Identifying Aarskog Syndrome
Anis Ahmed1, Abdullah Mufeed2, Ashir Kolikkal Ramachamparambathu3, Umer Hasoon4
1 Reader, Department of Oral Medicine and Radiology, Indira Gandhi Institute of Dental Sciences, Cochin, Kerala, India.
2 Reader, Department of Oral Medicine and Radiology, MES Dental College, Perinthalmanna, Kerala, India.
3 Reader, Department of Oral Medicine and Radiology, KMCT Dental College, Calicut, Kerala, India.
4 Reader, Department of Oral and Maxillofacial Surgery, KMCT Dental College, Calicut, Kerala, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Anis Ahmed, Reader, Department of Oral Medicine and Radiology, Indira Gandhi Institute of Dental Sciences, Cochin, Kerala, India.
E-mail: dranisahmed@rediffmail.com
Aarskog syndrome also known as Aarskog-Scott Syndrome, Facio-digito-genital Syndrome or Faciogenital Dysplasia is a rare, X-linked disorder predominantly affecting males, characterized by facial, skeletal and genital anomalies. This is a case report of a 15-year-old male patient who visited our college complaining of poor facial aesthetics. History revealed consanguinity and his sibling to be suffering from the same. A diagnosis of Aarskog syndrome was made based upon the detailed patient history, thorough clinical evaluation and identification of characteristic findings in radiographs. Professional counselling explained him the nature of his condition and treatment options to correct dental anomalies and congenital malformations were advised.
Aarskog-Scott syndrome, Facial anomalies, Genital anomalies
Case Report
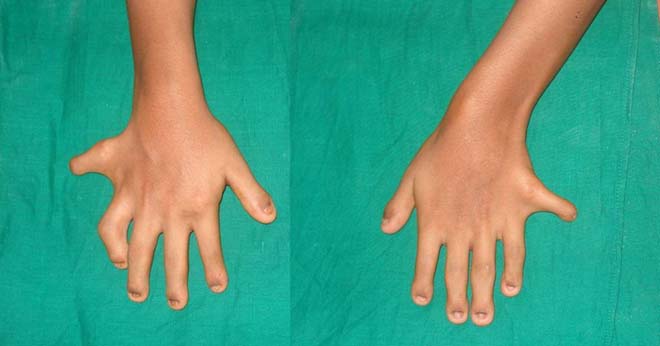
Syndromes not associated with severe medical problems or mental retardation can easily go unnoticed by physicians who may not be aware of the syndrome and co-related features. We report a case of 15-year-old male patient who came with a complaint of poor aesthetics because of missing teeth in the front region of the upper and lower jaws since childhood. He gave no history of extraction or exfoliation of teeth in front region of the jaw and there was no history of trauma either. He stated that he was the second son of consanguineous parents and had two brothers; the elder brother had a short stature, missing teeth and extra fingers. No relevant medical history was reported. On general examination he had short stature [Table/Fig-1], was well nourished and well oriented in time place and person. He had sparse scalp hair [Table/Fig-2]. His facial appearance was striking with abnormally large nose and ptosis of upper eyelids, hypertrophied and everted lower lip [Table/Fig-3]. The patient was 1.32 meter tall, weighed 46 kilograms and his vital signs were within the normal range. The patient had 6 digits on both his hands and the nails appeared smaller in size than normal [Table/Fig-4]. The patient could not adduct his thumb, index finger and the extra digit. Inward bowing of both lower limbs was noticed and both the feet had six toes [Table/Fig-5].


Large nose, droopy upper eyelids, hypertrophied and everted lower lip.

Extra finger on both hands, small nails.
Bowing of legs and extra toes.

Intra-oral examination revealed an abnormally large tongue covering the occlusal surface of the mandibular dentition. The maxillary lateral incisors and all four mandibular incisors were missing. A high arched palate was observed with palatal positioning of second premolars [Table/Fig-6]. The maxillary central incisors were macrodontic with altered morphology and diastema [Table/Fig-7]. All the canines were conical in shape and the edentulous ridge of mandibular incisor region showed a soft tissue prominence and hyperplastic labial frenum [Table/Fig-7]. Based on the history and the clinical findings a provisional diagnosis of acrodental dysostoses was arrived. The other differential diagnosis considered were Weyers acrodental dysostosis which besides the dwarfism, postaxial polydactyly and dysplastic teeth is also characterized by cardiac problems but as patient did not report of any systemic problems and examination of vital signs did not reveal any abnormalities this was ruled out. Aarskog syndrome was also considered as similar features are noticed as in this case but a characteristic feature of genital abnormality had to be further examined. Leopard syndrome was excluded because of absence of multiple black macules on the skin and absence of sensorineural deafness.
High arched palate, missing lateral incisors and palatally positioned premolars.

Altered morphology of central incisors with midline diastema and missing mandibular central and lateral incisors. Hyperplastic labial frenum and conical shaped canines.

Investigations: An Orthopantomograph (OPG) of the patient was done which confirmed all the clinical observations made regarding the number, shape and position of teeth. The hand wrist radiograph showed an extra digit and star like pattern of the digits [Table/Fig-8]. Further physical and clinical examinations were conducted by a general physician who acknowledged that there was no cardiac problem but the examination of genitals revealed unusual shawl like tissue around glans penis. This characteristic feature made us to presume the most probable diagnosis as Aarskog syndrome. Further blood investigations and genetic investigation to search for mutation in FGD1 were advised to the patient but he was quiet unwilling for further investigations. Besides explaining the patient his condition, prosthetic rehabilitation was done for him which was his main concern.
Star like pattern of hand radiograph.

Discussion
In 1970 Aarskog, in Norway, described a syndrome associating short stature with certain anomalies of the face, hands, feet, and genitalia in seven males from two generations of the same family [1]. The following year Scott also described a similar case [2]; thus, acquiring the name: Aarskog-Scott syndrome. It is an X-linked disorder caused by mutations in the FGD1 gene and therefore males express all the clinical manifestations and female carriers only show minor manifestations of the disorder, especially in the face and hands [3]. Typical features of Aarskog syndrome have been presented in [Table/Fig-9]. Population surveys estimate that the Aarskog-Scott syndrome occurs with a recognized frequency of approximately 1 per one million in general population [4]. Most of the cases are clinically diagnosed and only 35 molecularly proven cases have been published worldwide [Table/Fig-9] [5].
Typical features of Aarskog syndrome reported in the literature.
| General features [5,6,7] | Extra-oral features [6] | Intra-oral features [7,8] | Radiographic features [9] |
|---|
| - Short Stature- Severly shortened distal extremities- Webbed appearance of hands and feet- Hyperflexible joints- Short and inwardly curved little finger- Simian crease in the palm of the hand- Shawl scrotum or bifid scrotum- Delayed puberty | - Round face- Hypertelorism- Ptosis- Down slanting palpebral fissure- Broad nasal bridge with anteverted nostrils- Long upper lip with a linear dimple below the lower lip | - Maxillary hypoplasia- Missing teeth (either impacted or hypodontia)- Decreased vertical facial height | - Lumber kyphoscoliosis- Pes planovalgus (flat foot) |
| All these features were appreciated in our patient except for Lumbar Kyphoscoliosis |
There are no specific therapies for Aarskog syndrome. Some features such as inguinal or umbilical hernias, cryptorchidism and unusually severe craniofacial features may need surgical intervention [15]. Atypical features associated with Aarskog syndrome reported in the literature are shown in [Table/Fig-10].
Atypical features associated with Aarskog syndrome reported in the literature.
| Year of Publication | Author(s) | Uncommon findings associated with Aarskog syndrome |
|---|
| 1983 | Daniel LH [10] | The author reported a case with metatartus adductus (forefoot turned inwards) in Aarskog syndrome and emphasized on surgical correction of the same. |
| 1988 | Ahmad ST et al., [11] | The authors reported Aarskog syndrome in 5 siblings of consanguineous marriage. This is an exceptional case where the female siblings were also expressing the features of Aarskog syndrome. |
| 1992 | Ruth V-AM and Lurie IW [9] | The authors documented lymphoedema of the feet appreciated in maternal grandfather and grandson both of whom were affected with Aarskog syndrome. |
| 1999 | Waldo S et al., [12] | The authors describe a case of Aarskog syndrome identified prenatally by sonography at 28 weeks of pregnancy. Cystic hygroma and vertebral anomalies were diagnosed by ultrasonography which are not typical features of Aarskog syndrome. |
| 2005 | Mahmoud NS et al., [13] | The authors have published a case with congenital heart disease (aortic root dilation and sub-valvular aortic stenosis). They recommended cardiac screening for all patients with Aarskog syndrome. |
| 2012 | Raghavendra BN et al., [14] | The authors have published a case of Aarskog syndrome combined with temper tantrums, demanding behaviour, grandiose ideas, over familiarity, abusive assaultive behaviour and tobacco abuse in a 10 year old. Behavioural and personality disorders were not reported with the other cases. |
| 2016 | The present case | The atypical features noticed were polydactyl and alopecia. |
Conclusion
Aarskog syndrome may be undiagnosed due to the rarity of the condition and lack of knowledge. Dental and orofacial features are strikingly characteristic and play a key roll in the diagnosis of conditions like Aarskog syndrome. Diagnosis and management of rare syndromes will require a multidisciplinary approach involving paediatrician, orthopaedic surgeons, dentists and neuropsychiatrist.
[1]. Berry C, Cree J, Mann T, Aarskog’s syndromeArch Dis Child 1980 55:706-10. [Google Scholar]
[2]. Orrico A, Galli L, Faivre L, Clayton-Smith J, Azzarello-Burri SM, Hertz JM, Aarskog–Scott syndrome: Clinical update and report of nine novel mutations of the FGD1 geneAm J Med Genet A 2010 152:313-18. [Google Scholar]
[3]. Moraes SG, Guerra-Junio G, Maciel-Guerra AT, Female counterpart of shawl scrotum in Aarskog-Scott syndromeInternational Braz J Urol 2006 32:459-61. [Google Scholar]
[4]. Gorski JL, Estrada L, Changzhi H, Zhou L, Skeletal-specific expression of Fgd1 during bone formation and skeletal defects in faciogenital dysplasia (FGDY; Aarskog syndrome)Dev Dyn 2000 218:573-86. [Google Scholar]
[5]. Orrico A, Galli L, Clayton-Smith J, Jean-Pierre F, Clinical utility gene card for: Aarskog–Scott syndrome (faciogenital dysplasia) – update 2015Eur J of Hum Genet 2015 23(4) [Google Scholar]
[6]. Bozorgmehr B, Kariminejad A, Hadavi V, Kariminejad MH, Aarskog–Scott syndrome: Report of 7 cases and review of literatureGenetics in the third millennium 2006 4:954-56. [Google Scholar]
[7]. Jones KL, Smith’s recognizable patterns of human malformations 2006 6th edW.B. Saunders Company:134-35. [Google Scholar]
[8]. Luciane QC, Maximiano T, Caroline D, Daniele PC, Ivana AV, Aarskog-Scott syndrome: A review and case reportInt J Clin Pediatr Dent 2012 5(3):209-12. [Google Scholar]
[9]. Ruth V-AM, Lurie I W, Atypical case of Aarskog syndromeJ Med Genet 1992 29:349-50. [Google Scholar]
[10]. Daniel LH, Metatarsus adductus in two brothers with Aarskog syndromeJ Med Genet 1983 20(6):477 [Google Scholar]
[11]. Ahmad ST, Kamal KN, Sadika AA, Qasem AS, New autosomal recessive faciodigitogenital syndromeJ Med Genet 1988 25:400-06. [Google Scholar]
[12]. Waldo S, Victor D, Eleonora H, Mariana A, Prenatal sonographic diagnosis of Aarskog SyndromeJ Ultrasound Med 1999 18:707-10. [Google Scholar]
[13]. Mahmoud NS, Asif H, Chaudhari MP, Joel D, Case report – Congenital Aarskog syndrome with aortic root dilatation and sub-valvular aortic stenosis: Surgical managementInteract Cardiovasc Thorac Surg 2005 4:47-48. [Google Scholar]
[14]. Raghavendra BN, Ambika L, Bhogale GS, Apandurangi A, Mania with Aarskog-Scott SyndromeIndian Pediatr 2012 49:327-28. [Google Scholar]
[15]. Orrico A, Galli L, Obregon MG, de Castro Perez MF, Falciani M, Sorrentino V, Unusually severe expression of craniofacial features in Aarskog-Scott Síndrome due to a novel truncating variant of the FDG1 geneAm J Med Genet A 2007 143:58-63. [Google Scholar]