Case Report
A 22-year-old man was referred to the Department of Oral and Maxillofacial Surgery with a chief complaint of heaviness on the left side of the face, mild headache and intermittent dull pain in the left side of the face and in front of the left ear.
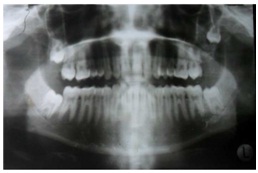
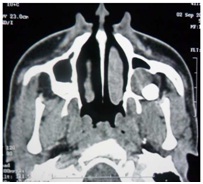
Intraoral examination revealed absence of left maxillary third molar. Panoramic radiograph revealed that the tooth was placed much higher in the sinus along the posterolateral wall [Table/Fig-1]. On Computed Tomography (CT) imaging the tooth was found to be partially in the maxillary sinus and partially in the infratemporal fossa, communicating through the posterolateral wall of maxillary sinus, lateral to the lateral pterygoid plate [Table/Fig-2].
Pre-operative OPG showing impacted tooth with cystic lining.
CT scan showing a unilateral unilocular well-defined corticated hypodense lesion.
The patient was admitted for surgery under General Anesthesia (GA) after thorough physical examination and routine blood investigations. Prior to the surgery a duly signed written informed consent was obtained from the patient.
The Caldwell Luc operation, originally described in the late 1800s, is an approach to the anterior wall of the maxillary sinus by making a window just below the canine fossa and the anterior wall is breached [1], but in the present case we had to modify this approach as the tooth was located posteriorly in the sinus, so a vestibular incision was given starting from tooth #23 till 1cm distally to tooth #27. A full thickness mucoperiosteal flap was reflected. The posterior part of the anterior wall of the maxillary sinus was breached by making a window by rosette round bur along with a 4mm chisel and bone rongeur, over teeth #26 and 27, the lateral wall was also resected till the posterolateral wall was approached [Table/Fig-3]. The tooth was found in the posterolateral aspect of the maxillary sinus and infra-temporal fossa, guttering of the bone was done around the tooth, distal retractor was used and the tooth was retrieved along with the cystic lining with the help of a curette [Table/Fig-4]. Post-operative recovery was uneventful; the patient was prescribed analgesics and antibiotics. He was followed up for three months and found to have no complaints.
Intra-operative image showing a window for Caldwell Luc procedure.

Specimen post dis-impaction.

Discussion
The term “dentigerous cyst” was coined by Paget in 1853; literal meaning of dentigerous is “tooth bearing”. After radicular cyst, dentigerous cyst is the second most common cystic lesion of the jaw. The theory behind the pathogenesis of this cyst is the accumulation of fluid between an unerupted tooth and the surrounding reduced enamel epithelium [2-4]. The association of dentigerous cyst to ectopic maxillary third molar that is partially in the maxillary sinus and partially in infratemporal fossa is rare and a proper surgical planning is necessary for its treatment.
The dis-impaction surgeries for maxillary third molar are among the most common procedure performed by Oral and Maxillofacial Surgeons [5-7]. The complications associated with removal of impacted maxillary third molar are fracture of tuberosity, tooth root fracture, perforation of the maxillary sinus, prolapsed buccal pad of fat and displacement of root into maxillary sinus [7,8]. Other possible complications include alveolar ostitis, infection, dysesthesia, hemorrhage, trismus, facial swelling and bruising, orofacial pain and the anesthetic difficulty [9]. According to literature the most ectopic position of maxillary third molar is the maxillary sinus or infratemporal fossa, pterygopalatine fossa, lateral pharyngeal space, ptergomandibular space, buccal space, where it gets positioned either iatrogenically or de novo [7,8,10,11].
However, this is the first reported case of an impacted maxillary third molar associated with a dentigerous cyst that was found de novo, located partially in the maxillary sinus and was communicating with anterosuperior part of the infratemporal fossa through the postero-lateral wall of maxillary sinus. The surgical procedure that was used was a modified Caldwell Luc operation, the importance of the radiological analysis prior to removal of the third molar has also been stated and the different surgical treatment options are described.
Ectopic tooth are those which are located in the jaw bones or region other than the alveolar arch. Ectopic eruption of a tooth is rare; however, there have been few reports of the tooth in nose, mandibular condyle, coronoid process, maxillary sinus, ptery-gopalatine fossa, infratemporal space, bucca space and lateral pharyngeal space [12-15].
Ectopic eruption of tooth may occur due to disturbance in the developmental process i.e., disturbance related to the tooth development [16], pathological process or iatrogenic activity.
Dentigerous cyst is the most common follicular cyst. Dentigerous cyst is usually present in the third and fourth decade and is rare in childhood, although few cases in childhood have been reported. Males have a higher incidence than females (M:F – 1.84 :1), 70% of dentigerous cyst occurs in the mandible and 30% in the maxilla [16,17]. Teeth which are mostly associated are mandibular third molar, maxillary canine, maxillary third molar [18-20].
Dentigerous cysts have been reported with syndromes such as basal cell nevus syndrome, mucopolysachhroidosis and cleido cranial dysplasia [21,22].
Dentigerous cyst is a slow progressing lesion and it may produce symptoms after several years. When the maxillary sinus and infratemporal fossa is involved the patient can have symptoms like headache [23], obstruction of the sinus [24], epiphora due to nasolacrimal duct obstruction [25], recurrent sinusitis, purulent rhinorhea [16], elevation of the orbital floor [26] and fracture of the sinus [27], patient sometimes also complains of diplopia and rarely blindness can also occur [28].
On radiographic examination, dentigerous cyst appears as a unilocular radiolucency of varying sizes with a well defined sclerotic border which is associated with a crown of an unerupted tooth. When a cyst is smaller in size it is difficult to differentiate a dentigerous cyst from a large but normal dental follicle. Dentigerous cyst is suspected when the distance between the crown and dental follicle is greater than 2.5mm–3.0 mm [29].
Water’s view, OPG, lateral cephalograph can help in radiographic evaluation of ectopic tooth in maxillary sinus and infratemporal fossa, CT scan and MRI have proved to give better image quality and diagnostic accuracy over conventional radiographs as it can help to visualize the ectopic tooth in its actual place [27,30].
The differential diagnosis of a dentigerous cyst includes unicystic ameloblastoma, adenomatoid odontogenic tumor, early stages of gorlin cyst/CEOT, odontogenic keratocyst, ameloblastic fibroma, fibro-odotoma [31].
Histologically, dentigerous cyst is lined by a layer of non-keratinized stratified squamous epithelium with surrounding walls of thin connective tissue containing odontogenic epithelial rest. There are cases in literature where the lining epithelium of dentigerous cyst develops into ameloblastoma or epidermoid carcinoma or squamous cell carcinoma [32,33].
Enucleation and extraction of the associated tooth via Caldwell Luc procedure is followed for a dentigerous cyst in maxillary sinus. In large cyst initial marsupialisation, followed by enucleation and tooth extraction has been advocated [2].
Endoscopic approach for its management has also been done, piezoelectric surgery is another modern approach for management of such cases [2].
In the present case the conventional Caldwell Luc procedure was modified. A window was made more posteriorly that could facilitate visualization and retrieval of the maxillary third molar which was partially in the maxillary sinus and partially in the infratemporal fossa.
Numerous surgical approaches to the infratemporal region can be used for the removal of impacted teeth such as Coronal, Gille’s temporal approach, Caldwell Luc or resection of coronoid process [5-7,34-36].
Adequate flap design and proper retrieval technique can prevent the displacement towards the base of the skull, no effort should be made to retrieve the tooth as it could result into major complication like hemorrhage, neurological injuries because many vital structures are present nearby like branch of mandibular nerve, otic ganglion, chorda tympani nerve, maxillary artery, pterygoid venus plexus [6,37].
Wrinkle T et al., in 1977 reported a case in which a maxillary third molar was inside the maxillary sinus and the tooth was removed via transantral approach, but when the patient was evaluated after six months, patient complained of persistent diplopia on upward and downward gaze [38].
Oberman M et al., 1986 reported a case of an attempted removal via an introral approach in which despite removal of the laterosuperior portion of the antral wall and part of the malar bone, the tooth could not been located [34].
Gulbrandsen SR et al., used a combined intraoral and hemicoronal approach and successfully removed the tooth from the infratemporal fossa [5].
Dawson K et al., reported the successful removal of maxillary third molar from infratemporal fossa by a temporal approach and the aid of image intensifying cineradiography [6].
Lipa Bodener et al., and Selvi F et al., successfully retrieved maxillary third molar via extended intraoral approach under local anesthesia [39,40].
Conclusion
Occurence of an ectopic tooth partially in the maxillary sinus and partially in the infratemporal fossa and associated dentigerous cyst is a rare phenomenon. It may be asymptomatic initially but later on symptoms may arise, so an early diagnosis and treatment is necessary to prevent morbidity. Imaging studies like plain film radiography as well as CT Scan aid in the diagnosis of ectopic tooth associated with dentigerous cyst, histopathologic feature help to confirm the diagnosis.
Modified Caldwell Luc procedure along with enucleation and primary closure was followed in this case as the tooth was partially located in maxillary sinus and partially in infratemporal fossa, but the treatment modality mostly depends on a surgeon’s preference, uniqueness of each case and patients psycological condition.
[1]. Stammberger H, Posawetz W, Functional endoscopic sinus surgery. Concept indications and results of the Messerklinger techniqueEur Arch Otorhinolaryngol 1990 247:63-76. [Google Scholar]
[2]. Di Pasquale P, Shermetaro C, Endoscopic removal of a dentigerous cyst producing unilateral maxillary sinus opacification on computed tomographyEar Nose Throat J 2006 85(11):747-48. [Google Scholar]
[3]. Tournas A, Tewfik M, Chauvin P, Manoukian J, Multiple unilateral maxillary dentigerous cysts in a nonsyndromic patient: A case report and review of the literatureInt J Pediatr Otorhi Extra 2006 1:100-06. [Google Scholar]
[4]. Browne RM, Smith AJ, Investigative Pathology of the Odontogenic Cyst 1991 New JerseyCRC Press Boca Raton:88-109.Pathogenesis of odontogenic cysts [Google Scholar]
[5]. Gulbrandsen S.R, Jackson I.T, Turlington E.G, Recovery of a maxillary third molar from the infratemporal space via a hemicoronal approachJ Oral Maxillofac Surg 1987 45:279 [Google Scholar]
[6]. Dawson K, MacMillan A, Wiesenfeld D, Removal of a maxillary third molar from the infratemporal fossa by a temporal approach and the aid of image-intensifying cineradiographyJ Oral Maxillofac Surg 1993 51:1395 [Google Scholar]
[7]. Sverzut CE, Trivellato AE, Sverzut AT, de Matos FP, Kato RB, Removal of a maxillary third molar accidentally displaced into infratemporal fossa via intraoral approach under local anesthesia: Report of a caseJOMS 2009 67(6):1316-20. [Google Scholar]
[8]. Dimitrakopoulos I, Papadaki M, Displacement of a maxillary third molar into the infratemporal fossa: Case reportQuentencence Int 2007 38(7):607-10. [Google Scholar]
[9]. Brauer HU, Unusual complications associated with third molar surgery: a systematic reviewQuintenence Int 2009 40(7):565-72. [Google Scholar]
[10]. Patel M, Down K, Accidental displacement of impacted maxillary third molarsBr Dent J 1994 177(2):57-59. [Google Scholar]
[11]. Özer N, Üçem F, Saruhanoğlu A, Yilmaz S, Tanyeri H, Removal of a maxillary third molar displaced into pterygopalatine fossa via intraoral approachCase Reports in Dentistry 2013 Article ID 392148, 4 pages, 2013 [Google Scholar]
[12]. I-Hung Lin, Chung-Feng Hwang, Chih-Ying Su, Yi-Fen Kao, Jyh-Ping Peng, Intranasal tooth: Report of three casesChang Gung Med J 2004 27:385-89. [Google Scholar]
[13]. Yusuf A, Quayle AA, Intracondylar toothInternational Journal of Maxillofacial Surgery 1989 18(6):323 [Google Scholar]
[14]. Toranzo Fernandez M, Terrones Meraz MA, Infected cyst in the coronoid processOral Surg Oral Med Oral Pathol Oral Radiol Endod 1992 73(6):768 [Google Scholar]
[15]. Buyukkurt MC, Omezli MM, Miloglu O, Dentigerous cyst associated with an ectopic tooth in the maxillary sinus: A report of 3 cases and review of the literatureOral Surg Oral Med Oral Pathol Oral Radiol Endod 2010 109(1):67-71. [Google Scholar]
[16]. Prasad TS, Sujatha G, Niazi T M, Rajesh P, Dentigerous cyst associated with an ectopic third molar in the maxillary sinus: A rare entityIndian Journal of Dental Research 2007 18(3):141-43. [Google Scholar]
[17]. Pramod D S R, Shukla J N, Dentigerous cyst of maxilla in a young childNatl J Maxillofac Surg 2011 2(2):196-99. [Google Scholar]
[18]. Wang Chih Jen, Po-Hsien Huang, Yin-Lai Wang, Yih-Chung Shyng, Wen-Bin Kao, Dentigerous cyst over maxillary sinus: A case report and literature reviewTaiwan J Oral Maxillofac Surg 2009 20:116-24. [Google Scholar]
[19]. de Souza LB, Gordón-Núñez MA, Nonaka CF, de Medeiros MC, Torres TF, Emiliano GB, Odontogenic cysts: Demographic profile in a Brazilian population over a 38-year periodMed Oral Patol Oral Cir Bucal 2010 15(4):583-90. [Google Scholar]
[20]. Baykul T, Dogru H, Yasan H, Cina Aksoy M, Clinical impact of ectopic teeth in the maxillary sinusAuris Nasus Larynx 2006 33(3):277-81. [Google Scholar]
[21]. Robert M Barton, Barton NW, Constantopoulos G, Butler DP, Donahue AH, Occurrence of multiple dentigerous cysts in a patient with the Maroteaux-Lamy syndrome (mucopolysaccharidosis, type VI)Oral Surg Oral Med Oral Pathol 1984 58(2):169-75. [Google Scholar]
[22]. Trimble L D, West RA, McNeill RW, Cleidocranial dysplasia: comprehensive treatment of the dentofacial abnormalitiesJ Am Dent Assoc 1982 105(4):661-66. [Google Scholar]
[23]. Freedland ES, Henneman PL, An unusual cause of headache: A dentigerous cyst in the maxillary sinusAnn Emerg Med 1987 16:1174-76. [Google Scholar]
[24]. Litvin M, Caprice D, Infranco L, Dentigerous cyst of the maxilla with impacted tooth displaced into orbital rim and floorEar Nose Throat J 2008 87(3):160-62. [Google Scholar]
[25]. Ray B, Bandyopadhyay SN, Das D, Adhikary B, A rare cause of nasolacrimal duct obstruction: Dentigerous cyst in the maxillary sinusIndian J Ophthalmol 2009 57(6):465-67. [Google Scholar]
[26]. Golden AL, Foote J, Lally E, Beideman R, Tatoian J, Dentigerous cyst of the maxillary sinus causing elevation of the orbital floor- report of a caseOral Surg Oral Med Oral Pathol 1981 52(2):133-36. [Google Scholar]
[27]. Han MH, Chang KH, Lee CH, Na DG, Yeon KM, Han MC, Cystic expansile masses of the maxilla: Differential diagnosis with CT and MRAJNR Am J Neuroradiol 1995 16(2):333-38. [Google Scholar]
[28]. Savundranayagam A, Migratory third molar erupting into the lower border of orbit causing blindness in the left eyeAust Dent J 1972 17(6):418-20. [Google Scholar]
[29]. Guruprasad Y, Chauhan D S, Infected dentigerous cyst of maxillary sinus arising from an ectopic third molarJ Clin Imaging Sci 2013 3:7 [Google Scholar]
[30]. Bonder L, Tovi F, Bar-Ziv J, Teeth in the maxillary sinus -imaging and managementJ Laryngol Otol 1997 111(9):820-24. [Google Scholar]
[31]. Mahesh KR, Umashankar DN, Nandakumar H, Radhika BM, Sudhakar Inflammatory variant of dentigerous cyst in maxillary sinus-A case reportInt J Oral Maxillofac Pathol 2010 1:17-19. [Google Scholar]
[32]. Rajendran R, Cysts and Tumors of Odontogenic Origin. In: Rajendran R, Sivapathasundharam B, editorsShafer’s Textbook of Oral Pathology 2006 5th edNew DelhiElsevier Publishers:360-1. [Google Scholar]
[33]. Yasuoka T, Yonemoto K, Kato Y, Tatematsu N, Squamous cell carcinoma arising in a dentigerous cystJ Oral Maxillofac Surg 2000 58:900-05. [Google Scholar]
[34]. Oberman M, Horowitz I, Ramon Y, Accidental displacement of impacted maxillary third molarsInt J Oral Maxillofac Surg 1986 15:756-58. [Google Scholar]
[35]. Gómez-Oliveira G, Arribas-García I, Alvarez-Flores M, Gregoire-Ferriol J, MartínezGimeno C, Delayed removal of a maxillary third molar from the infratemporal fossaMed Oral Patol Oral Cir Bucal 2010 15(3):509-11. [Google Scholar]
[36]. Sverzut CE, Trivellato AE, Lopes LMF, Ferraz EP, Sverzut AT, Accidental displacement of impacted maxillary third molar: a case reportBraz Dent J 2005 16(2):167-70. [Google Scholar]
[37]. Moore Keith L, Dalley Arthur, Clinically oriented anatomy 2006 5th edLippincott Williams & Wilkins [Google Scholar]
[38]. Winkler T, von Wowern N, Bittlmann S, Retrieval of an upper third molar from the infratemporal spaceJournal of Oral Surgery 1977 35:130-32. [Google Scholar]
[39]. Lipa Bodnera, Ben Zion Joshuab, Max B, Puterman. Removal of a maxillary third molar from the infratemporal fossaJ Med Cases 2012 3(2):97-99. [Google Scholar]
[40]. Selvi F, Cakarer S, Keskin C, Ozyuvaci H, Delayed removal of a maxillary third molar accidentally displaced into the infratemporal fossaJ Craniofac Surg 2011 22(4):1391-93. [Google Scholar]