Topical Corticosteroids (TCs) have an important role in wide spectrum of dermatological conditions especially those characterized by hyper proliferation, inflammation and immunological responses [1,2]. TC are amongst the most commonly used medication in the outpatient Department of Dermatology because of its profound efficacy than the other group of drugs on the different skin conditions. In India, the annual sales figure of TCs was 14 billion rupees in 2013, which accounts for almost 82% of total dermatological product sale in the country [3].
Over the years TC is being increasingly abused by both patients and doctors as well. Apart from common indications such as psoriasis, atopic dermatitis, vitiligo, lichen planus, lichen simplex chronicus, discoid lupus erythematosus, etc., they are also being used for conditions such as melasma, urticarial and even undiagnosed skin rash by dermatologists and more so by general physicians [4]. This is because of the quick symptomatic relief of many skin disorders by the application of TC in the first instance. This can develop confidence in patient a little longer with a general physician or specialists other than dermatologist. In addition to this, studies done in patients presenting with steroid-related side effects have shown that, there are several non-medical advisers like friends, neighbours, beauticians, barbers, etc. telling them to use TCs as fairness/cosmetic creams, anti-acne, anti-fungal therapy and for any skin eruptions [5]. There is also a tendency to re-use old prescription for a new rash or lesion. Friends and relatives also share the same prescription presuming that similar looking skin problems can be self-treated by simply copying the old prescription is quite rampant. To add to this problem, there is unrestricted availability of these drugs almost at every chemist shop without a valid prescription by just asking for TC. Moreover, pharmacists in chemist shop and quacks whose qualification is not known also play as doctors doling out advice about which TCs to use. These instances, although reported from many places worldwide [6,7] have significant impact in our country where only few dermatologists are there to serve such large population with no strict regulations on over the counter (OTC) prescription of these drugs. Because of the easy availability and affordable prices of these potent type of TCs, misuse has been noted among the general population, producing many undesirable effects. In spite of being a serious issue, only few studies have investigated the misuse of TC products in India [8–14].
The present study was conducted to assess the prevalence of misuse of TCs, to find out the causes behind it and the cutaneous adverse effects associated with it so as to raise awareness about the misuse of these drugs.
Materials and Methods
This observational cross-sectional study involved a total of 2174 patients who attended a tertiary care government teaching Hospital in New Delhi from 1st June 2015 to 30th November 2015. The study was approved by the Institutional Ethical Committee. The patients included were of any age and sex attending dermatology OPD using TCs presently or in past for any indication. Past history of use of steroids was assessed on basis of any records available with the patients or if the patient was carrying the medicine with him. This also included patients who presented with the side-effects of these drugs as the chief complaint. Patients not willing to participate in the study and those on oral corticosteroids were excluded from the study.
All the patients included in the study were assessed for misuse of TC which was defined as inappropriate use of topical steroid on skin in terms of incorrect dosing, formulation, frequency, duration or indications used for certain skin problems. Patients were examined for cutaneous adverse effects of TCs. This study was a self-designed questionnaire based study. Patients were interviewed directly using pretested and validated structured questionnaire containing 12 questions after getting their written informed consent as well as from patients whose pictures were taken to present the side effects of TC.
After that patients were also counselled for the rational use of the topical steroid and appropriate treatment was given for the presence of side effects, if any.
Statistical Analysis
Pie chart and percentage calculation done by Microsoft excel office 2010.
Results
Out of 2174 patients, using TC for any indication, enrolled during the study period, 256 (11.77%) patients were found to be misusing TCs and out of these 250 had clinically evident adverse effects of TCs. 60% of the study population were females. Most of the patients were in the age group of 20-29 years (38%) and 20% were illiterate. Demographic characteristics are listed in [Table/Fig-1].
Demographic status of patients (n=250).
| Age group(years) | Number (%) |
|---|
| 0-9 | 5 (2%) |
| 10-19 | 70 (28%) |
| 20-29 | 95 (38%) |
| 30-39 | 41 (16.4%) |
| 40-49 | 28 (11.2%) |
| >50 | 11 (4.4) |
| Gender |
| Male | 100 (40%) |
| Female | 150 (60%) |
| Education | |
| Illiterate | 50 (20%) |
| Primary | 60 (24%) |
| High school | 104 (41.6%) |
| Graduate | 36 (14.4%) |
| Occupation |
| Employed | 60 (24%) |
| Unemployed | 190 (76%) |
| Awareness of side effects |
| Aware | 8(3.2%) |
| Not Aware | 242(96.8%) |
Most common indication for misuse of steroid was dermatophytosis or fungal infection (38%), other indications being enlisted in [Table/Fig-2]. Some patients used these for more than one reason (1.2%). Steroids of varying potency were used by the patients commonest being Betamethasone Valerate (72.8%) followed by use of topical combination of Clobetasole Propionate, anti-biotics and anti-fungals (18.4%). The various TCs used are summarized in [Table/Fig-2]. The mean duration of use of TC was 2 months (68%) which ranged from 1 day to 15 years. Out of 250 patients 241 patients misused in terms of duration (more than the required duration) summarized in [Table/Fig-2].
Reasons for use of topical corticosteroid.
| Reason for using TC | Numbers(n=250) |
|---|
| Dermatophytosis | 96 (38.4%) |
| Acne Vulgaris | 73(29.2%) |
| Others (intertrigo, insect bite, eczema, urticaria) | 33 (13.2%) |
| Lightening of Skin Colour | 21(8.4%) |
| Melasma | 18(7.2%) |
| Bacterial /Viral | 9(3.6%) |
| TC formulation misused (n=250) |
| Betamethasone Valerate (0.1%) | 182 (72.8%) |
| Combination (clobetasole propionate, anti-fungal and anti-biotics) | 46(18.4%) |
| Clobetasole(0.01%) | 9(3.6%) |
| Mometasone Furoate (0.1%) | 8 (3.2%) |
| Fluticasone Propionate (0.05%) | 3(1.2%) |
| Halobetasol | 1 (0.4%) |
| Hydrocortisone | 1 (0.4%) |
| Duration of misuse of TC (n=241) |
| < 3 months | 170 (68%) |
| 3 – 6 months | 32 (12.8%) |
| 1-3 years | 6(2.4%) |
| >6 months | 12 (4.8%) |
| 6 months- 1 year | 11 (4.4%) |
| 3 – 5 years | 6 (2.4%) |
| >5 years | 4 (1.6%) |
Most of the patients (97.6%) did not know the dosage i.e., how much amount of the drug should be used for each particular body area. One patient had applied 5 tubes of topical steroid within 1 week as advised by pharmacist. A total of 85(34%) patients inappropriately used the TC in terms of incorrect frequency. Out of these 85 patients 66% people had the history of application of one of the above mentioned product once/twice a day, 8 patients used the TC more than required duration as prescribed by the physicians.
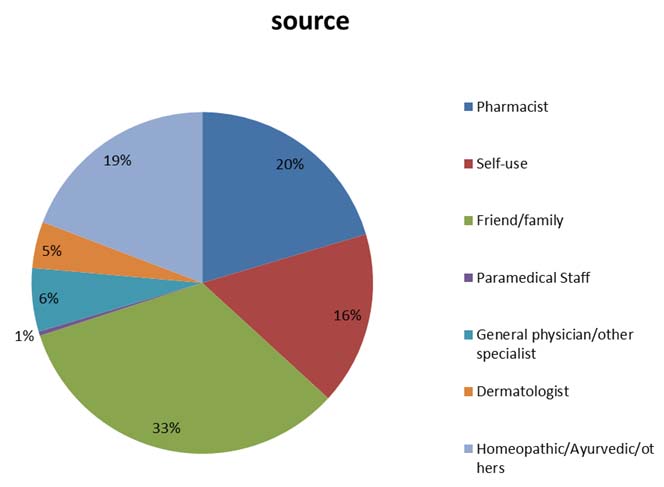
Source of advice for initiation of steroid application was majorly friends and family [Table/Fig-3]. Dermatologists contributed only 4.45% to the source. Only 3.2% patients had some knowledge of the adverse effects of TCs and 96.8% were unaware about the side effects with improper use as depicted in [Table/Fig-1].
Sources for using topical corticosteroids (n=250)
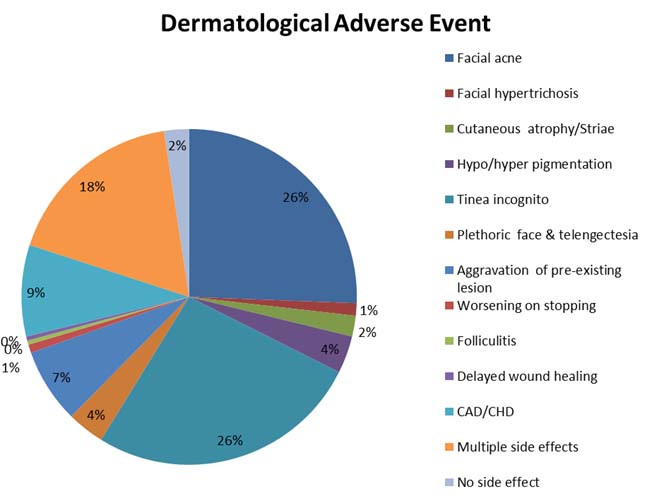
The dermatological side effects which were seen in our patients after application of topical steroids are listed in [Table/Fig-4]. Most common side effect seen was tinea incognito in 26.4% followed by facial acne in 25.6%, plethoric face and telengiectasis in 3.6%. Patients who presented with acneiform eruptions had sudden onset of lesions at the sites of application with predominance of papulopustular lesions. Photographs representing some of the adverse effects are shown in [Table/Fig 5,6,7,8,9,10,11 and 12].
Dermatological adverse effects seen (n=250).
Tinea incognito: The patient had applied topical corticosteroids that masked a diagnosis of tinea.


Patient presented with telangiectasia.

Generalized facial erythema and photosensitivity.

Topical steroid induced hypertrichosis.

Aggrevation of intertrigo due to topical steroid.

Acneform eruption with post-inflammatory pigmentation.

Steroid acne on the face.

Discussion
Glucocorticoids are used topically for a large variety of dermatological conditions. The intensity of the action depends on the extent of absorption to the deeper layers, thus, lipophilicity of the compound determines potency to a great extent. Ever since, the invention of TCs like hydrocortisone in 1952, a large number of similar molecules were discovered including Triamcinolone Acetonide (1958), Fluocinolone Acetonide (1961), Betamethasone (1963), Clobetasole Propionate (1974), Clobetasole Butyrate (1978), Fluticasone (1990), Halobetasole (1990), Fluticasone (1990), Mometasone (1991) and a host of other molecules. These molecules are of varying potencies as determined by their vasoconstrictrive properties [15].
Misuse or abuse of TCs appears to be a common problem in our country. This is reflected by the large proportion of patients who visit the Dermatology Department with the adverse effects of these drugs. However, the real problem is even greater than what appears there are a number of indications where these are contraindicated, but if applied to bring about an initial relief, making the disease very difficult to treat by a dermatologist as the clinical picture and response to the actual treatment gets modified significantly.
It has been observed that, in various skin conditions like primary bacterial and fungal infections, undiagnosed skin rash, acne and as fairness cream, irrational use of TC just for initial relief of the symptoms by pharmacists at chemist shops or non-qualified practitioners or by advise of friends and relative [6–9] are serious area of concern. According to Drugs and Cosmetics (D and C) Act 1940, the TCs fall under the category of Schedule H drugs and these drugs should be sold in chemist shops only on the prescription of a registered doctor, which is hardly ever practiced in India [16]. Unapproved use of TC seems to be a common clinical practice in India as all approved dermatological indications are mentioned on Central Drugs Standard Control Organization (CDSCO). Apart from that, the Indian market is flooded with several Fixed Dose Combinations (FDCs) of corticosteroids with anti-bacterial and anti-fungal agents, which in no way can be considered as scientific and rational [17,18].
Various recent studies on prescription patterns of TCs in dermatology outpatient department in tertiary care center have been done in India [19–22]. In one study topical steroids were given in 28.4% of all the prescriptions where drug dose, quantity, frequency and duration were not mentioned. Another study done by Madarkar et al., observed that, out of all drugs prescribed 15.4% were topical steroids and out of these about 11.8% of the prescriptions contained steroids of potent nature [20]. Duration of applications was not mentioned in 35.04% of these prescriptions and site of application was mentioned only in 53.8% prescriptions. Thus, dermatologists are also liable for misuse of TC as they do not write the proper instructions for exact duration, dose and amount to be applied and thus, awareness among dermatologists is a must for the same.
Very few studies have been done on misuse of topical steroid and the causes behind it in India [8–11]. In our study we evaluated the reasons behind the abuse of TC where people of various age groups, different educational status, and employment were found to be using TCs as self-medication for conditions where their use is actually not indicated. Similar kind of study was done by Dey and Sinha et al., [8,9]. Most topical products/steroids abusers in these studies were in the 10–29 years age group quite similar to our study probably in this period young people start to take care of their appearance. However, in most of the studies, data were limited to usage on the face, whereas, in our study, we found topical steroids abuse anywhere on the body. Study done by Sinha et al., was quite different from our study as in that all patients attending Dermatology Department for skin diseases were enquired about the unsupervised use of any cosmetic product on their facial skin and in case of a positive affirmation, the nature of the product was confirmed by showing them photographs of commonly used products [9]. The reason for TC abuse was found to be lightening of skin in 74%, melasma (14%), acne induced hyperpigmentation (8%) and dark circles (4%). About 80% people had obtained one or the other products OTC 8% had followed the attractive advertisements, 8% had started the application on the recommendation of friends/family while only 4% people had correctly gone through the proper channel to consult a dermatologist.
In study done by Dey VK, lightening of skin was the main reason of using TC in the absence of any primary dermatosis and was seen in 50.39% patients [8].
However, in our study fungal infection was the main cause (38.4%) of using TC, probably due to the humid weather experienced during the study period resulting in fungal infections being the most common presentation in dermatology OPD.
TC have emerged in recent years as major skin lighteners owing to their potent bleaching power and perhaps also their anti-inflammatory activity, which can reduce the risk for dermatitis [23]. We observed a trend of use of TC as fairness cream in our study with 8.4% of our patients using TC for this indication. A study by Agarwal et al., on evaluation of steroids in face creams of different marketed brands concluded that more than 60% of all skin products/cosmetics that claim to produce instant glow, contain steroid which can lead to serious damage to the skin [24]. Skin lightening was the main reason for the use of the TC (65.7%) in another study done in an Iraqi hospital [9]. This attitude is prevalent across the globe with minor variations in other countries as evidenced by various population based studies [25–28]. This may also explain the female predominance (60%) in the patients we studied. Various studies on facial abuse of TC has already been done not only in India but across the globe where the representative sample of adults mostly young female used the TC totally ignorant of its adverse effects just for the craziness for getting a fair skin [10,11,14].
Most of the patients in our study (83%) used potent to very potent TCs as depicted in [Table/Fig-2] such as (Betamethasone Valerate (0.1%). The most popular brands in our study were Betnovate® followed by mixed preparation of Clobetasol Propionate with anti-fungal and anti-bacterial (18.4%) (Clobevate®, Fourderm, Cortiderm). In study done by Dey VK, 39.84% applied mixed combinations as these combinations are easily available and cheap and are sold without medical prescription [8]. We also ascertained who advised regarding the prescription of these creams and found that in majority of the patients, the source was friends, relatives and peers in 33.2%, self-use in 16.4% and RMPs and quacks in 19.2%, only in a few patients’ topical TCs prescribed by a physician or a dermatologist. In our study, effortless source of supply of these products were pharmacies in 20.4% reflecting the lax regulatory oversight, and influence of aggressive marketing and advertising.
TC is used primarily for their anti-inflammatory properties [29]. However, their inappropriate use can lead to multiple local side effects including atrophy, striae, telengiectasis, purpura, hypo-pigmentation, acneiform eruptions, rosacea-like perioral and periorbital dermatitis, and hypertrichosis [30–41], if used in inappropriate indications, they may modify the clinical picture of the disease, altering the normal presentation thus, masking diagnosis and make further treatment more difficult, as is seen in case of tinea incognito [Table/Fig-5] which was the most common adverse effect found in our study (26%), Emergence of facial acne also came out to be another major effect of misuse of TC (25.6%). Chohan et al., found facial erythema to be the most prominent adverse effect shown in their study of facial abuse of topical steroids and fairness creams in Pakistan [14]. Dey VK, found facial acne in almost 37% and tinea incognito in only 4.8% due to misuse of TC [8]. Prolonged and continuous uses of TC on face leads to development of dermatoses which has been named variously by different workers and is presently called “Topical Steroid-Dependent Face” (TSDF) [11]. This has a distinct clinical presentation. Patients are mostly females who keep on using the steroidal cream till they get magical response and continue it later to prevent rebound flare till finally the lesions become persistent [Table/Fig-6,7 and 8].
Contact Dermatitis (CAD-contact allergic dermatitis/CHD-contact hand dermatitis) due to TC is not uncommon. The estimated prevalence was found to be in the range of 0.2–6% in previous studies [42]. Non-fluorinated corticosteroids are more likely to cause CD. According to Monthly Index of Medical Specialities (MIMS), India and Indian Drug Review, 11 TCs of different potencies are available in India with 119 FDCs of these corticosteroids with other agents (anti-bacterial, anti-fungal, keratolytic etc.,) [43–45]. However, only 27 of these 119 formulations available are among the CDSCO’s approved list of FDCs from 1961 to July 2014 in India [15] implying that the manufacturing and marketing of rest has not been permitted in the country. Thus, we need stringent actions and rules against the pharmaceutical companies who are marketing these non-approved FDCs and against chemists who dispenses these medications without a valid prescription to regulate dermatological drug market in the country. Similar situation is hardly seen in western countries where FDC’s are hardly used and topical steroids are never dispensed without prescription [45].
However, in the absence of proper surveillance mechanisms by the Indian drug regulatory authority, Task force Against Topical Steroid Abuse (IADVL Task Force Against Topical Steroid Abuse (ITATSA) is a welcome step in this direction [46]. ITATSA is a special task force created by Indian Association of Dermatologists, Venereologists and Leprologists (IADVL) to look into issues related to TC abuse. It has raised the issue of TC misuse at various fronts including physicians, manufactures, pharmaceutical companies and regulators. One such effort is this online petition, which is being given to the Ministry of Health and Family Welfare, Government of India and Central Drugs Standard Control Organization (CDSCO) which stresses upon issues related to the indiscriminate sale of TCs without prescription in India due to unregulated market and also makes an effort to sensitize common people about the risks associated with their use. The drug regulator could also create a new category of OTC TCs, which could include only one or two of the mild potency preparations and the rest all will be sold only on valid prescriptions.
Particularly in peripheral areas of our country mostly the chemists play a significant role in inappropriate use of the TC where they are first person to contact for any health related problems. The central and state drug regulatory authorities need to be active in sensitizing chemists about the deleterious effects of TC abuse and to physicians, dermatologists regarding the right use of TC including dose, frequency, site and duration. Also, they should understand that TC’s should never be used to bring about an initial relief in conditions where they are not indicated just to make the patient happy as it eventually would cause more harm. Regular continuing medical education and workshops to create awareness regarding this important issue will go a long way to ensure rational use of TCs. Along with this, there is need to sensitize patients, the actual user, about the adverse effects of TC abuse on face.
Limitation
The limitation of the study was that as this was an OPD-based study, it may or may not accurately reflect the community data but it certainly highlights misuse of TCs particularly among common people.
Conclusion
Topical steroid misuse is rampant in Indian society and fault lies at all levels-patient, doctors, pharmaceutical companies, chemists and the regulatory authorities. This leads to significant morbidity and psychological distress as usually the face is affected which is the prime site of aesthetics and thus a major cosmetic concern. Sensitization at all the levels and a coordinated approach is the need of the hour.