According to the World Health Report 2002, Cardio Vascular Diseases (CVD) will be the largest cause of death and disability in India by 2020 [1]. World Health Statistics 2016 claimed 17.5 million lives in 2012 (46% of all Non Communicable Disease deaths) – 6 million of which were under age 70. Of the 17.5 million deaths, 7.4 million were due to coronary heart disease and 6.7 million to stroke [2].
Aortic sclerosis is associated with increased incidence of myocardial infarction and cardiovascular death [3,4]. Detection of an ejection systolic murmur in the aortic valve region often corresponds to a diagnosis of aortic sclerosis or aortic stenosis. Ejection systolic murmur even though regarded as harmless, may also be found in patients with significant aortic valve obstruction and associated with increased cardiovascular events [5].
The epidemiological risk factors of calcific aortic valve disease resemble those of atherosclerosis and include age, male gender, hypertension, smoking, elevated levels of serum Low-Density Lipoprotein (LDL) cholesterol and diabetes [6,7].
In spite of the high incidence of myocardial infarction in our scenario, there is a lack of understanding of its association with the common finding of aortic valve sclerosis in our setup. Having an understanding of an association between the two, may help to understand better the complex patho-physiological aspects involved in acute coronary syndromes.
Materials and Methods
This prospective case control study was conducted in the medical Intensive Coronary Care Unit of North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences (NEIGRIHMS), Shillong, between 1st Jan 2015 to 31st Dec 2015. A total of 60 patients diagnosed with acute coronary syndromes were randomly selected and studied after obtaining the Institute ethics committee clearance. They were compared with 60 age and sex matched individuals admitted to In Patient Department for reasons other than acute coronary syndromes. The formula that was used for calculating sample size was:
Z1-α/2 = Is standard normal variate at 5% type 1 error (p<0.05) it is 1.96 was used in the formula.
p = Expected proportion in population based on previous studies or pilot studies.
d = Absolute error or precision (has to be decided by the researcher).
According to the study of Kearney K et al., the proportion of people having aortic sclerosis was ~ 4 [8]. The precision/absolute error was kept at 5% and type 1 error was kept at 5%.
So, if the above values are put in the formula above=

Inclusion Criteria
1) History of acute new onset chest pain within the previous 24 hours.
2) 12 lead electrocardiogram with changes suggestive of acute coronary syndromes.
Exclusion Criteria
Age < 18years.
Presence of aortic stenosis.
Past history of ischaemic heart disease.
Acquired immunodeficiency syndrome.
Known case of COPD or CRF or chronic liver disease.
Chronic steroid use.
Immunosuppressive therapy.
Any major surgery within the past two months.
Data were collected for the presence of aortic valve sclerosis and to study its association with the conventional risk factors of coronary artery disease and its impact on immediate outcome in patients with acute coronary syndromes.
Statistical analysis was performed using the SPSS version 22. The following tests were applied: percentages and Chi-square analysis was used to compare the frequency of events in each group.
Results
The [Table/Fig-1] shows that the cases had more incidences of aortic valve sclerosis but was not statistically significant (p-value 0.31).
Showing the prevalence of aortic valve sclerosis among cases and controls.
| SclAV | Cases | Controls | Total |
|---|
| Present | 11 | 7 | 18 |
| Absent | 49 | 53 | 102 |
| Total | 60 | 60 | 120 |
| Chi-Square | df | p-value | |
| 1.046 | 1 | 0.31 |
Scl AV – Sclerotic aortic valve
In the cases group aortic valve sclerosis was observed only after the age of 50 years and this association was statistically significant (p-value 0.04) while in the control group aortic valve sclerosis was observed only after the age of 60 years and this association was highly significant (p-value 0.001) [Table/Fig-2,3].
Showing age wise distribution of aortic valve sclerosis among cases and controls.
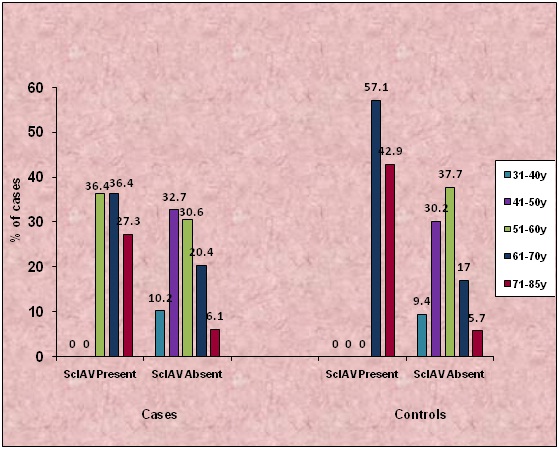
Showing the Chi- Square test results in cases and controls for age distribution.
| Test | Cases | Controls |
|---|
| Chi-Square | 9.807 | 18.574 |
| df | 4 | 4 |
| p-value | 0.044 | 0.001 |
In both the cases and control groups with no aortic valve sclerosis [Table/Fig-4] the percentage of male cases was more (67.3% in cases and 66% in controls).
Showing the gender-wise distribution of aortic valve sclerosis among cases and controls.
| Sex | Cases | Controls |
|---|
| Scl AV | Total | Scl AV | Total |
|---|
| Absent | Present | Absent | Present |
|---|
| Female | 16 | 6 | 22 | 18 | 4 | 22 |
| Male | 33 | 5 | 38 | 35 | 3 | 38 |
| Total | 49 | 11 | 60 | 53 | 7 | 60 |
| Chi-Square | 1.854 | 1.431 |
| df | 1 | 1 |
| p-value | 0.17 | 0.232 |
As per the modified Kuppuswamy classification subjects were divided into upper class, upper middle, upper lower, lower middle and lower class. Most of them belonged to the lower middle class (70% among cases and 60% among controls). No significant association of aortic valve sclerosis with socioeconomic class was seen [Table/Fig-5] [9].
Showing the socioeconomic class of cases and controls [9].
| Socio economic status | Cases | Controls |
|---|
| Scl AV | Total | Scl AV | Total |
|---|
| Absent | Present | Absent | Present |
|---|
| Lower Middle | 34 | 8 | 42 | 33 | 3 | 36 |
| Upper Class | 3 | 1 | 4 | 2 | 0 | 2 |
| Upper Middle | 12 | 2 | 14 | 18 | 4 | 22 |
| Total | 49 | 11 | 60 | 53 | 7 | 60 |
| Chi-Square | 0.286 | 1.558 |
| df | 2 | 2 |
| p-value | 0.87 | 0.459 |
While there was no significant association between the presence of hypertension [Table/Fig-6] and the presence of sclerotic aortic valve in the cases group there was a very significant association between the presence of hypertension and the presence of sclerotic aortic valve in the control group (p-value 0.009).
Showing the distribution of hypertensives, diabetics, tobacco use and BMI in sclerotic and non-sclerotic aortic valve among cases and controls.
| Cases | Controls |
|---|
| Scl AV | Total | Scl AV | Total |
|---|
| Absent | Present | Absent | Present |
|---|
| Hypertension |
| No | 33 | 6 | 39 | 45 | 3 | 48 |
| Yes | 16 | 5 | 21 | 8 | 4 | 12 |
| Chi-Square | 0.647 | 6.833 |
| df | 1 | 1 |
| p-value | 0.42 | 0.009 |
| Diabetes |
| No | 41 | 9 | 50 | 48 | 7 | 55 |
| Yes | 8 | 2 | 10 | 5 | 0 | 5 |
| Chi-Square | 0.022 | 0.720 |
| df | 1 | 1 |
| p-value | 0.88 | 0.396 |
| Tobacco use |
| No | 20 | 5 | 25 | 46 | 6 | 52 |
| Yes | 29 | 6 | 35 | 7 | 1 | 8 |
| Chi-Square | 0.080 | 0.006 |
| df | 1 | 1 |
| p-value | 0.78 | 0.937 |
| BMI (wt in kg/ht in cm2) |
| 18.5-24.9 | 33 | 9 | 42 | 46 | 5 | 51 |
| 25.0-29.9 | 15 | 1 | 16 | 7 | 2 | 9 |
| > 30 | 1 | 1 | 2 | 0 | 0 | 0 |
| Chi-Square | 3.169 | 1.145 |
| df | 2 | 1 |
| p-value | 0.205 | 0.285 |
Most subjects in the study were not known diabetics (83.3% in cases and 91.7% in cases). There was also no significant association between the presence of diabetes and the presence of sclerotic aortic valve in both the cases and control groups. No association was observed with tobacco consumption and presence of aortic valve sclerosis in either of the cases and control groups.
Most of the study subjects in the cases and control groups had normal BMI (70% in cases and 85% in controls). No significant association between an increase in BMI and the presence of sclerotic aortic valve in both the cases and control groups was noted. No significant association was found between total cholesterol levels with aortic valve sclerosis [Table/Fig-7] in the case group. But in the control group 28.6% of the subgroup with sclerotic aortic valve had total cholesterol levels > 240 mg/dL as compared to 5.7% in the subgroup without a sclerotic aortic valve which was statistically significant (p-value 0.048).
Showing Total Cholesterol, LDL, HDL, TGL levels in sclerotic and non-sclerotic aortic valve among cases and controls.
| Cases | Controls |
|---|
| Scl AV | Total | Scl AV | Total |
|---|
| Absent | Present | Absent | Present |
|---|
| T Chol (in mg/dl) |
| < 200 | 32 | 5 | 37 | 48 | 4 | 52 |
| 200-239 | 6 | 2 | 8 | 2 | 1 | 3 |
| > 240 | 11 | 4 | 15 | 3 | 2 | 5 |
| Chi-Square | 1.507 | 6.058 |
| df | 2 | 2 |
| p-value | 0.471 | 0.048 |
| LDL levels (mg/dl) |
| < 100 | 23 | 3 | 26 | 35 | 4 | 39 |
| 100-129 | 11 | 2 | 13 | 14 | 0 | 14 |
| 130-160 | 3 | 3 | 6 | 2 | 1 | 3 |
| > 160 | 12 | 3 | 15 | 2 | 2 | 4 |
| Chi-Square | 4.924 | 8.994 |
| df | 3 | 3 |
| p-value | 0.177 | 0.029 |
| HDL levels (mg/dl) |
| < 40 | 13 | 3 | 16 | 29 | 2 | 31 |
| 40-60 | 32 | 5 | 37 | 23 | 3 | 26 |
| > 60 | 4 | 3 | 7 | 1 | 2 | 3 |
| Chi-Square | 3.388 | 9.624 |
| df | 2 | 2 |
| p-value | 0.184 | 0.008 |
| TGL levels (mg/dl) |
| < 150 | 31 | 6 | 37 | 44 | 5 | 49 |
| 150-200 | 10 | 2 | 12 | 7 | 1 | 8 |
| > 200 | 8 | 3 | 11 | 2 | 1 | 3 |
| Chi-Square | 0.720 | 1.474 |
| df | 2 | 2 |
| p-value | 0.698 | 0.479 |
No significant association was found between LDL levels with aortic valve sclerosis in the case group. In the control group 42.9% of the subjects with sclerotic aortic valve had a LDL value >130 mg/dl as compared to 7.6% in the subjects without sclerotic aortic valve and this association was found to be significant (p-value 0.029).
There was no association found between HDL and the presence of sclerotic aortic valve in the case group but a significant association (p-value= 0.008) was found in the control group where 28.6% of the subgroup with sclerotic aortic valve had HDL levels > 60 mg/dl as compared to 1.9% in the subgroup without aortic valve sclerosis. No significant association between TGL levels with aortic valve sclerosis either in the case or control groups was seen.
Among the cases anterior wall MI was the most common form of Acute Coronary Syndrome in both the sub-groups [Table/Fig-8]. A 18.2% of subgroup with sclerotic AV had a EF < 35% as compared to 8.2% in the subgroup without sclerotic AV but this was not found to be significant.
Showing ECG findings and EF% in cases with sclerotic and non-sclerotic aortic valve.
| Sclerotic Aortic Valve | Total |
|---|
| Absent | Present |
|---|
| ECG |
| AWSTEMI | 28 | 6 | 34 |
| EAWMI | 5 | 0 | 5 |
| EIWMI | 5 | 0 | 5 |
| IWSTEMI | 11 | 5 | 16 |
| EF% |
| < 35 | 4 | 2 | 6 |
| 35-44 | 24 | 4 | 28 |
| 45-54 | 16 | 4 | 20 |
| > 54 | 5 | 1 | 6 |
| Chi-square | 1.256 |
| df | 3 |
| p-value | 0.74 |
AWSTEMI – anterior wall ST elevation MI
EAWMI – evolved anterior wall MI
EIWMI – evolved inferior wall MI
IWSTEMI – inferior wall ST elevation MI
EF- ejection fraction
Most patients presenting with acute coronary syndromes fell in Killip’s class 1 and no significant difference between the two subgroups i.e. those with and without sclerotic aortic valve was noted in terms of their Killip’s class [Table/Fig-9].
Showing Killip’s class in cases with sclerotic and non-sclerotic aortic valve.
| Killip’s Class | Sclerotic Aortic Valve | Total |
|---|
| Absent | Present |
|---|
| 1 | 39 | 7 | 46 |
| 2 | 8 | 3 | 11 |
| 3 | 2 | 1 | 3 |
| Chi-square | 1.336 |
| df | 2 |
| p-value | 0.513 |
No significant association was found between immediate outcome and the presence or absence of aortic valve sclerosis in patients presenting with acute coronary syndromes [Table/Fig-10].
Showing immediate outcomes in cases with sclerotic and non-sclerotic aortic valve.
| Outcome | Scl AV Absent | Scl AV Absent | Z-test | Total |
|---|
| No./Total | % | No./Total | % |
|---|
| Death | 1/11 | 9.1 | 6/49 | 12.2 | 0.31 | 0.76 |
| CHF | 2/11 | 18.2 | 5/49 | 10.2 | 0.64 | 0.52 |
| CS | 2/11 | 18.2 | 7/49 | 14.3 | 0.31 | 0.76 |
| VT | 1/11 | 9.1 | 2/49 | 4.1 | 0.55 | 0.58 |
| CHB | 2/11 | 18.2 | 3/49 | 6.1 | 1 | 0.32 |
| UE | 6/11 | 54.5 | 32/49 | 65.3 | 0.66 | 0.51 |
CHF – congestive heart failure
CS – cardiogenic shock
VT – ventricular tachycardia
CHB – complete heart block
UE – uneventful
Discussion
Aortic valve sclerosis even without significant stenosis is associated with an increased risk of myocardial infarction and death from cardiovascular causes [3]. The demographic profile of patients of the present study was comparable with the Cardiovascular Health Study, the CREATE study, the Helsinki Ageing Study, Chandra et al., Agmon et al., Pohle et al., etc., [6,10–14]. In the present study no significant association was found between aortic valve sclerosis and male sex similar to the Helsinki Ageing Study and Chandra et al., [11,12]. But several other studies showed a significant association as in The Cardiovascular Health Study (p-value <0.001), Agmon et al., (p-value 0.01) and Pohle et al., (p-value <0.001) [6,13,14]. No association was found between aortic valve sclerosis and socioeconomic status, as most of the study subjects belonged to the lower middle class (70% among cases and 60% among controls) instead of upper middle or high socioeconomic status.
But David Messika and colleagues [15] showed that aortic valve calcification was frequent (27%) with ageing (p<0.01) and in men (p<0.05). No association was observed with tobacco consumption and presence of aortic valve sclerosis in either of the cases and control groups similar to other studies i.e., the Cardiovascular Health Study, the Helsinki Ageing Study and Agmon et al., etc., [6,7,13]. In our study hypertension, diabetes, weight, Body Mass Index (BMI), hyperglycaemia and hyperlipidemia were not found to be significantly associated with aortic valve sclerosis in patients presenting with acute coronary syndromes.
The Helsinki Ageing Study [7] showed that hypertension (p=0.005) and BMI (p=0.005) were independent predictors of aortic valve degeneration while smoking, diabetes, serum lipids and insulin were unrelated.
The Cardiovascular Health Study [6] showed that clinical factors associated with aortic valve sclerosis and stenosis was similar to risk factors for atherosclerosis: age, male gender, history of hypertension (p-value <0.001), elevated serum levels of Lipoprotein (a) and LDL cholesterol. No relation was found to diabetes (p-value 0.90) and smoking (p-value 0.43).
In an age and gender- stratified random sample of the Olmsted County (Minnesota) Agmon et al., showed that weight, body mass index (p=0.006), bodysurface area, antihypertensive drug treatment (p=0.02) were associated with aortic valve sclerosis after adjusting for age and gender, whereas diabetes mellitus, smoking and blood lipid levels were not [13].
Chandra et al., found that aortic valve sclerosis was associated with age and hypertension (p<0.05) however by multivariate analysis only age was associated with the presence of aortic sclerosis (p<0.0001) [12]. No association was found for male gender, diabetes, hyperlipidemia and smoking. Pohle et al., found that aortic valve calcification was found more frequently in patients with hyperlipidemia (p<0.001), hypertension (p=0.01) and diabetes (p=0.002) [14]. No statistically significant difference in the prevalence of aortic calcification was found for smoking (p=0.10) or a positive family history of coronary artery disease (p=0.10).
In our study, aortic valve sclerosis was found to be significantly associated with age, hypertension and hyperlipidemia in patients without ischaemic heart disease. This discrepancy in the association of aortic valve sclerosis with risk factors of atherosclerosis between the cases and the control groups could be explained by the fact that there is a high prevalence of risk factors in the cases group as these patients have already presented with an acute coronary syndrome which is absent in the control group thereby unmasking the association of aortic valve sclerosis with risk factors of atherosclerosis. There is no consensus on the association between aortic valve sclerosis and coronary artery disease with some reporting a 50% increase in cardiovascular mortality and thereby recommending use of statins and angiotensin-converting enzymes for secondary prevention [16]. At the other extreme, Tolstrup et al., found no association between aortic valve sclerosis and coronary artery disease [17] and Chandra and colleagues found no association between aortic valve sclerosis and the all-cause or cardiovascular mortality endpoint [12]. The study by Otto et al., represents a reference regarding the prognostic effect of aortic valve sclerosis on overall and cardiovascular mortality [3]. In this study, aortic valve sclerosis did not influence patients’ prognosis, with the exception of a subgroup of patients with no ischemic heart disease. The relative risk of death from cardio vascular causes among subjects without coronary heart disease at base line was 1.66 (95 percent confidence interval, 1.23 to 2.23) for those with sclerotic valves as compared with those with normal valves, after adjustment for age and sex. This adverse clinical outcome was also observed in the LIFE study, in which hypertensive patients with aortic valve sclerosis had almost twice the risk for serious cardiovascular events [18]. Aronow et al., reported that older patients with valvular aortic sclerosis have a higher risk (1.8 times) of new coronary events than older subjects without valvular aortic sclerosis, after controlling for the confounding effects of other prognostic variables [4].
In our study, the presence of aortic valve sclerosis was not associated with increased risk of cardiovascular mortality and morbidity. This may be explained by the fact that cardiovascular outcome in patients with aortic valve sclerosis was measured after they had presented with myocardial infarction. Therefore, we suppose that if a study were carried out to evaluate primarily the prognostic effect of aortic valve sclerosis in patients with no ischemic heart disease, it is likely that positive results would have been obtained. Another possibility is that in our study only immediate outcome over a period of 7 days was assessed thus if we were to follow-up these patients over a period of time a significant association might have been found. It is worthwhile to note here that all of the above mentioned studies showed significant association of aortic valve sclerosis with cardiovascular events only over one year. Chandra and colleagues who studied adverse outcomes in patients presenting with chest pain showed no difference in outcome at index admission and in-hospital death with the presence of aortic valve sclerosis but over one year, the presence and severity of aortic sclerosis were strongly associated with adverse cardiovascular outcomes [12].
Limitation
The limitation of the study was the time period of 24 hours from the onset of symptoms of acute coronary syndrome. Many patients who did not make it to the hospital in time excluded from the study and others whose ECG changes might appear after 24 hours of the onset of the symptomatology was also be excluded from the study.
Conclusion
The risk factors for atherosclerosis (age, hypertension and dyslipidemia) were associated with the presence of aortic valve sclerosis in the control group. Hence, finding of a sclerosed aortic valve on echocardiography will help identify those persons in the apparent normal population who might be at a high risk of having an underlying coronary artery disease and thus make them amenable for earlier treatment and prevention of acute coronary syndromes before it sets in.
Scl AV – Sclerotic aortic valve
AWSTEMI – anterior wall ST elevation MI
EAWMI – evolved anterior wall MI
EIWMI – evolved inferior wall MI
IWSTEMI – inferior wall ST elevation MI
EF- ejection fraction
CHF – congestive heart failure
CS – cardiogenic shock
VT – ventricular tachycardia
CHB – complete heart block
UE – uneventful