad I, Rahil N, Hussain M, Noman N, Correlation between body mass index and intraocular pressure in adultsGomal Journal of Medical Sciences 2010 8(1):85-88. [Google Scholar]