Non-surgical Management of Skeletal Class III Malocclusion with Bilateral Posterior Crossbite: A Case Report
Lalima Kumari1, Kamal Nayan2
1 Senior Lecturer, Department of Orthodontics and Dentofacial Orthopaedics, Haldia Institute of Dental Sciences and Research, Banbishnupur, West Bengal, India.
2 Senior Lecturer, Department of Prosthodontics and Crown and Bridge, Mithila Minority Dental College and Hospital, Darbhanga, Bihar, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Lalima Kumari, C/O Sri Bhuwaneshwar Rai, Friend’s Colony, Katira, Ara-802301, Bihar, India.
E-mail: lali3dec@gmail.com
A 16-year-old female patient with skeletal Class III malocclusion and bilateral posterior cross bite complaining of difficulty in chewing was treated orthodontically without surgery (camouflage treatment). The treatment comprised of fixed orthodontic treatment with MBT prescription (0.022˝×0.028˝ slot) using quad helix appliance for bilateral expansion of maxillary arch and Class III elastics for occlusal correction. Post-treatment records showed normal overbite and overjet with acceptable occlusion. So with this treatment strategy of expanding the maxillary arch using a quad helix appliance and use of Class III elastics, we achieved a good result with optimal occlusion.
Camouflage treatment, Class III elastics, Maxillary expansion, Quad helix
Case Report
A 16-years-old female patient was referred for orthodontic consul-tation. Her chief complaint was inability to chew well because her posterior teeth were not in contact properly while eating. The extra-oral examination showed a typical skeletal Class III facial pattern, with mandibular prognathism, increased lower anterior face height, leptoprosopic facial pattern and straight profile. Functional examination showed no abnormal features. Intraorally, she had Class III molar, canine and incisor relationships bilaterally and a bilateral posterior cross bite involving the canines, premolars and molars [Table/Fig-1]. Both the maxillary and mandibular midlines were coincident. The patient had composite restoration in the lower mandibular second molars. Study cast analysis showed a constricted maxillary arch [Table/Fig-2]. Pre-treatment Ortho- Pantomo-Gram (OPG) revealed no abnormality [Table/Fig-3]. The pre-treatment cephalogram [Table/Fig-4] showed a skeletal Class III jaw relationship (as indicated by ANB angle, -3°) with vertical growth pattern (SN-GoGn angle, 37° and FMA angle, 30°). The maxillary and mandibular incisors were slightly proclined and the curve of spee was mild. The bite was found to be edge to edge in the anterior region. The patient was in good general health with no history of major systemic diseases.
Pre-treatment photographs.


Pre-treatment lateral cephalogram.

Treatment objectives: Overall treatment objectives consisted of correcting the antero-posterior basal relationship by surgically advancing the maxilla and retruding the mandible. These changes were expected to greatly improve the patient’s facial aesthetics. Limited treatment objectives were to provide a camouflage treatment by correcting the anterior cross bite, eliminating the bilateral posterior cross bite by expanding the maxillary arch and to achieve normal occlusion with ideal overjet and overbite.
Treatment alternatives: As the patient had a skeletal Class III profile with prominent mandible, the best treatment modality considered was the orthognathic surgery in conjunction with orthodontic treatment after the attainment of 18 years of age. But as the patient was not ready for surgery, the treatment was aimed at the correction of the bilateral posterior cross bite as well as Class III malocclusion orthodontically using an expansion appliance for maxillary arch along with fixed mechanotherapy using medium torque prescription MBT (0.022˝×0.028˝ slot).
Treatment progress: The proposed orthodontic treatment involved the use of a quad helix appliance to expand the maxillary arch and fixed orthodontic appliances (MBT prescription, 0.022˝×0.028˝ slot) in both the arches. At first, all the first molars were banded and a quad helix appliance [Table/Fig-5] made of 0.036˝ stainless steel wire [1] was soldered to the maxillary molar band lingually to expand the maxillary arch. The expansion was stopped when the maxillary lingual cusps were in contact with mandibular buccal cusps. The total duration of expansion was four months. The same quad helix appliance was retained for a period of next three months for retention and stability. The quad helix was then replaced by a Transpalatal Arch (TPA) on the maxillary first molars for the remainder of treatment to prevent any relapse after expansion. Brackets were then bonded on both the arches and levelling and alignment were continued using 0.014˝, 0.016˝ and 0.017˝×0.025˝ nickel-titanium wire; followed by 0.017˝×0.025˝ and further by 0.019˝×0.025˝ stainless steel wires [Table/Fig-6]. During 0.017˝×0.025˝ stainless steel wire stage, Class III elastics were used judiciously to obtain an ideal occlusal relationship. Vertical settling elastics were used during the last one month of treatment. Debonding was done after a total treatment time of one year and nine months duration and removable Hawley’s retainers were delivered. Patient was advised to wear removable retainer on both the arches full time for a period of one year and then only during night for next six months.
Quad helix appliance design.

Mid-treatment photographs.

Treatment Results: Normal functional occlusion was established with normal overbite and overjet [Table/Fig-7]. The posterior crossbites were corrected and the final molar relationship was acceptable. There was no change in facial profile. The post-treatment radiographs [Table/Fig-8,9] showed no evidence of root resorption. Cephalometric analysis showed protraction of the maxillary complex, including the maxillary incisors and point A. Maxillary incisors were proclined and mandibular incisors were more retroclined after the treatment [Table/Fig-10].
Post-treatment photographs.

Post-treatment lateral cephalogram.


| Measurements | Pre-treatment | Post-treatment |
|---|
| SNA | 77° | 79 ° |
| SNB | 80 ° | 80 ° |
| ANB | -3° | -1° |
| SN-GoGn | 37 ° | 37 ° |
| U1-NA (Linear) | 10 mm | 11mm |
| U1-NA (Angular) | 38 ° | 41 ° |
| L1-NB (Linear) | 7mm | 5mm |
| L1-NB (Angular) | 21 ° | 12 ° |
| Inter-incisal angle | 124 ° | 125 ° |
| FMA | 30 ° | 31 ° |
| IMPA | 79 ° | 79 ° |
| Y-Axis | 57 ° | 59 ° |
| U Lip to E-Line | -4mm | -4mm |
| L Lip to E-Line | 0mm | 0mm |
Discussion
Class III malocclusion is one in which the lower first molar is mesially positioned relative to the upper first molar as described by Edward H Angle [2]. This relationship may result from a normal maxilla and a mandibular skeletal protrusion or a maxillary retrusion and a normal mandible or a combination of maxillary retrusion and mandibular protrusion.
Class III malocclusion with a significant skeletal component is an orthodontic challenge, especially when a conservative approach is requested. An important factor for the successful treatment of this malocclusion is the facial growth pattern. A reduced lower anterior face height, deep overbite and passive lip seal, associated with a Class III malocclusion, present a better prognosis, because treatment induced backward rotation of the mandible will assist in camouflaging the antero-posterior discrepancy. When an increased lower anterior face height is associated with this malocclusion, surgical intervention is the treatment of choice. However, for patients reluctant to undergo surgery or who are satisfied with their facial appearance, an alternative is to treat with dentoalveolar compensation without correcting the underlying skeletal deformity (Orthodontic camouflage) [3].
Posterior crossbite is defined as an inadequate transverse relation-ship of maxillary and mandibular teeth. It occurs when the buccal cusps of the maxillary posterior teeth occlude lingually to the buccal cusps of the corresponding mandibular teeth. The basic mechanisms of posterior cross bite remain unclear, but various combinations of dental, skeletal and neuromuscular functional components are known to be aetiologic factors [4]. The most common cause however, is a posterior transverse discrepancy due to reduced maxillary dental arch width alone or combined with increased mandibular arch width [5].
The management of a posterior crossbite is based on the cause of the discrepancy between the maxillary and mandibular arch widths. Treatment usually involves the use of a maxillary expansion appliance, which can take many forms. The recommended treatment for younger patients is expansion of the maxillary arch with a removable expansion plate or a quad-helix appliance after grinding the occlusal interferences [6,7]. If however, the posterior transverse discrepancy is caused by increased mandibular arch width only or combined with reduced maxillary arch width, it is difficult to achieve the desired effect with fixed appliances and a maxillary expansion appliance.
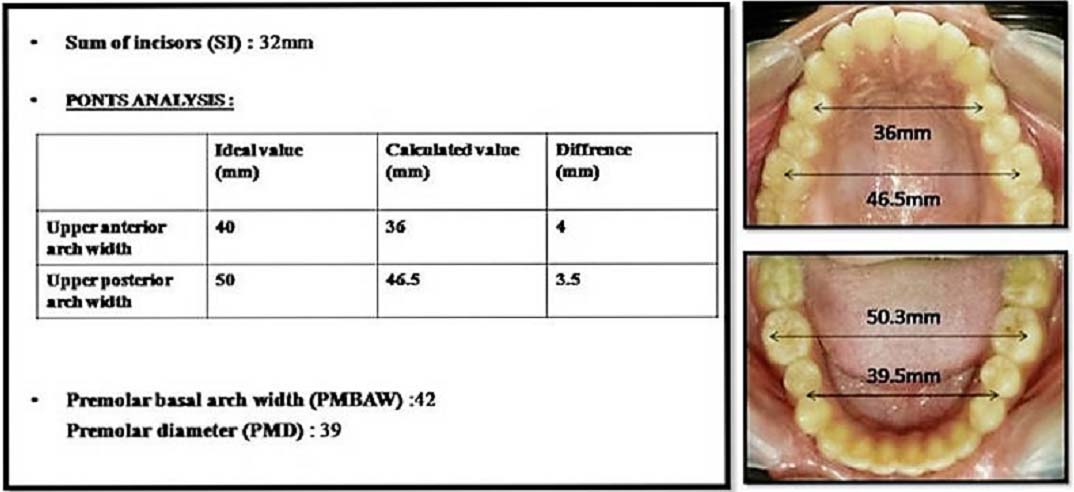
As in this case both the anterior as well as posterior arch width in the upper arch were found to be lesser as compared to the lower arch [Table/Fig-2], as well as to the ideal values given by Ponts and other authors [Table/Fig-11] [8], posterior cross bite was attributed to the constricted maxillary arch and hence, expansion of upper arch was planned.
Correlation between sum of upper incisors and dental arch width.
| Pre-treatment | Pont | Harth | Schmuth | Ritter | Weise |
|---|
| SI (mm)32 | Anterior arch width | 40 | 37.5 | 40 | 38 | 38.2 |
| Posterior arch width | 50 | 49 | 48 | 50 | 50.8 |
Si= Sum of incisors.
Numerous treatment modalities have been recommended to expand the maxillary arch [9]. Orthodontic effects include tooth tipping and bodily movement of the maxillary posterior teeth and the canines. Midpalatal suture opening is the skeletal response to maxillary expansion, particularly in young patients [10]. However, if applied to adult patients, the possibility of successful palatal expansion is decreased, because the sutures have a more interdigitated form and greater resistance to mechanical forces [11]. In most of the patients with posterior crossbite, varying degrees of skeletal component occurs. In adults, when skeletal growth is nearly complete, minor skeletal malocclusions can be camouflaged by orthodontic treatment alone.
Two basic approaches have been developed to expand the maxilla. Rapid maxillary expansion generates large forces to exceed the limits of orthodontic tooth movement, this produces maximum orthopaedic repositioning and affects the circum-maxillary suture system and more specifically, the mid-palatal suture [12] and slow maxillary expansion maintains sutural integrity during expansion, producing a more stable result than rapid maxillary expansion [13]. Slow expansion is commonly accomplished with removable expansion plates or fixed wire appliances such as the W-arch or the quad-helix. The quad-helix provides primarily buccal translation of the molars and does not require patient compliance. It has been reported to be highly successful in correcting crossbites in most of the cases [14-16]. Most of the expansion obtained is due to dental movement. Reported ratios of orthodontic to orthopedic effects range between 6:1 and 10:1 [17-18]. Considering age of the patient along with all the beneficial effects of quad helix, this appliance was chosen for expanding the maxilla in this case.
For the correction of Class III occlusal relation, Class III elastics were used. The effects like protraction of maxillary complex along with maxillary incisors and further retroclination of mandibular incisors resulted because of the use of Class III elastics. As the treatment was non-surgical and involved non-extraction method, there was no change in soft tissue facial profile of patient.
Conclusion
This case demonstrates that the use of a quad helix appliance with fixed appliance therapy along with the use of Class III elastics can be an effective method to camouflage the mild skeletal Class III cases with bilateral posterior cross bite.
Si= Sum of incisors.
[1]. Santos RLD, Pithon MM, Mechanical evaluation of quad-helix appliance made of low-nickel stainless steel wireDental Press J Orthod 2013 18(3):35-38. [Google Scholar]
[2]. Proffit WR, Fields HW Jr, Contemporary Orthodontics 2000 3rd edSt LouisMosby [Google Scholar]
[3]. Janson G, De Souza JEP, Alves FA, Andrade Jr P, Nakamura A, De Freitas MR, Extreme dentoalveolar compensation in the treatment of Class III malocclusionAm J Orthod Dentofacial Orthop 2005 128:787-94. [Google Scholar]
[4]. Harrison JE, Ashby D, Orthodontic treatment for posterior crossbitesCochrane Database of Systematic Reviews 2000 1:CD000979 [Google Scholar]
[5]. Andrade Ada S, Gameiro GH, Derossi M, Gavião MB, Posterior crossbite and functional Changes: A systematic reviewAngle Orthod 2009 79:380-86. [Google Scholar]
[6]. Erdinc A, Ugur T, Erbay E, A comparison of different treatment techniques for posterior crossbite in the mixed dentitionAm J Orthod Dentofacial Orthop 1999 116:287-300. [Google Scholar]
[7]. Bjerklin K, Follow-up control of patients with unilateral posterior cross-bite treated with expansion plates or the quad-helix applianceJ Orofac Orthop 2000 61:112-24. [Google Scholar]
[8]. Rakosi T, Jonas I, Graber TM, Orthodontic Diagnosis. In: Rateitschak KH, Wolf HF, editorsColor Atlas of Dental Medicine 1992 New YorkThieme Medical Publishers Inc:210 [Google Scholar]
[9]. Yaseen SM, Acharya R, Hexa helix: Modified quad helix appliance to correct anterior and posterior crossbites in mixed dentitionCase Rep Dent 2012 2012:860385 [Google Scholar]
[10]. Handelman CS, Wang L, BeGole EA, Haas AJ, Nonsurgical rapid maxillary expansion in adults: Report on 47 cases using the Haas expanderAngle Orthod 2000 70:129-44. [Google Scholar]
[11]. Takeuchi M, Tanaka E, Nonoyama D, Aoyama J, Tanne K, An adult case of skeletal open bite with a severely narrowed maxillary dental archAngle Orthod 2002 72:362-70. [Google Scholar]
[12]. Baldini A, Nota A, Santariello C, Assi V, Ballanti F, Cozza P, Influence of activation protocol on perceived pain during rapid maxillary expansionAngle Orthod 2015 85:1015-20. [Google Scholar]
[13]. Wong CA, Sinclair PM, Keim R G, Kennedy DB, Arch dimension changes from successful slow maxillary expansion of unilateral posterior crossbiteAngle Orthod 2011 81:616-23. [Google Scholar]
[14]. Petren S, Bondemark L, Correction of unilateral posterior crossbite in the mixed dentition: A randomized controlled trialAm J Orthod Dentofacial Orthop 2008 133:790.e7-13. [Google Scholar]
[15]. Vizzotto MB, de Araujo FB, da Silveira HS, Boza AA, Closs LQ, The quad-helix appliance in the primary dentition-orthodontic and orthopedic measurementsJ Clin Pediatr Dent 2007 32:165-70. [Google Scholar]
[16]. Bell RA, LeCompte EJ, The effects of maxillary expansion using a quad-helix appliance during the deciduous and mixed dentitionsAm J Orthod 1981 79:152-61. [Google Scholar]
[17]. Boysen B, La Cour K, Athanasiou AE, Gjessing PE, Three-dimensional evaluation of dentoskeletal changes after posterior cross-bite correction by quad-helix or removable appliancesBr J Orthod 1992 19:97-107. [Google Scholar]
[18]. Frank SW, Engel GA, The effects of maxillary quad-helix appliance expansion on cephalometric measurements in growing orthodontic patientsAm J Orthod 1982 81:378-89. [Google Scholar]